Page 29 of 38
OG12.10 | Gynaecological and Surgical Disorders in Pregnancy — SDL Guide (Part 2)
Management Principles: Conservative, Surgical, and Obstetric Considerations
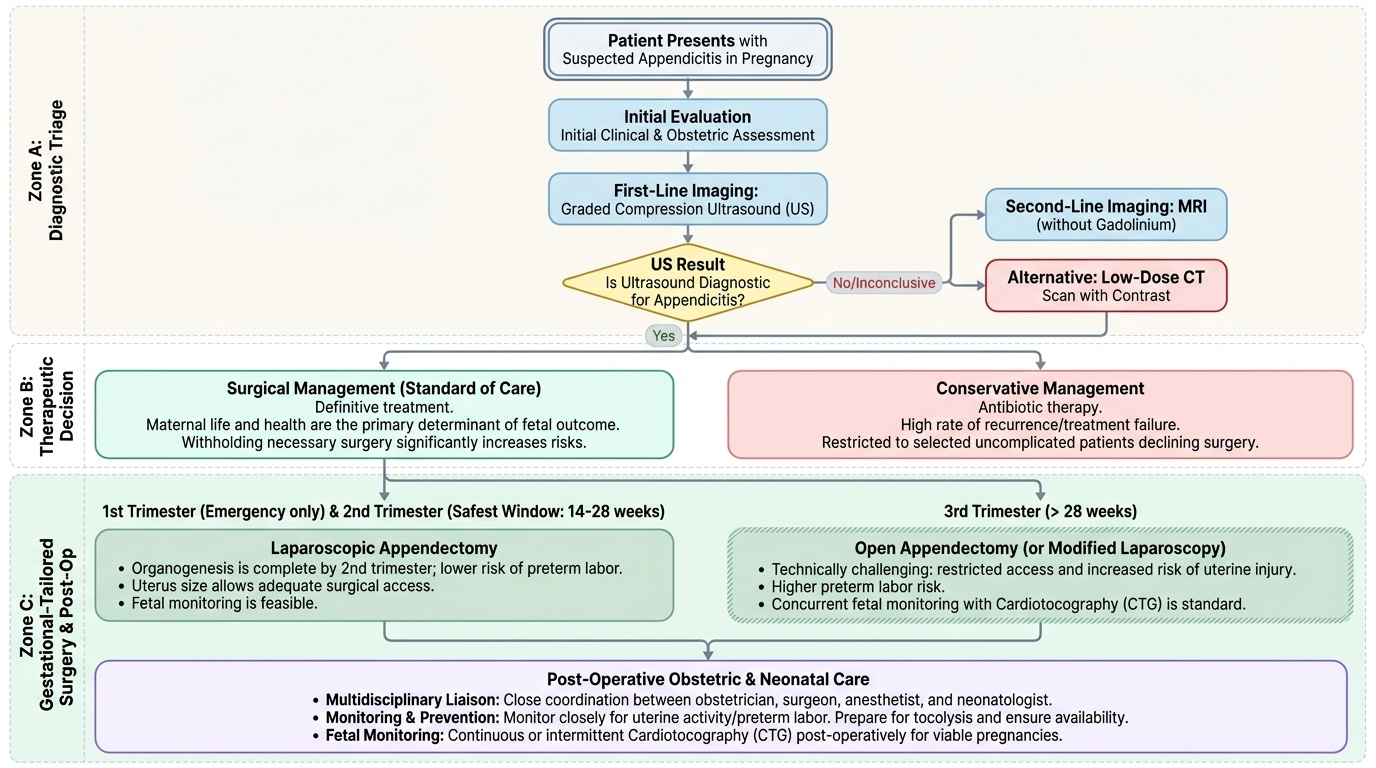
Management of surgical and gynaecological disorders in pregnancy demands careful coordination between the obstetrician, the general or gynaecological surgeon, the anaesthetist, and — in viable pregnancies — the neonatologist. The guiding philosophy is simple but non-negotiable: the mother's life and health are the primary determinant of fetal outcome, and withholding necessary surgical treatment to 'protect' the fetus is not only misguided but actively dangerous. Systemic sepsis, generalised peritonitis, haemodynamic shock, and untreated bowel strangulation all impose far higher fetal mortality and morbidity than a well-conducted operative procedure. The ACOG and FOGSI guidelines therefore recommend: treat maternal emergencies immediately regardless of gestational age; schedule semi-elective procedures in the second trimester (the safest window); and defer truly elective interventions until after delivery. The clinical team must also prepare for the possibility that surgery will precipitate preterm labour and plan accordingly — tocolysis monitoring, neonatal intensive care availability, and informed consent must all be addressed preoperatively.
Timing of surgery:
- First trimester: Surgery carries risks of spontaneous miscarriage, drug-induced teratogenicity, and anaesthetic exposure during organogenesis. Emergency surgery is performed as needed; elective and semi-elective surgery is deferred to the second trimester.
- Second trimester (14–28 weeks): the safest window for non-emergency surgery. The uterus is large enough that fetal monitoring is feasible, yet small enough to allow adequate surgical access. Organogenesis is complete, and the risk of preterm labour is lower than in the third trimester.
- Third trimester: Surgery is more technically challenging (restricted access, increased risk of uterine injury, higher preterm labour risk). However, it is not withheld when necessary; concurrent fetal monitoring with cardiotocography (CTG) is standard.
Provided image
Appendicitis: Surgical management is the standard of care — conservative antibiotics-only management carries a high perforation risk and is not recommended outside of trials. Laparoscopic appendicectomy is preferred in the first and second trimesters; it has equivalent outcomes to open surgery and carries no excess fetal loss. In the third trimester, a right-lateral (or right paramedian) open approach is often preferred because of restricted laparoscopic access and increased risk of uterine injury. The incision is placed at the point of maximum tenderness (which may be considerably higher than McBurney's). Post-operatively: IV antibiotics (ampicillin + gentamicin + metronidazole for 3–5 days for perforated cases), fetal surveillance with CTG, and tocolysis if uterine contractions are monitored.
Ovarian torsion: Prompt surgical detorsion preserves ovarian function — the ovary should be untwisted and assessed for viability before any decision to remove it, as the colour and appearance can recover dramatically after detorsion. Laparoscopic detorsion is the preferred approach; cystectomy or oophorectomy is performed only for necrotic ovary or specific histological risk (e.g., malignancy suspected). The operated ovary should be assessed at the next follow-up ultrasound for return of flow and follicular activity.
Fibroid red degeneration: Conservative management with analgesics (paracetamol; NSAIDs cautiously in mid-trimester, avoided after 32 weeks due to ductus arteriosus closure risk), hydration, bed rest, and reassurance is the mainstay. The acute episode typically resolves over 7–14 days. Rarely, refractory pain or threatened preterm labour warrants hospitalisation and tocolysis. Surgery is avoided unless there is torsion of a pedunculated fibroid, intestinal obstruction, or other rare complication.
Acute cholecystitis: In the first instance, conservative management with IV fluids, nil by mouth, IV antibiotics (cephalosporins + metronidazole for cholecystitis; add ciprofloxacin for cholangitis), and analgesia (opioids as needed — morphine or pethidine). Laparoscopic cholecystectomy during pregnancy is safe and should be performed for recurrent symptoms, failure of conservative management, or empyema — preferably in the second trimester. ERCP with sphincterotomy and stone extraction for choledocholithiasis is safe in pregnancy with appropriate radiation shielding; MRCP is preferred for diagnosis to avoid radiation.
Intestinal obstruction: Nasogastric decompression, IV fluids, correction of electrolytes, and serial abdominal assessment. Failure to improve within 24–48 hours (or immediate surgery for signs of strangulation: fever, raised white cells, peritonism) — perform exploratory laparotomy. Lysis of adhesions, volvulus reduction, and bowel resection if indicated. Concurrent fetal viability assessment and availability of neonatal intensive care for viable gestations.
Anaesthetic considerations: Regional anaesthesia (spinal/epidural) is preferred where feasible to minimise fetal drug exposure. When general anaesthesia is required, rapid sequence induction with cricoid pressure is standard (due to increased aspiration risk in pregnancy). Positioning: left lateral tilt of the operating table to displace the uterus from the inferior vena cava and prevent aortocaval compression. Neuromuscular agents, volatile anaesthetics, and opioids are used at lowest effective doses.
Tocolysis: Perioperative uterine contractions are monitored from approximately 20 weeks onward. Betamimetics (salbutamol IV) or indomethacin (NSAIDs, safe before 32 weeks) are used for tocolysis when contractions are detected. The decision to tocolyse is balanced against the underlying surgical condition.
Fetal surveillance: Doppler and CTG monitoring before and after surgery; biophysical profile in cases of prolonged surgery or intraoperative haemodynamic instability. The neonatal team should be present for all surgeries after 28 weeks in case emergency delivery is required.
CLINICAL PEARL
The single most important principle in managing surgical emergencies in pregnancy is this: do not delay surgery out of fear of harming the fetus. The greatest risk to the fetus comes not from a well-performed surgical procedure but from the systemic sepsis, peritonitis, and haemodynamic compromise that result from delayed intervention. A perforated appendix in a third-trimester patient carries a fetal mortality of 20–35%; prompt appendicectomy reduces this to under 2%. When in doubt, operate. Use the safest surgical approach available for the gestational age, protect the uterus at every step, and provide meticulous post-operative fetal surveillance — but never substitute watchful waiting for a surgical emergency.
SELF-CHECK
A 22-year-old woman at 19 weeks of gestation is diagnosed with acute appendicitis. Her vitals are stable and there is no evidence of perforation on MRI. What is the preferred surgical approach?
A. Open appendicectomy through a midline incision
B. Laparoscopic appendicectomy
C. Conservative management with IV antibiotics and hospital observation
D. Delay surgery until 28 weeks when the risk of preterm labour is lower
Reveal Answer
Answer: B. Laparoscopic appendicectomy
Laparoscopic appendicectomy is the preferred approach in the first and second trimesters for non-perforated appendicitis in a stable patient. It offers equivalent outcomes to open surgery with less post-operative pain, shorter hospital stay, and no excess fetal loss risk. The second trimester (14–28 weeks) is the safest operative window. Conservative antibiotics-only management has a high failure and perforation rate in pregnancy and is not standard of care. Surgery should not be delayed — perforation risk increases significantly with time.
Prevention, Counselling, and Fetal Prophylaxis
Prevention and counselling are integral to the management of surgical disorders in pregnancy, both before and after an acute event. From a preventive standpoint, most surgical emergencies such as appendicitis and ovarian torsion are not predictable or avoidable, but some conditions — particularly cholecystitis and intestinal obstruction from adhesions — have identifiable risk factors that merit counselling. Women with known cholelithiasis who are planning pregnancy should be counselled about the increased risk of symptomatic gallstone disease during pregnancy and the preference for elective laparoscopic cholecystectomy prior to conception if the stones are symptomatic. Women who have undergone prior abdominal or pelvic surgery should be advised of their elevated risk of intestinal obstruction from adhesions and counselled to seek early evaluation for any abdominal pain during pregnancy.
When a surgical emergency occurs during pregnancy, the counselling priorities are threefold. First, the patient and her family must understand that prompt surgical intervention — not delay — is the safest course for both mother and baby. Second, they must be informed about the specific maternal and fetal risks of the procedure, including the possibility of preterm labour (risk increases in the third trimester and with peritonitis), and the monitoring plan that will be in place postoperatively. Third, the patient should be informed about the expected recovery timeline, activity restrictions, and signs of postoperative complications (wound infection, preterm contractions, reduced fetal movements) that should prompt re-presentation.
For ovarian cysts detected incidentally during antenatal care, the counselling message is nuanced: most simple cysts <5 cm — particularly corpus luteum cysts in the first trimester — resolve spontaneously by 16–18 weeks and require surveillance only. Complex cysts or those persisting beyond 16 weeks merit closer monitoring and surgical planning, ideally in the second trimester. The patient should be advised to seek urgent review if she develops sudden-onset severe pelvic pain, which may herald torsion. For women with known uterine fibroids, red degeneration should be discussed as a possible event, with reassurance that it is almost always managed conservatively and does not threaten the pregnancy in the vast majority of cases. The baby's fetal wellbeing is monitored throughout the acute phase and, if the pregnancy is stable and fetal movements are normal, preterm delivery is not indicated.
Fetal surveillance after any abdominal surgery in pregnancy includes daily CTG from 28 weeks, and ultrasound fetal biometry and Doppler assessment at 2–4 weeks post-operatively to ensure there has been no growth restriction from perioperative haemodynamic compromise. Women should be counselled about the signs of preterm labour and given written information on when to attend the labour ward directly.