Page 4 of 38
OG12.2 | Anaemia in Pregnancy — SDL Guide
Learning Objectives
- Define anaemia in pregnancy and classify it by aetiology and severity using WHO criteria
- Describe the pathophysiology of iron deficiency anaemia in pregnancy including physiological anaemia
- Identify clinical features, investigations and diagnostic criteria for anaemia in pregnancy
- Explain the adverse effects of anaemia on the mother and foetus
- Outline the management of anaemia in pregnancy including prophylaxis, oral/parenteral iron, and transfusion
INSTRUCTIONS
Anaemia complicates approximately 50% of all pregnancies in India and is a leading indirect cause of maternal mortality. This module uses the OG disease arc to take you from recognising the clinical presentation through to evidence-based management, with a focus on the thresholds and drug choices that are tested in clinical exams and applied at the bedside.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Chapter 14 (textbook)
- Williams Obstetrics, 26th edition, Chapter 56 (textbook)
- WHO Guideline: Daily iron and folic acid supplementation during pregnancy, 2012 (guideline)
- NHM — Iron and Folic Acid Supplementation Programme, India (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Meena, a 24-year-old primigravida at 32 weeks gestation, attends her antenatal clinic looking pale and breathless on minimal exertion. She has been taking iron tablets irregularly because they cause nausea. Her haemoglobin is 6.2 g/dL, heart rate 108 beats/min, and she has bilateral pedal oedema. Her baby's growth on ultrasound is below the 10th centile. The obstetrician faces an urgent decision: can she safely reach term, how should her anaemia be corrected, and how will labour be managed? The answers hinge on understanding why anaemia in pregnancy matters so profoundly — for both mother and baby.
WHY THIS MATTERS
Anaemia in pregnancy is not merely a laboratory finding; it is a direct driver of maternal and perinatal mortality in low- and middle-income countries. India contributes disproportionately to the global burden, with national surveys (NFHS-5, 2019-21) showing that approximately 52% of pregnant women are anaemic. Severe anaemia (haemoglobin below 7 g/dL) increases the risk of cardiac failure, postpartum haemorrhage, puerperal sepsis, and maternal death. On the foetal side, anaemia is the most preventable cause of intrauterine growth restriction and low birth weight. For the practising obstetrician, identifying, classifying, and correcting anaemia is a core clinical competency: the threshold at which you choose parenteral iron over oral tablets, or packed cells over parenteral iron, is precisely the knowledge this module builds.
RECALL
Before we explore anaemia in pregnancy, recall from your physiology and biochemistry courses: the normal haemopoiesis pathway produces erythrocytes dependent on iron, vitamin B12, and folate; iron is absorbed in the ferrous (Fe²⁺) form from the duodenum and jejunum, facilitated by gastric acid and vitamin C, and transported by transferrin to the bone marrow; ferritin is the storage form. In a non-pregnant woman the daily iron requirement is approximately 1–2 mg. You should also remember that folate requirements double during rapid cell division — relevant because foetal growth accelerates this further. Keeping these mechanisms in mind will help you understand why pregnancy dramatically outstrips routine dietary intake.
Clinical Presentation of Anaemia in Pregnancy
Anaemia in pregnancy is defined by the World Health Organization (WHO) as a haemoglobin (Hb) concentration below 11 g/dL at any trimester of pregnancy. This threshold is lower than the non-pregnant female value of 12 g/dL because pregnancy causes physiological haemodilution — plasma volume expands by 40–50%, while red cell mass expands by only 20–30%, producing a dilutional fall in Hb that is normal and expected. The distinction between physiological haemodilution and true pathological anaemia is an important clinical judgment: a woman at 28 weeks with Hb 10.5 g/dL and a healthy peripheral smear may simply reflect normal dilution, whereas the same value with a microcytic hypochromic smear signals iron deficiency.
Clinically, pregnant women with anaemia present along a severity spectrum. Mild anaemia (Hb 10–10.9 g/dL) often produces no symptoms; it is detected only on routine antenatal screening. Moderate anaemia (Hb 7–9.9 g/dL) produces fatigue, exertional breathlessness, palpitations, easy fatigability, and mild pallor of the conjunctiva, tongue, and nail beds. Severe anaemia (Hb below 7 g/dL) causes resting dyspnoea, tachycardia, ankle oedema from a high-output state, and marked pallor; patients with haemolytic or haemorrhagic aetiology may be jaundiced. Very severe anaemia (Hb below 4 g/dL) is a medical emergency: congestive cardiac failure, pulmonary oedema, and imminent maternal collapse are immediate risks.
The epidemiological burden in India is staggering: the National Family Health Survey-5 (2019–21) reported that 52% of pregnant women aged 15–49 years are anaemic. Nutritional deficiency — primarily iron deficiency — accounts for approximately 95% of all anaemia in pregnancy in India, making it the dominant clinical problem in antenatal care. The remaining 5% includes folate/B12 deficiency, haemolytic anaemias (malaria, sickle cell, thalassaemia), and rare aplastic anaemia.
Provided image
On examination, key signs include conjunctival pallor (reliable below Hb 9 g/dL), pallor of the tongue and nail beds, koilonychia (spoon-shaped nails in iron deficiency), angular stomatitis, glossitis, and tachycardia. Fundal examination may reveal tortuous retinal vessels in severe chronic anaemia. Oedema, raised jugular venous pressure, and basal crepitations suggest cardiac decompensation.
Pathophysiology and Aetiology
Understanding why pregnancy generates a near-universal iron deficit requires tracing the simultaneous demands placed on maternal iron stores across all three trimesters. During a singleton pregnancy, the total additional iron requirement is estimated at 700–1000 mg: approximately 300 mg for foetal and placental development, 500 mg for expansion of the maternal red cell mass, and 200 mg to replace basal daily losses. The average Indian woman enters pregnancy with iron stores of only 200–300 mg — barely sufficient even for basal needs. When dietary intake (typically 10–15 mg/day with only 10% absorption) cannot bridge this deficit, iron deficiency develops and erythropoiesis becomes iron-restricted.
The sequence of iron deficiency progresses through three stages: first, iron depletion (falling serum ferritin, stores emptying); second, iron-deficient erythropoiesis (falling serum iron, rising TIBC, falling transferrin saturation, reticulocytes diminish); and third, frank iron deficiency anaemia (microcytic, hypochromic red cells; Hb falls below the WHO threshold of 11 g/dL). In practice, pregnant women often present at stage three because symptoms are insidious and early stages are asymptomatic.
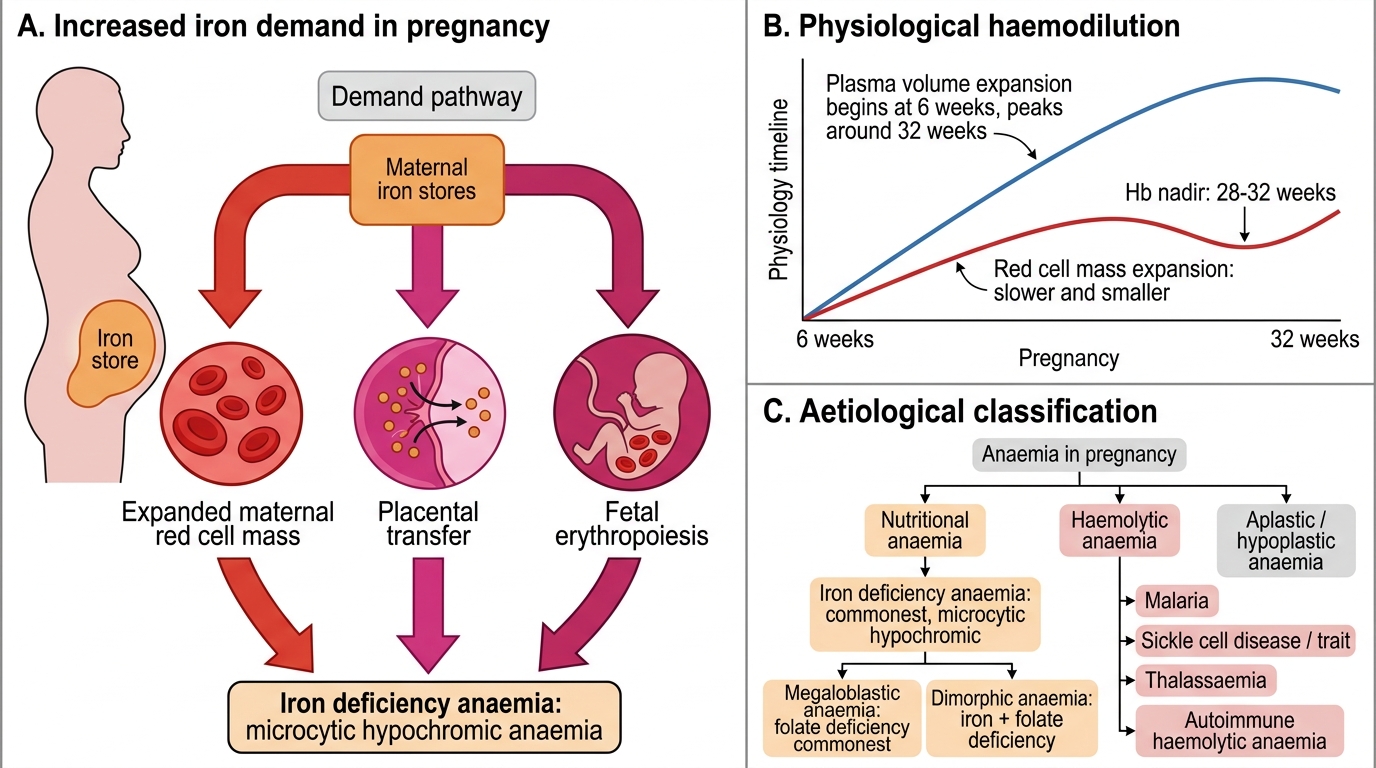
Increased Iron Demand and Anaemia in Pregnancy
Classification by aetiology:
• Nutritional anaemia (most common — 95% in India):
- Iron deficiency anaemia (IDA): microcytic hypochromic; commonest cause; inadequate diet, poor absorption, recurrent infections (especially hookworm)
- Megaloblastic anaemia: macrocytic; folate deficiency (commonest megaloblastic cause in pregnancy — foetal and placental demands deplete folate rapidly) or rarely vitamin B12 deficiency
- Dimorphic anaemia: mixed iron + folate deficiency producing a mixed microcytic/macrocytic picture
• Haemolytic anaemia:
- Malaria: leading cause of haemolytic anaemia in endemic regions; also suppresses bone marrow
- Sickle cell disease / trait: more frequent crises in pregnancy; HbSS carries high perinatal mortality
- Thalassaemia: β-thalassaemia major presents before reproductive age; β-thalassaemia minor is the common carrier state detected incidentally
- Autoimmune haemolytic anaemia: rare in pregnancy
• Aplastic / hypoplastic anaemia: rare; idiopathic or drug-induced; poor prognosis for mother and foetus
Physiological anaemia of pregnancy must be differentiated from pathological anaemia. Plasma volume expansion begins at 6 weeks and peaks at 32 weeks; red cell mass expansion is slower and smaller, resulting in a nadir Hb around 28–32 weeks. This is NORMAL. A low Hb in a woman with a normal peripheral smear, normal MCV, normal iron studies, and no symptoms beyond fatigue represents physiological haemodilution, not iron deficiency, and should NOT trigger iron treatment beyond routine prophylaxis.
Investigations and Diagnosis
A systematic investigation approach is essential both to confirm the presence of anaemia and — critically — to identify its type, because the treatment differs fundamentally between iron deficiency, megaloblastic anaemia, and haemolytic disease.
The first-line investigation is a Complete Blood Count (CBC) with peripheral blood smear. The CBC provides Hb, haematocrit (PCV), red cell indices (MCV, MCH, MCHC, RDW), total white cell count, and platelet count. Mean Corpuscular Volume (MCV) is the key discriminator: MCV below 80 fL = microcytic (IDA, thalassaemia); MCV 80–100 = normocytic (early IDA, haemolytic, aplastic, anaemia of chronic disease); MCV above 100 fL = macrocytic (megaloblastic).
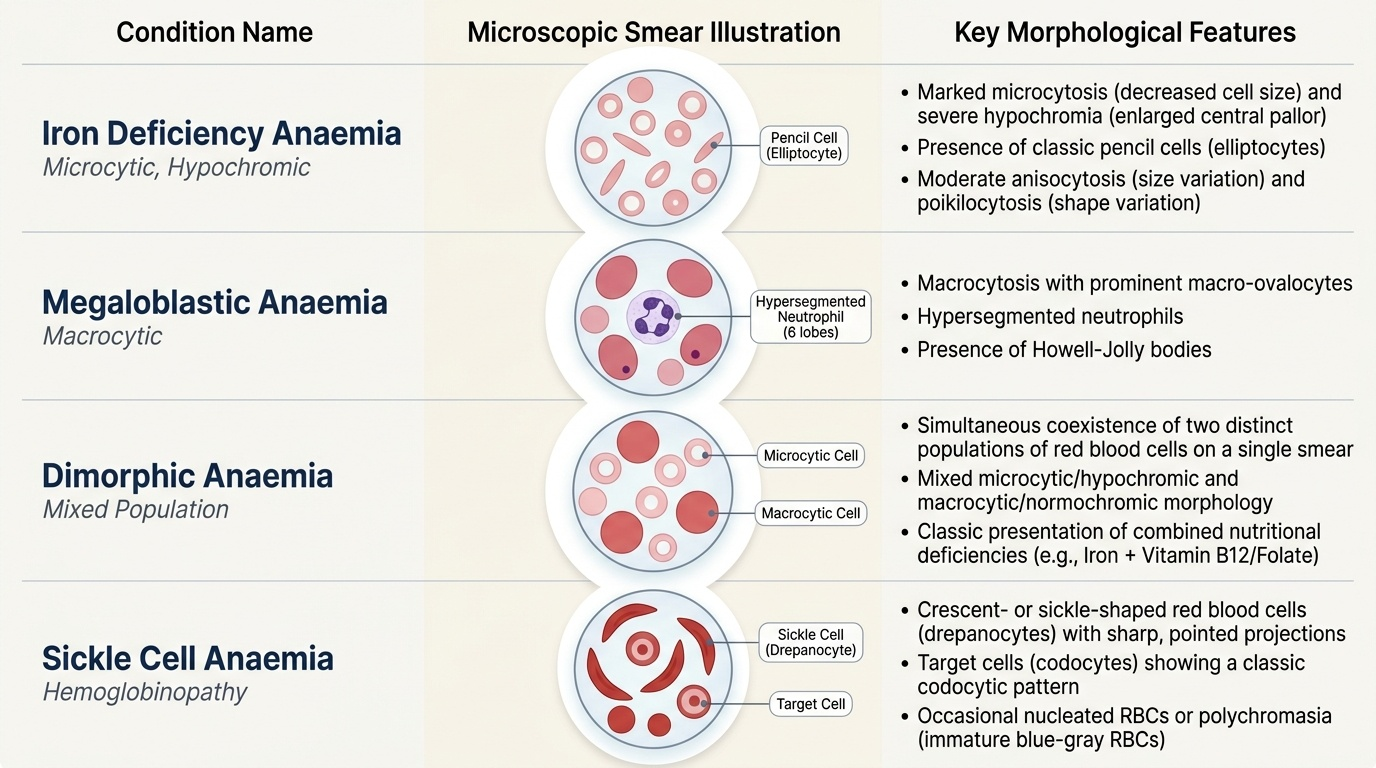
The peripheral blood smear adds morphological detail that the indices cannot fully capture, translating numerical values into visually recognisable patterns of red cell size, shape, and chromasia that directly reflect the underlying deficiency state:
- Iron deficiency: microcytic, hypochromic cells; pencil cells (elliptocytes); anisocytosis and poikilocytosis; high RDW
- Megaloblastic: macro-ovalocytes, hypersegmented neutrophils (≥5 lobes in ≥5% cells), elevated MCV; Howell-Jolly bodies in severe disease
- Dimorphic: mixed microcytic and macrocytic population; bimodal distribution
- Sickle cell: sickle-shaped erythrocytes, target cells, Howell-Jolly bodies
- Haemolytic: fragmented cells (schistocytes), spherocytes depending on cause
Iron studies provide definitive diagnosis of the type:
| Parameter | Iron Deficiency Anaemia | Anaemia of Chronic Disease | Megaloblastic |
|---|---|---|---|
| Serum iron | Low | Low | Normal/High |
| TIBC | High (>360 µg/dL) | Low/Normal | Normal |
| Serum ferritin | Low (<12 ng/mL) | Normal/High | Normal |
| Transferrin saturation | Low (<16%) | Low | Normal |
| RBC folate | Normal | Normal | Low |
Serum ferritin is the single best test for iron deficiency in pregnancy (below 12 ng/mL = depleted stores; below 30 ng/mL = probable deficiency in pregnancy context). However, ferritin is an acute-phase reactant and rises falsely in infection/inflammation — interpret with clinical context.
Additional investigations depending on clinical suspicion:
- Serum folate and vitamin B12: if MCV elevated or dimorphic picture
- Reticulocyte count: elevated in haemolytic anaemia; low in aplastic or nutritional
- Direct Coombs test (DAT): for autoimmune haemolysis
- Haemoglobin electrophoresis: if sickle cell or thalassaemia suspected (family history, Mediterranean/African origin, abnormal smear)
- Malarial parasite (MP) smear: thick and thin smear if febrile or in endemic area
- Urine microscopy: to exclude haematuria or haemoglobinuria
- Bone marrow examination: rarely needed; reserved for suspected aplastic anaemia or diagnostic uncertainty after full workup
Routine antenatal screening should include Hb measurement at booking (first visit), 28 weeks, and 36 weeks, supplemented by peripheral smear if Hb is below 11 g/dL.
SELF-CHECK
A 28-week primigravida has Hb 9.4 g/dL, MCV 74 fL, low serum ferritin (8 ng/mL), and high TIBC. Her peripheral smear shows microcytic hypochromic cells with pencil cells. Which is the most likely diagnosis?
A. Physiological anaemia of pregnancy
B. Iron deficiency anaemia
C. Megaloblastic anaemia
D. Anaemia of chronic disease
Reveal Answer
Answer: B. Iron deficiency anaemia
Iron deficiency anaemia (IDA) is characterised by microcytic (low MCV), hypochromic cells on smear, low serum ferritin (depleted stores), and elevated TIBC (the body upregulates transferrin to capture more iron). Physiological anaemia has normal indices and normal iron studies. Megaloblastic anaemia has macrocytic cells. Anaemia of chronic disease has low serum iron but NORMAL or LOW TIBC and NORMAL or HIGH ferritin.