Page 28 of 38
OG12.10 | Gynaecological and Surgical Disorders in Pregnancy — SDL Guide
Learning Objectives
- Recognise the altered clinical presentation of common surgical emergencies (appendicitis, cholecystitis, intestinal obstruction, ovarian torsion) in the pregnant patient
- Explain the pathophysiological mechanisms by which pregnancy predisposes to, or modifies, gynaecological and surgical complications
- Select appropriate investigations, including imaging modalities safe for use in pregnancy, to reach a timely diagnosis
- Outline the management principles for each condition, including timing of surgery, surgical approach, anaesthetic considerations, tocolysis, and fetal surveillance
- Counsel patients and their families about the maternal and fetal risks of surgical intervention during pregnancy
INSTRUCTIONS
Non-obstetric surgical emergencies complicate approximately 1 in 500–635 pregnancies and represent a challenging diagnostic and therapeutic problem. The anatomical displacement caused by the enlarging uterus, the physiological leukocytosis of pregnancy, and the masked peritoneal signs due to lax abdominal musculature all conspire to delay diagnosis. This module equips you to maintain a high index of suspicion, select radiation-safe investigations, and collaborate with the surgical team to deliver timely care without compromising fetal wellbeing.
References
- DC Dutta's Textbook of Obstetrics, 9th ed., Ch. 18 — Medical and Surgical Disorders in Pregnancy (textbook)
- Williams Obstetrics, 25th ed., Ch. 54 — General Considerations and Maternal Evaluation (textbook)
- ACOG Committee Opinion 775 — Non-Obstetric Surgery During Pregnancy, 2019 (guideline)
- Shaw's Textbook of Gynaecology, 16th ed. (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 26-year-old primigravida at 24 weeks of gestation presents to the emergency department at 2 a.m. with an 18-hour history of periumbilical pain that has migrated to the right side of her abdomen. She has vomited twice and has a low-grade fever of 37.8°C. On examination, there is guarding in the right lumbar region rather than the classic right iliac fossa. Her total leukocyte count is 18,000/µL. The on-call obstetric registrar considers the normal leukocytosis of pregnancy and wonders whether this is truly significant. As the diagnosis wavers, the question arises: if this is appendicitis and perforation occurs, what are the consequences for mother and fetus?
WHY THIS MATTERS
Surgical and gynaecological complications in pregnancy are a significant cause of maternal morbidity and indirect maternal mortality in India. Unlike purely obstetric emergencies, these conditions require joint obstetric–surgical decision-making, and delays in diagnosis — common because of atypical presentations — directly worsen outcomes for both the mother and the fetus. As a graduating doctor, you will be the first contact physician in any district hospital, expected to identify these conditions promptly and initiate appropriate referral or management. Understanding the altered anatomy, physiology, and diagnostic criteria in the pregnant patient is therefore not an academic exercise but a life-saving clinical skill.
RECALL
Before proceeding, recall from your basic science training:
• The anatomical changes of pregnancy: the uterus rises from a pelvic organ at 12 weeks to reaching the umbilicus at 20 weeks and the xiphisternum near term — displacing bowel loops upward and laterally.
• The physiological leukocytosis of pregnancy: white cell counts of 10,000–16,000/µL (and up to 20,000–30,000/µL in labour) are normal — so mild leukocytosis alone is not diagnostic of infection in pregnancy.
• The immunological changes of pregnancy: a shift towards Th2 immunity may alter inflammatory responses and mask typical peritoneal signs.
• Progesterone's smooth muscle relaxant effect: relaxes the biliary tract and delays intestinal transit, predisposing to gallstone formation and constipation.
• The anatomy of the right ovary and its relationship to the ovarian ligament: torsion occurs when the ovary, often bearing a cyst, rotates on its pedicle, compromising its blood supply.
Clinical Presentation of Surgical Emergencies in Pregnancy
Surgical emergencies in pregnancy are notoriously difficult to diagnose because the anatomical and physiological changes of the gravid uterus distort the classical clinical picture. Recognising these deviations is the first and most critical step — a missed or delayed diagnosis carries serious maternal and fetal consequences.
Appendicitis is the commonest non-obstetric surgical emergency in pregnancy, occurring in approximately 1 in 1,500 pregnancies. The classic presentation — pain at McBurney's point (one-third of the way from the anterior superior iliac spine to the umbilicus), nausea, vomiting, and fever — is progressively distorted as the uterus enlarges and displaces the appendix upward and to the right. By the third trimester, appendiceal tenderness may be found in the right flank or even the right hypochondrium, far above the iliac fossa. Rovsing's sign (pain in the right iliac fossa on palpation of the left side) becomes unreliable. Peritoneal guarding may be diminished because the stretched abdominal wall is separated from the underlying appendix by the uterus. Alder's sign is useful: if the point of maximum tenderness shifts to the left when the patient rolls to the left lateral decubitus position, the pain is from the uterus (not appendicitis); tenderness fixed in position points to an extra-uterine source. Fever, leukocytosis, and anorexia are present, but must be interpreted against the physiological baseline of pregnancy.
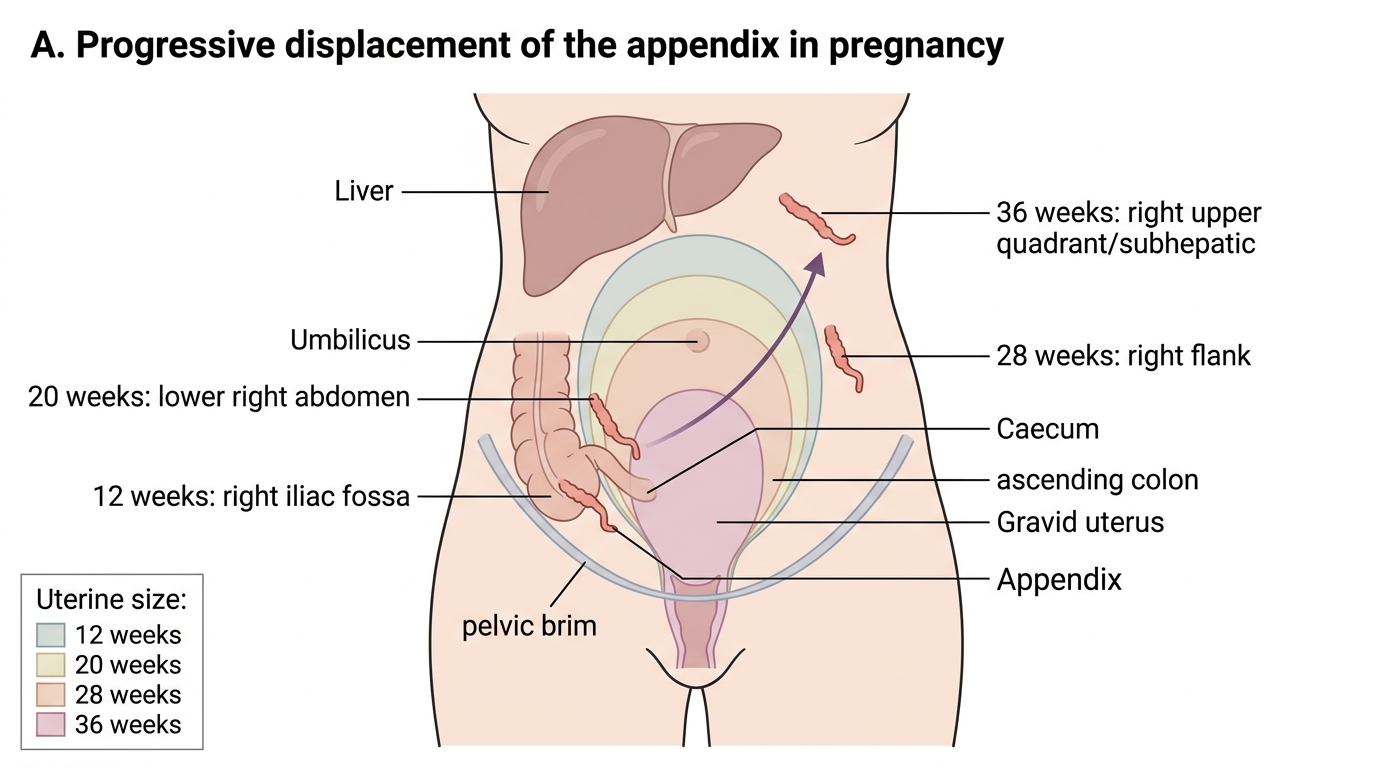
Appendix Displacement During Pregnancy
Ovarian torsion is the third commonest gynaecological emergency in pregnancy (after ectopic pregnancy and corpus luteum complications). Torsion occurs when an ovarian cyst (commonly a dermoid, corpus luteum cyst, or benign serous cystadenoma) rotates on its ligamentous pedicle, initially obstructing venous and lymphatic drainage and eventually arterial inflow. The presentation is acute onset of unilateral lower abdominal or pelvic pain — often crampy and colicky, sometimes with a positional component. Nausea, vomiting, and low-grade fever follow as the ovary becomes oedematous and ischaemic. In pregnancy, however, the enlarged uterus may displace the adnexa upward, shifting the point of maximal tenderness and making the clinical picture ambiguous.
Fibroid red (carneous) degeneration presents as acute localised pain directly over a fibroid, typically between 14 and 22 weeks when the rapidly growing fibroid outstrips its vascular supply. The patient is systemically unwell (low-grade fever, uterine tenderness), but without signs of peritonism or adnexal pathology. The uterus is often palpably enlarged for dates, and the fibroid may be tender to direct palpation.
Acute cholecystitis in pregnancy presents similarly to the non-pregnant state: right upper quadrant (RUQ) colicky pain — particularly postprandial after fatty meals — radiating to the right shoulder tip (Boas' sign), nausea, vomiting, and fever. Murphy's sign (arrest of inspiration on deep palpation of the right hypochondrium) remains useful, though it may be less reproducible in advanced pregnancy when the liver and gallbladder are pushed upward.
Intestinal obstruction in pregnancy presents with central colicky abdominal pain, absolute constipation, bilious vomiting, abdominal distension, and high-pitched ('tinkling') bowel sounds. Most cases are due to adhesions from prior pelvic surgery; in late pregnancy the enlarging uterus may cause volvulus of the sigmoid colon or right iliac fossa tethering at old adhesion sites.
SELF-CHECK
A primigravida at 30 weeks presents with right-sided abdominal pain and low-grade fever. Tenderness is elicited in the right lumbar region, not the right iliac fossa. Which feature is most specific for this gestational shift in the clinical presentation?
A. Positive Rovsing's sign
B. Leukocytosis of 14,000/µL
C. Tenderness in the right flank rather than McBurney's point
D. Nausea and anorexia
Reveal Answer
Answer: C. Tenderness in the right flank rather than McBurney's point
By 30 weeks, the appendix is displaced upward and to the right by the gravid uterus, reaching the right lumbar (flank) or even subhepatic region. Tenderness that is higher and more lateral than McBurney's point is the specific discriminator in the third trimester. Rovsing's sign is unreliable in pregnancy; leukocytosis is physiological; nausea and anorexia are non-specific.
Pathophysiology and Mechanisms of Complications
Understanding why pregnancy increases the risk and alters the course of surgical complications requires appreciation of the anatomical, hormonal, immunological, and vascular changes that occur across the three trimesters.
Appendicitis in pregnancy shares the same basic mechanism as in the non-pregnant patient — luminal obstruction (by a faecolith, mucosal lymphoid hyperplasia, or fibrosis) leads to bacterial overgrowth within the distended appendix, followed by ischaemia and, if untreated, gangrenous perforation with localised abscess or diffuse peritonitis. In pregnancy, two additional factors worsen outcomes. First, the displaced appendix is farther from the anterior abdominal wall, so the greater omentum — which normally walls off appendiceal perforation — cannot reach the appendix efficiently in the third trimester, predisposing to generalised peritonitis rather than localised abscess. Second, the immunological shift of pregnancy (Th2 predominance, elevated plasma proteins) blunts the peritoneal inflammatory response, masking guarding and rigidity until the condition is advanced. Fetal mortality rates rise from approximately 1.5% with simple appendicitis to 20–35% with perforation, primarily due to preterm labour triggered by intraperitoneal sepsis.
Ovarian torsion is precipitated by the presence of a cyst that enlarges the ovary beyond its normal ligamentous constraints. Corpus luteum cysts (common in the first trimester), dermoid cysts, and benign serous cystadenomas are the commonest culprits. When the ovary rotates on its pedicle, venous and lymphatic drainage is obstructed first (producing marked oedema and enlargement of the ovary), followed by arterial occlusion — leading to haemorrhagic infarction and, ultimately, necrosis. In pregnancy, the risk of torsion is heightened because ovarian hyperstimulation (particularly with ART pregnancies) and the rising uterus repositioning the ovaries make them more susceptible to mechanical twisting.
Fibroid red (carneous) degeneration occurs when the rapidly enlarging fibroid outstrips its vascular supply, leading to venous infarction and haemorrhagic necrosis of the fibroid centre. Progesterone and human chorionic gonadotrophin (hCG) stimulate fibroid growth in early pregnancy, predisposing to degeneration between 14 and 22 weeks. The process is self-limited but acutely painful. True uterine perforation, torsion, or preterm labour from fibroid degeneration is uncommon unless the fibroid is submucosal or adjacent to the placental bed.
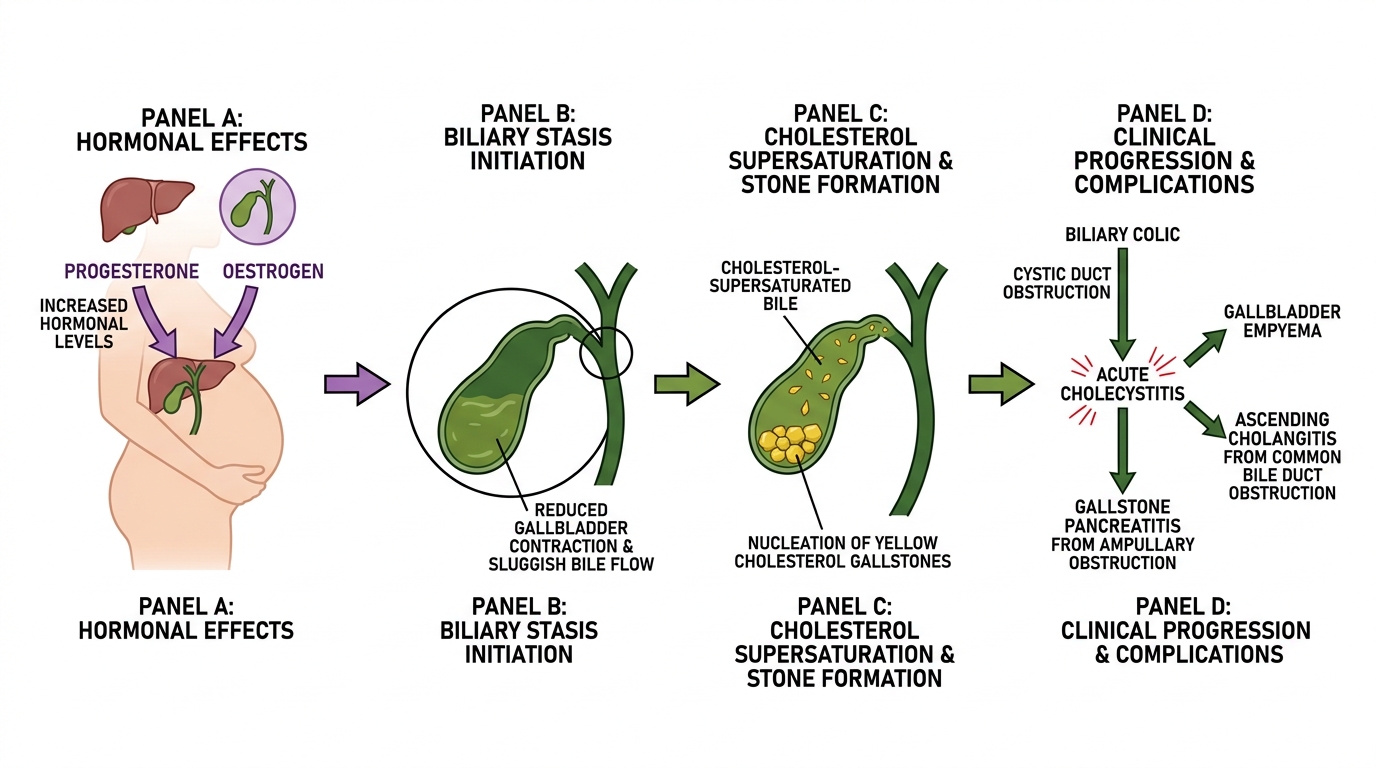
Pregnancy-Related Biliary Stasis and Gallstone Complications
Cholecystitis and cholelithiasis are directly facilitated by the hormonal milieu of pregnancy. Progesterone reduces gallbladder contractility and prolongs bile stasis, while oestrogen increases biliary cholesterol secretion and reduces the cholesterol-solubilising bile acid pool. These two changes together supersaturate bile with cholesterol, promoting nucleation and gallstone formation — particularly cholesterol stones. Gallstones are twice as common in parous versus nulliparous women, and symptomatic cholelithiasis complicates 0.1–0.3% of pregnancies. Progression from biliary colic → acute cholecystitis → empyema or cholangitis → gallstone pancreatitis follows the same cascade as in the non-pregnant patient, but treatment decisions are complicated by the fetal safety concerns around surgery and endoscopic intervention.
| Condition | Core mechanism in pregnancy | Key complication risk |
|---|---|---|
| Appendicitis | Luminal obstruction → bacterial overgrowth; displaced appendix → generalised peritonitis | Fetal mortality 20–35% with perforation |
| Ovarian torsion | Cyst enlarges ovary → mechanical rotation → venous obstruction → haemorrhagic infarction | Ovarian necrosis; preterm labour |
| Fibroid degeneration | hCG/progesterone → rapid fibroid growth → venous infarction of fibroid core | Acute pain; rarely preterm labour |
| Cholecystitis | Progesterone-induced biliary stasis + oestrogen-driven cholesterol supersaturation | Ascending cholangitis; gallstone pancreatitis |
| Intestinal obstruction | Adhesion tethering + uterine displacement → bowel trapping / sigmoid volvulus | Strangulation; maternal mortality 3–4% |
Intestinal obstruction in pregnancy is most commonly caused by adhesions from prior abdominal or pelvic surgery (caesarean section, myomectomy, appendicectomy) that tether loops of bowel, which are then distorted or compressed by the rapidly growing uterus. Sigmoid volvulus and caecal volvulus are rare but specific to pregnancy in later trimesters when the enlarged uterus acts as an axle around which the sigmoid rotates.
SELF-CHECK
Which combination of hormonal changes specifically promotes cholelithiasis in pregnancy?
A. Progesterone reduces gallbladder contractility; oestrogen increases biliary cholesterol secretion
B. hCG stimulates gallbladder emptying; oestrogen reduces bile salt pool
C. Progesterone increases bile salt synthesis; oestrogen promotes cholesterol absorption
D. Cortisol reduces gallbladder motility; oestrogen inhibits cholesterol secretion
Reveal Answer
Answer: A. Progesterone reduces gallbladder contractility; oestrogen increases biliary cholesterol secretion
In pregnancy, progesterone impairs gallbladder smooth muscle contractility, prolonging bile stasis. Oestrogen simultaneously increases biliary cholesterol secretion and reduces bile acid synthesis, supersaturating bile with cholesterol. Together, these two hormonal effects promote nucleation and growth of cholesterol gallstones, explaining the increased prevalence of gallstones in parous women.
Diagnosis and Investigations in Pregnant Patients
Diagnosis of surgical emergencies in pregnancy demands a structured, stepwise approach. It must respect the altered clinical picture — McBurney's point is unreliable after the first trimester, the normal leukocyte count of pregnancy is 10,000–16,000/µL (up to 20,000 in labour), and peritoneal guarding may be absent in advanced pregnancy because the stretched anterior abdominal wall separates the examiner's hand from the inflamed viscus. Serial clinical reassessment is indispensable: a rising total leukocyte count, increasing pain, and systemic deterioration collectively indicate surgical disease even when individual findings are equivocal. The investigative strategy must also accommodate fetal safety — the guiding principle is to use the lowest-radiation or no-radiation option that provides diagnostic certainty within the time available. Imaging should never be withheld when the clinical decision hinges on its result.
Clinical assessment begins with a careful history — character, onset, and migration of pain; associated symptoms (nausea, vomiting, fever, change in bowel habit, urinary symptoms); and obstetric history including gestation, prior surgeries, and antenatal findings. Examination findings should be interpreted with an understanding of the gestational age: McBurney's point is unreliable after 20 weeks, and peritoneal guarding may be absent even with perforation in late pregnancy.
Laboratory investigations:
• Full blood count (FBC): Total leukocyte count (TLC) is normally 10,000–16,000/µL in pregnancy; values >16,000–18,000/µL, or the presence of a marked left shift (band forms, toxic granulation), are clinically significant. A rising serial TLC is more informative than a single value.
• C-reactive protein (CRP): CRP is NOT elevated in physiological pregnancy and its elevation (>8–10 mg/L) is a useful marker of significant inflammation or infection, especially when combined with leukocytosis.
• Liver function tests (LFTs) and amylase/lipase for suspected cholecystitis or pancreatitis; urine microscopy and culture to exclude urinary tract infection (which mimics appendicitis).
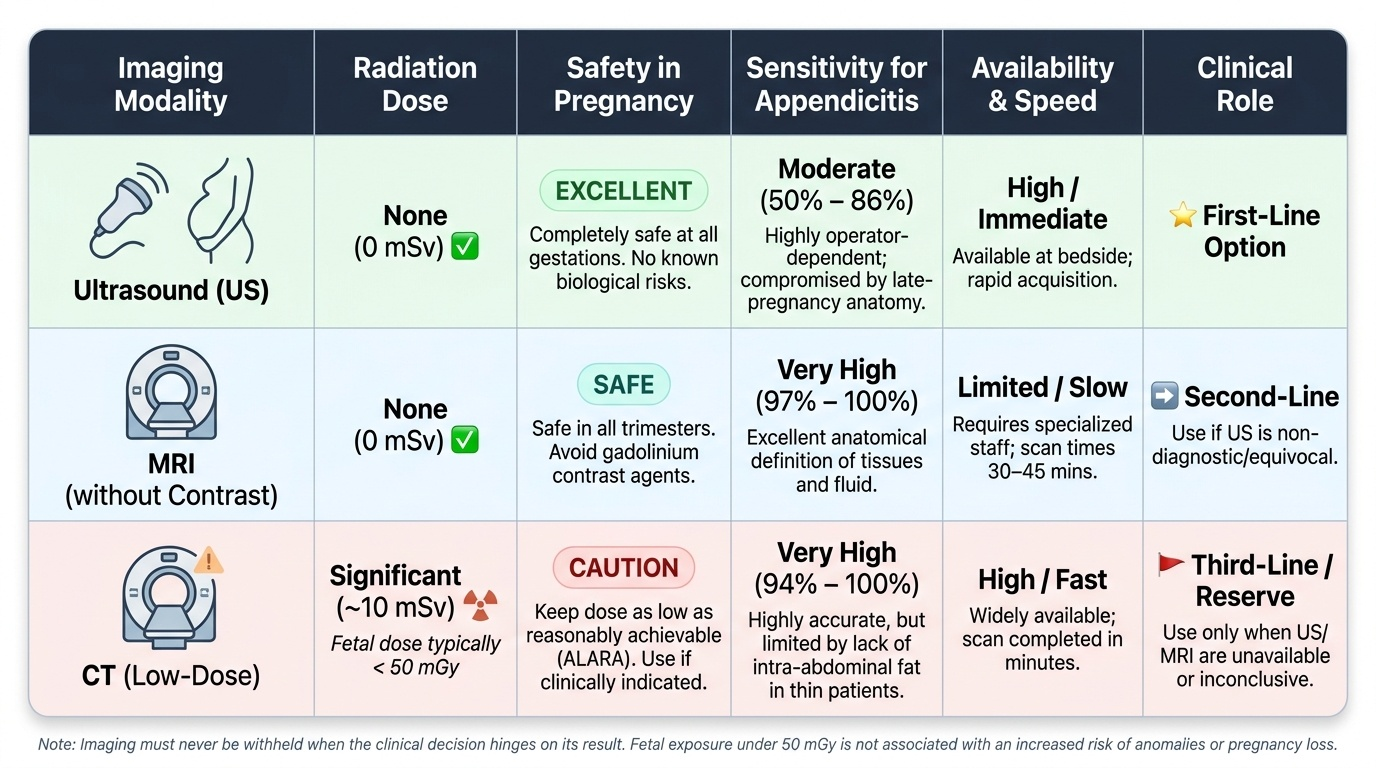
• Ultrasound abdomen and pelvis remains the first-line imaging in pregnancy: no ionising radiation, widely available, and diagnostic for ovarian torsion (Doppler flow absent or reduced in torsion), gallstones/cholecystitis, and adnexal masses. However, its sensitivity for appendicitis is limited in pregnancy (45–75%) due to appendiceal displacement and gas shadowing.
Provided image
MRI without gadolinium contrast is the preferred second-line modality for inconclusive ultrasound, especially after 20 weeks. It has no ionising radiation, visualises the displaced appendix in 97% of cases with high sensitivity (~94%) and specificity (~97%) for appendicitis, and evaluates the entire abdomen and pelvis. Gadolinium-based contrast agents cross the placenta and are avoided unless absolutely essential (WHO category B/C; ACOG recommends withholding in all trimesters unless the benefit clearly outweighs the theoretical teratogenic risk).
Computed tomography (CT abdomen and pelvis) is reserved for clinical situations where MRI is unavailable and the diagnosis remains uncertain, particularly when the risk of delayed diagnosis (perforation, sepsis) outweighs the radiation risk. The total fetal radiation dose from a CT abdomen-pelvis is approximately 25–30 mGy — below the threshold for direct teratogenic effect (>100 mGy), though theoretically increasing lifetime childhood cancer risk by a small margin. CT should not be reflexively withheld in a genuine emergency.
Diagnostic laparoscopy has evolved from a last resort to an acceptable primary surgical approach in the second trimester for equivocal cases where clinical deterioration is occurring. It confirms the diagnosis, allows direct treatment (appendicectomy, salpingo-oophorectomy in torsion), and avoids the prolonged radiation exposure of multiple CT scans. However, laparoscopic entry in the third trimester carries increased risk of uterine injury, and open Hasson technique (rather than Veress needle) is preferred.
Key diagnostic points by condition:
• Appendicitis: USS first; if inconclusive → MRI. Alvarado/MANTRELS score has limited validity in pregnancy — clinical gestalt and imaging predominate.
• Ovarian torsion: USS with colour Doppler is the primary test. Absence of Doppler flow strongly suggests torsion, but its presence does NOT exclude torsion (partial torsion may have preserved flow).
• Cholecystitis/cholelithiasis: USS is highly sensitive (>95%) for gallstones; thickened gallbladder wall (>4 mm), pericholecystic fluid, and a sonographic Murphy's sign support cholecystitis. MRCP replaces ERCP as the investigation for choledocholithiasis or biliary obstruction.
• Intestinal obstruction: Plain X-ray (erect abdomen, limited exposure) shows air-fluid levels and dilated loops; followed by CT if needed for severity/aetiology assessment.
SELF-CHECK
A 32-week primigravida with suspected appendicitis has had an inconclusive ultrasound. The surgical team requests imaging. Which is the most appropriate next step?
A. CT abdomen and pelvis with contrast
B. MRI abdomen and pelvis without gadolinium
C. Immediate exploratory laparotomy without further imaging
D. Repeat ultrasound in 6 hours
Reveal Answer
Answer: B. MRI abdomen and pelvis without gadolinium
MRI without gadolinium is the preferred second-line imaging in pregnancy when ultrasound is inconclusive. It carries no ionising radiation, provides high sensitivity (~94%) and specificity (~97%) for appendicitis, and can visualise the displaced appendix in the third trimester. CT should be reserved for situations where MRI is unavailable and clinical deterioration is imminent. Gadolinium-based contrast agents are avoided as they cross the placenta.