Page 5 of 38
OG12.2 | Anaemia in Pregnancy — SDL Guide (Part 2)
Adverse Effects on Mother and Foetus
The consequences of untreated or poorly managed anaemia in pregnancy extend across the continuum from conception to the postnatal period, affecting both the mother and the developing foetus through distinct but interrelated pathways. Anaemia impairs oxygen delivery to every maternal organ system, and the body compensates by increasing cardiac output — a compensatory mechanism that is effective in mild anaemia but becomes pathological when sustained, or when the underlying heart has limited reserve. Simultaneously, the developing foetus depends entirely on the uteroplacental circulation for its oxygen and nutritional supply; when maternal haemoglobin is chronically low, placental oxygen delivery falls, foetal growth slows, and the risk of preterm labour rises as oxidative stress accumulates in the membranes and decidua. Understanding these dual pathways — maternal cardiovascular stress and foetal uteroplacental insufficiency — is essential for appreciating why correcting anaemia before the third trimester dramatically improves perinatal outcomes.
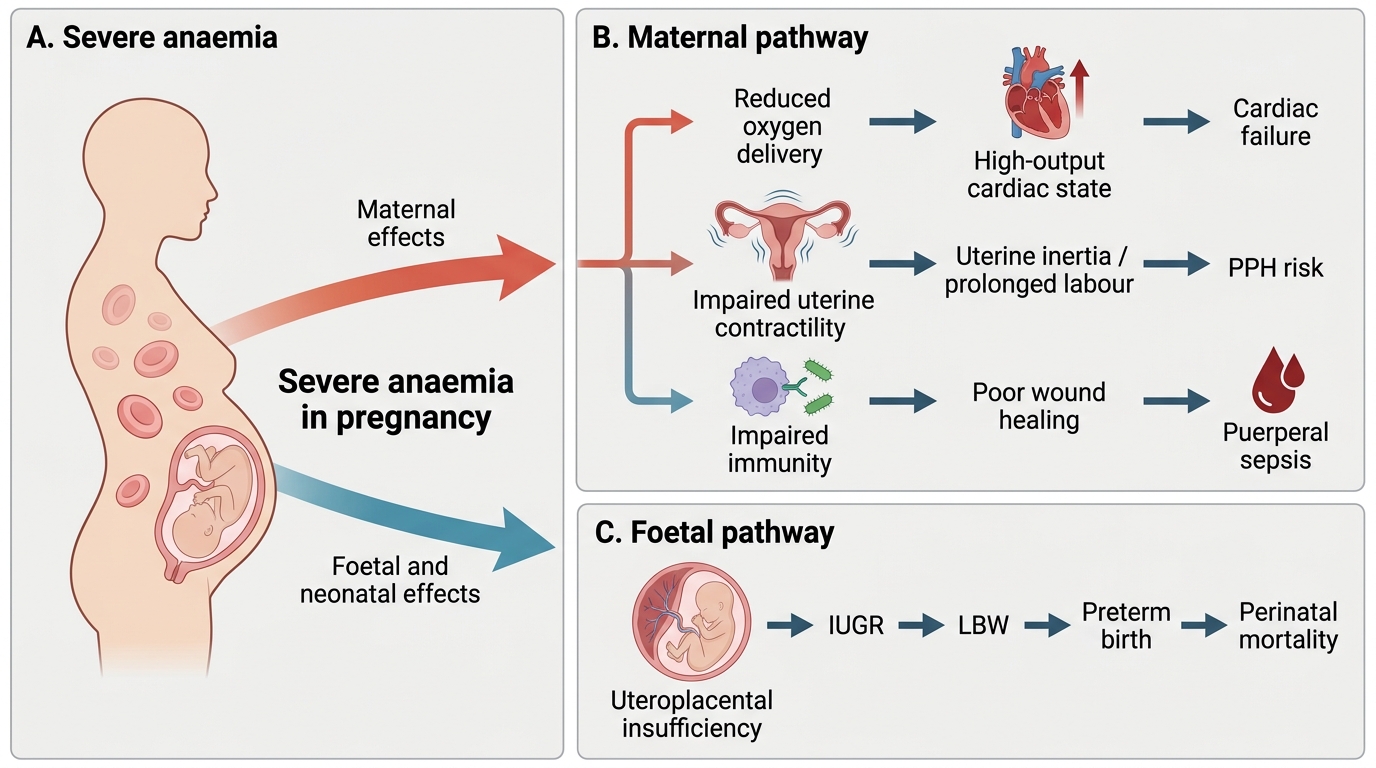
Adverse Effects of Severe Anaemia in Pregnancy
Maternal effects:
- During pregnancy: increased susceptibility to infections, impaired immunity, easy fatigability reducing work capacity, and exacerbation of pre-existing heart disease or gestational hypertension
- Cardiac stress: severe anaemia triggers a high-output cardiac state (compensatory rise in heart rate and stroke volume to maintain oxygen delivery); in women with underlying valvular disease or cardiomyopathy, this can precipitate cardiac failure
- Labour and delivery complications: impaired myometrial contractility (iron-dependent enzymes) increases the risk of uterine inertia and prolonged labour; pre-existing anaemia reduces the capacity to tolerate normal postpartum blood loss, so that even a physiological 300–500 mL loss may cause haemodynamic decompensation, effectively lowering the functional PPH threshold
- Postpartum: poor wound healing, increased risk of puerperal sepsis (anaemia impairs neutrophil function and bactericidal capacity), delayed recovery, increased risk of postnatal depression
- Anaesthetic risk: severe anaemia increases risk with both regional and general anaesthesia
Foetal and neonatal effects:
- Intrauterine growth restriction (IUGR): chronic uteroplacental hypoxia reduces foetal oxygen and nutrient supply, restricting foetal growth
- Preterm birth: the association with preterm labour is strongest in severe anaemia; proposed mechanisms include membrane oxidative stress and hormonal changes
- Low birth weight (LBW): both IUGR and preterm birth contribute; LBW neonates face increased neonatal morbidity and mortality
- Perinatal asphyxia: impaired placental oxygen reserve during labour contractions
- Iron deficiency in the neonate: while the foetus preferentially extracts iron from maternal serum, very severe maternal IDA depletes foetal stores, increasing infant risk of postnatal iron deficiency anaemia
- Stillbirth and perinatal mortality: risk rises steeply in severe (Hb <7 g/dL) and very severe (Hb <4 g/dL) anaemia
The severity-outcome gradient is important for clinical communication: a woman with Hb of 10 g/dL on treatment has a very different prognosis from a woman with Hb of 4.5 g/dL presenting in labour.
SELF-CHECK
Severe anaemia (Hb <7 g/dL) in the third trimester increases the risk of postpartum haemorrhage primarily because:
A. It causes placenta praevia
B. The woman cannot tolerate normal postpartum blood loss, lowering the functional PPH threshold
C. It directly causes uterine rupture
D. Anaemia causes premature rupture of membranes
Reveal Answer
Answer: B. The woman cannot tolerate normal postpartum blood loss, lowering the functional PPH threshold
PPH is defined as blood loss ≥500 mL after vaginal delivery (or ≥1000 mL after caesarean). A woman with severe anaemia who loses even a physiological 300–400 mL may develop haemodynamic compromise that would not occur in a well-haemoglobinised woman — effectively lowering her functional PPH threshold. Severe anaemia also impairs myometrial contractility (iron-dependent enzymes), which can contribute to uterine atony.
Management During Pregnancy and Labour
Management of anaemia in pregnancy follows a severity-tiered approach, anchored by the WHO/NHM threshold of Hb 11 g/dL as the diagnostic cut-off and targeting correction to 11 g/dL or above before delivery wherever possible. The underlying principle is that the earlier anaemia is identified and treated, the more time available for the least-invasive intervention — oral iron — to be effective; parenteral iron and blood transfusion are reserved for situations where oral therapy has failed, is contraindicated, or where delivery is too close to allow oral correction. Every management decision should simultaneously address the cause of the anaemia (nutritional replacement vs treatment of underlying infection vs transfusion), the prevention of labour-related bleeding complications, and the long-term nutritional health of the woman through the postpartum period. Prophylaxis through the National Health Mission IFA programme is the foundation, and all other interventions are layers on top of this baseline.
A. Prophylaxis (Prevention — all pregnant women)
The National Health Mission (NHM) Iron and Folic Acid (IFA) programme recommends universal supplementation for ALL pregnant women:
- Oral IFA: 60 mg elemental iron + 500 mcg folic acid daily throughout pregnancy and for 6 months postpartum
- Iron is best absorbed on an empty stomach or with vitamin C; gastric side effects (nausea, epigastric discomfort) are the main cause of non-adherence — counsel to take at bedtime if nausea occurs
- Dietary counselling: increase intake of iron-rich foods (green leafy vegetables, jaggery, animal protein) and vitamin C (citrus) to enhance absorption; avoid tea/coffee with meals (tannins reduce absorption)
- Deworming: single-dose albendazole 400 mg at 14–16 weeks reduces hookworm-related blood loss (major contributor to iron deficiency in rural India)
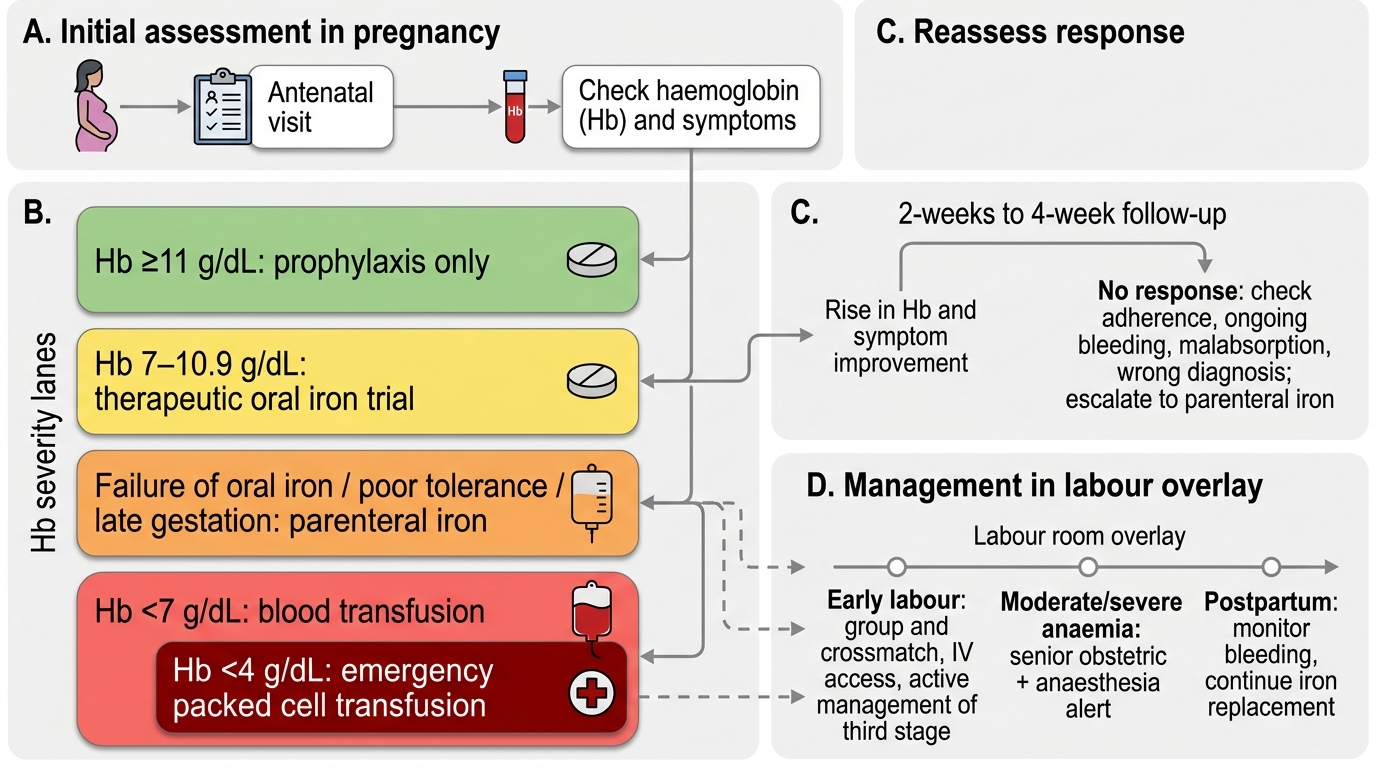
Anaemia Management Algorithm in Pregnancy
B. Oral Iron Therapy (Hb 7–10.9 g/dL)
- Ferrous sulphate 200 mg (= 60 mg elemental iron) thrice daily is the standard therapy
- Alternative salts: ferrous gluconate, ferrous fumarate — equivalent efficacy but differ in bioavailability and tolerability
- Expected response: reticulocytosis within 7–10 days; Hb rise of 0.8–1 g/dL per week; monitor at 4 weeks
- Continue for 3 months after Hb normalises to replenish iron stores
- Failure of oral iron (no rise in Hb after 4 weeks despite compliance): suspect non-compliance, malabsorption (hookworm, celiac), or incorrect diagnosis — reassess
C. Parenteral Iron (IV/IM) — Indications:
- Failure of oral iron despite adequate compliance and duration (4 weeks)
- Severe side effects from oral iron preventing adherence
- Severe anaemia (Hb <7 g/dL) requiring rapid correction, especially in the last 4–6 weeks of pregnancy when oral iron cannot achieve sufficient correction before delivery
- Malabsorption syndromes (inflammatory bowel disease, celiac)
- Ongoing blood loss exceeding the rate of oral replacement
Available preparations:
- Iron sucrose (IV): preferred in India; 200 mg in 100 mL normal saline over 30 minutes; total dose calculated by Ganzoni formula: Total deficit = Weight (kg) × (Target Hb − Actual Hb) × 2.4 + 500 mg (stores); administered in divided doses every 2–3 days; less anaphylaxis risk than older dextran preparations
- Iron dextran (IM — Z-track): older technique; more painful; risk of haematoma and anaphylaxis; less preferred
- Monitor: test dose recommended before iron sucrose infusion; observe for 30 minutes post-infusion; anaphylaxis management (adrenaline, antihistamines) must be available
D. Blood Transfusion — Indications:
- Hb <7 g/dL in the third trimester or when delivery is imminent and there is insufficient time for iron therapy
- Symptomatic anaemia regardless of Hb level (cardiac failure, severe dyspnoea at rest)
- Hb <4 g/dL (very severe) — emergency situation requiring immediate packed red cell transfusion regardless of gestational age
- Haemodynamic instability due to acute blood loss
- Packed red blood cells (PRBCs): each unit raises Hb by approximately 1 g/dL; transfuse slowly in severe anaemia with cardiac compromise (risk of fluid overload — consider concurrent frusemide)
E. Management in Labour:
- Women with Hb <7 g/dL should ideally have anaemia corrected before labour; if not possible, have blood cross-matched and available
- Active management of the third stage of labour (AMTSL) with oxytocin 10 IU IM immediately after delivery of the anterior shoulder — to minimise postpartum blood loss
- Vigilant for PPH — lower tolerance threshold for intervention
- Minimise blood loss during episiotomy and repair; ensure meticulous haemostasis
- Anaesthetic risk: inform anaesthetist; avoid excessive fluid loading; SpO₂ monitoring
- Antibiotics: prophylactic for operative deliveries (higher infection risk in anaemic patients)
F. Management of Specific Types:
- Megaloblastic anaemia: folic acid 5 mg/day oral (therapeutic dose, not the prophylactic 500 mcg); also correct vitamin B12 if deficient
- Malaria: antimalarial treatment per national protocol + iron/folate supplementation after parasite clearance
- Sickle cell disease: haematology co-management; folic acid supplementation mandatory; hydroxyurea generally avoided in pregnancy; exchange transfusion for crisis
- Thalassaemia minor: requires genetic counselling about foetal risk; oral folic acid; AVOID empirical IV iron (iron overload risk)
G. Postpartum management:
- Continue IFA supplementation for 6 months postpartum per NHM guidelines
- Check Hb at 6 weeks postpartum; reassess and treat persistent anaemia
- Breastfeeding support: iron passes to breast milk, contributing to infant iron stores
CLINICAL PEARL
The single most important clinical decision point in anaemia management is distinguishing severe IDA (Hb <7 g/dL) from moderate (Hb 7–10.9 g/dL): it determines whether you choose oral iron, parenteral iron, or blood transfusion. Remember also that thalassaemia minor patients should NOT receive empirical parenteral iron — iron overload in a patient who cannot export iron causes organ damage. Always check electrophoresis before parenteral iron if there is any suspicion of haemoglobinopathy. And never forget: the BEST outcome is prevention — every woman who completes her IFA course from booking is a woman whose Hb at 36 weeks will carry her safely through labour and the third stage.
SELF-CHECK
A 34-week primigravida with Hb 6.0 g/dL and iron deficiency anaemia failed 4 weeks of oral ferrous sulphate (confirmed compliance). The most appropriate next step is:
A. Switch to a different oral iron salt (ferrous gluconate)
B. Administer parenteral iron sucrose IV
C. Immediate caesarean section
D. Add folic acid 5 mg/day to her current oral iron
Reveal Answer
Answer: B. Administer parenteral iron sucrose IV
This patient has severe anaemia (Hb <7 g/dL) at 34 weeks with documented failure of oral iron. The indication for parenteral iron is clear: severe anaemia in the third trimester where oral therapy has failed and delivery is too close for oral therapy to correct haemoglobin sufficiently. Switching oral salts would not overcome the underlying absorption problem or the time constraint. Caesarean section is not indicated for anaemia alone. Adding folic acid would be appropriate for megaloblastic anaemia, not iron deficiency.
SELF-CHECK
The WHO definition of anaemia in pregnancy applies:
A. Only in the first trimester (Hb <12 g/dL)
B. To all trimesters: Hb <11 g/dL
C. Only after 20 weeks gestation: Hb <10 g/dL
D. Differently by trimester: <11 g/dL (1st), <10.5 g/dL (2nd), <11 g/dL (3rd)
Reveal Answer
Answer: B. To all trimesters: Hb <11 g/dL
WHO defines anaemia in pregnancy as Hb <11 g/dL, applicable uniformly across all three trimesters. This is the single threshold used in Indian national guidelines (NHM, ICMR). The second-trimester nadir (physiological haemodilution peak at 28–32 weeks) does not change the diagnostic threshold — only the interpretation of a borderline result with normal indices and normal iron studies, which may represent physiological haemodilution.
Self-Assessment
Having worked through the pathophysiology, investigations, adverse effects, and management of anaemia in pregnancy, it is now time to consolidate your learning through self-assessment. The questions and clinical scenarios that follow are designed to mirror the structured thinking required in a clinical encounter and in examination settings. When you encounter a pregnant woman with pallor, you should be able to move sequentially through the differential diagnosis of anaemia, order and interpret the correct investigations, grade severity using the WHO threshold of Hb below 11 g/dL, and select the appropriate intervention from the prophylaxis-oral-parenteral-transfusion hierarchy. Equally important is recognising the red flags: a woman with Hb below 7 g/dL at 34 weeks is a time-critical situation requiring parenteral iron or transfusion, not simply a dose escalation of oral tablets. Reflect on the key thresholds you have encountered in this module, and use the micro-quiz questions to confirm that you can apply them to clinical vignettes accurately and without hesitation.
Key thresholds to remember:
• WHO definition: Hb <11 g/dL (all trimesters)
• Severe anaemia: Hb <7 g/dL
• Very severe (emergency): Hb <4 g/dL
• Oral iron indicated: Hb 7–10.9 g/dL
• Parenteral iron indicated: Hb <7 g/dL or oral failure at term
• Blood transfusion: Hb <7 g/dL in third trimester or symptomatic
• NHM prophylaxis: 60 mg elemental iron + 500 mcg folic acid daily