Page 19 of 38
OG12.7 | HIV in Pregnancy — SDL Guide
Learning Objectives
- Describe the universal opt-out HIV screening protocol in antenatal care under the NACO PPTCT programme
- Explain the three routes of mother-to-child transmission (MTCT) of HIV and their relative contributions
- Outline the Option B+ lifelong ART regimen (TDF+3TC+EFV) and when to initiate it in pregnancy
- Determine mode of delivery based on viral load at 36 weeks
- Describe infant prophylaxis protocols (NVP 6 weeks vs NVP+AZT 12 weeks) and explain the AFASS-based infant feeding recommendation
INSTRUCTIONS
HIV infection in pregnancy poses one of the most preventable tragedies in modern medicine: an infant acquiring a lifelong chronic infection from its mother during a period when the transmission is almost entirely preventable with the right intervention at the right time. India's national PPTCT programme has dramatically reduced transmission rates, but the programme depends on every healthcare provider — doctor, nurse, and midwife — understanding the testing protocol, the treatment regimen, the delivery decision, and the nuanced feeding guidance. This module takes you through each of these components step-by-step, with a focus on the NACO 2021 guidelines that govern practice in India.
References
- NACO — Prevention of Parent-to-Child Transmission of HIV Guidelines, India 2021 (guideline)
- DC Dutta's Textbook of Obstetrics, 9th ed., Ch 18 — Medical Disorders in Pregnancy (textbook)
- WHO — Consolidated Guidelines on HIV Prevention, Testing, Treatment and Care, 2021 (guideline)
- Williams Obstetrics, 26th ed., Ch 65 — HIV Infection (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Priya is a 24-year-old primigravida attending her first antenatal visit at 12 weeks gestation. The ANM at the sub-centre offers her the routine opt-out HIV test as part of the ANC package. Priya is surprised — she has been in a monogamous relationship for 3 years and feels well. The rapid test returns reactive. On confirmatory testing at the ICTC, she is confirmed HIV-positive with a CD4 count of 480 cells/µL and a viral load of 12,000 copies/mL. Her husband tests negative. She has no symptoms and no opportunistic infections. She is frightened and asks: 'Will my baby get this? Can I breastfeed? Do I need tablets forever?' Every answer you give her in the next thirty minutes will either protect her baby's life or leave it at risk. What do you tell her?
WHY THIS MATTERS
HIV complicates approximately 0.3% of pregnancies in India, though prevalence varies substantially by state (higher in southern India and Maharashtra). Without any intervention, mother-to-child transmission (MTCT) of HIV occurs in 25–45% of pregnancies — around 15,000–20,000 infants in India could acquire HIV annually. With a fully implemented PPTCT programme (ART + optimal delivery + safe feeding), MTCT rates can be reduced to below 2%. The NACO PPTCT programme is therefore a genuine life-saving public health intervention, and its success depends on healthcare providers who can accurately counsel, prescribe, and follow up HIV-positive pregnant women. As a final-year student, you will participate in antenatal care and deliveries — understanding this protocol is not optional.
RECALL
Recall from your Microbiology studies that HIV is an RNA retrovirus of the Lentivirus genus. It infects CD4+ T-lymphocytes, macrophages, and dendritic cells by binding its envelope glycoprotein gp120 to the CD4 receptor and a co-receptor (CCR5 or CXCR4). After entry, reverse transcriptase converts viral RNA to proviral DNA, which integrates into the host genome. The virus then undergoes replication, assembly, and budding. Progressive CD4+ T-cell depletion leads to AIDS (CD4 <200 cells/µL). Recall from Pharmacology that antiretroviral classes include NRTIs (block reverse transcriptase as false substrates), NNRTIs (non-competitive reverse transcriptase inhibitors), protease inhibitors, and integrase inhibitors. This molecular basis explains why combination ART (targeting multiple steps) suppresses viral replication more effectively than monotherapy.
A Pregnant Woman Who Tests HIV-Positive — What Happens Next?
The typical presentation of HIV complicating pregnancy in India is a completely asymptomatic woman discovered at routine antenatal screening — she has no rash, no lymphadenopathy, no opportunistic infections, and may have been infected for years without knowing. This is the clinical reality of India's epidemic: the majority of HIV-positive pregnant women are in the chronic, clinically latent phase of infection, and would never seek HIV testing without the universal ANC screening programme.
A minority present with features that should raise suspicion even before formal testing: unexplained weight loss, persistent fever, oral candidiasis (white plaques that cannot be scraped off), generalised lymphadenopathy, or a history of recurrent herpes zoster in a young woman. In the obstetric context, recurrent pregnancy loss, severe anaemia unresponsive to haematinics, or an infant who has died in early infancy from an unidentified illness should prompt HIV testing.
Staging and immunological assessment at first presentation involves:
- CD4+ T-cell count: the key measure of immunological status. CD4 <200 cells/µL = AIDS-defining immunosuppression and mandates prophylaxis against opportunistic infections (OIs); CD4 200–350 = moderate immunosuppression; CD4 >500 = near-normal immunity. Under Option B+, ALL HIV-positive pregnant women are started on ART regardless of CD4 count — CD4 no longer determines when to start, but it guides OI prophylaxis and monitoring frequency.
- HIV viral load: the measure of active viral replication. A high viral load (>10,000 copies/mL) indicates active replication and higher transmission risk; the goal of ART is to achieve an undetectable viral load (<50 copies/mL) — at which point, MTCT risk is near-zero.
- WHO clinical staging (I–IV): Stage I = asymptomatic; Stage II = mild OIs/constitutional; Stage III = severe/advanced OIs (TB, severe bacterial infections); Stage IV = AIDS-defining illnesses (PCP, CMV retinitis, Cryptococcal meningitis, etc.).
The immediate priorities after a confirmed positive test are: (1) counselling the woman and her partner (discordant-couple counselling is mandatory), (2) notifying the ICTC for programme enrolment, (3) staging with CD4/VL/clinical assessment, (4) initiating ART under Option B+, and (5) planning mode of delivery and infant prophylaxis.
SELF-CHECK
Under NACO's Option B+ programme, at what CD4 count should a newly diagnosed HIV-positive pregnant woman at 16 weeks gestation start ART?
A. Only if CD4 <200 cells/µL
B. Only if CD4 <350 cells/µL
C. Only if CD4 <500 cells/µL
D. Regardless of CD4 count — all HIV-positive pregnant women start ART
Reveal Answer
Answer: D. Regardless of CD4 count — all HIV-positive pregnant women start ART
Option B+ (NACO India 2021, WHO 2015 guidelines) mandates lifelong ART for ALL HIV-positive pregnant and breastfeeding women, regardless of CD4 count or WHO clinical stage. This replaced earlier threshold-based approaches (Option A: prophylaxis only; Option B: ART during pregnancy+BF only) because lifelong treatment both prevents MTCT and benefits maternal health by maintaining viral suppression. There is no CD4 floor for starting ART in pregnancy.
How HIV Passes from Mother to Child — Pathophysiology of MTCT
Mother-to-child transmission (MTCT) of HIV occurs via three distinct biological routes, each with a different mechanism, timing, and preventive intervention. Without any prophylaxis, the overall MTCT rate is 25–45%; understanding each route is essential to understanding why each component of the PPTCT programme is necessary.
Route 1 — Antepartum (Transplacental) Transmission (30–40% of total MTCT):
The placenta is not an absolute barrier to HIV. During pregnancy, HIV-infected maternal CD4+ T-cells and free virions can cross the trophoblast layer, particularly when maternal viral load is high, the placenta is inflamed (chorioamnionitis), or there are placental disruptions (abruption, trauma). The risk is concentrated in the third trimester when placental permeability increases. Factors increasing antepartum transmission: high maternal viral load, low CD4 count, concurrent STIs causing placental inflammation, and first HIV infection during pregnancy (high viral replication, no antibody response yet — "acute HIV in pregnancy" carries the highest MTCT risk).
Route 2 — Intrapartum Transmission (50–65% of total MTCT):
This is the single largest route and the most preventable. During labour and delivery, the infant is exposed to HIV-infected maternal blood, cervicovaginal secretions, and amniotic fluid. Mechanisms include direct mucosal contact, microabrasions on the infant's skin or scalp, and ingestion of infected fluids. The duration of membrane rupture is an independent risk factor — prolonged rupture of membranes (>4 hours) significantly increases intrapartum exposure time. Invasive procedures (fetal scalp electrode, fetal blood sampling, forceps/ventouse with scalp trauma) further breach the infant's mucosal barrier. This is why mode of delivery — guided by the viral load at 36 weeks — is the most powerful single intrapartum intervention.
Route 3 — Postnatal (Breastfeeding) Transmission (10–20% of total MTCT):
HIV is present in breast milk — both free virions and cell-associated HIV in macrophages. Each breastfeeding exposure carries a small but cumulative risk of transmission: approximately 0.3% per month of exclusive breastfeeding in an untreated woman. Mixed feeding (combining breastfeeding with formula, water, or solids) dramatically increases transmission risk because solids and formula damage the infant gut mucosa, increasing viral entry. Prolonged breastfeeding beyond 12 months in the absence of ART carries substantial cumulative risk.
Effect of HIV on pregnancy and of pregnancy on HIV: HIV-positive women have higher rates of preterm birth, low birth weight, fetal growth restriction, stillbirth, and maternal anaemia. Pregnancy does not substantially accelerate HIV progression when CD4 is >200, but acute HIV seroconversion in pregnancy (first trimester, peak viraemia phase) carries a very high MTCT risk. Antiretroviral drugs cross the placenta and can affect fetal growth (efavirenz data reassuring for neural tube defects at therapeutic doses; TDF can cause mild fetal renal effects in some studies — monitoring advised).
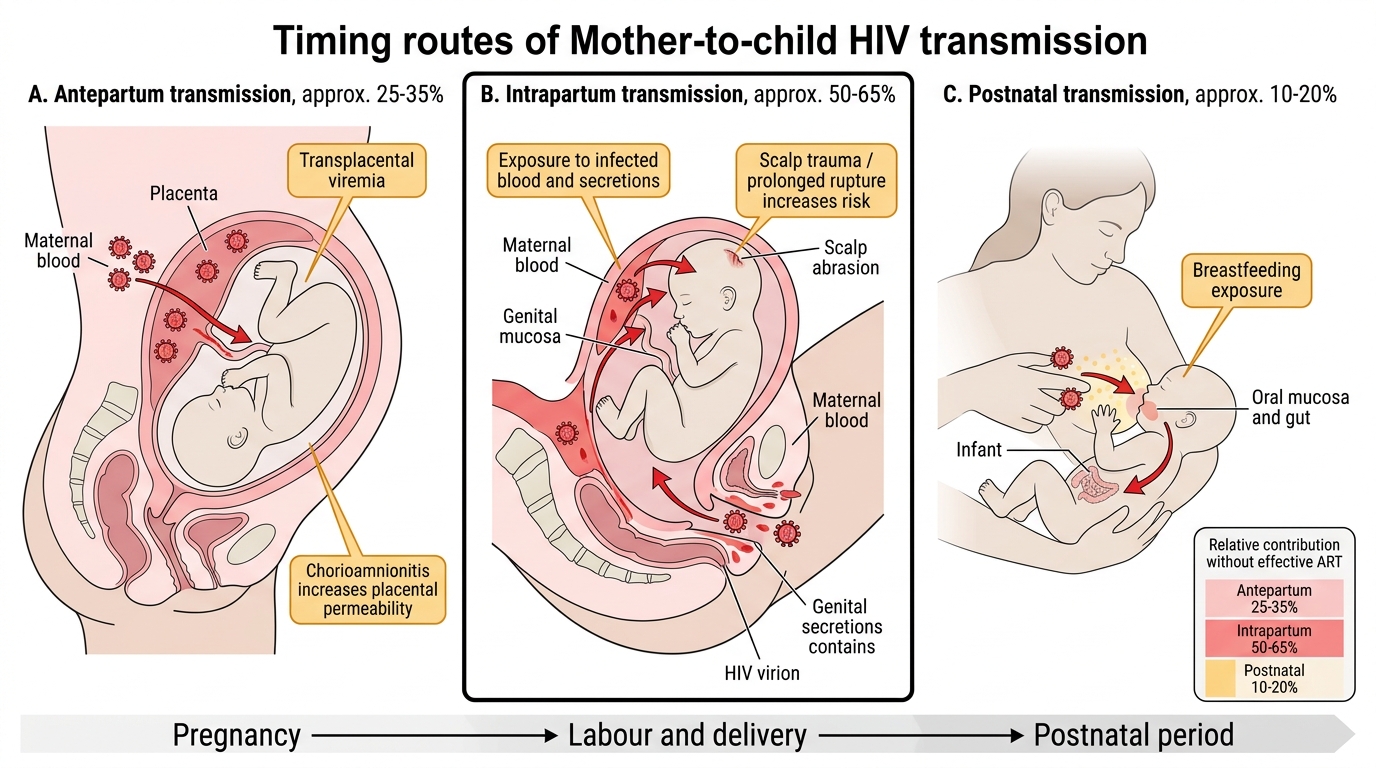
Routes of Mother-to-Child HIV Transmission
Screening, Diagnosis, and Baseline Assessment
India's NACO PPTCT programme mandates universal opt-out HIV testing at the first antenatal visit for all pregnant women. 'Opt-out' means the test is offered as a routine part of the ANC package, and the woman can decline — but refusal must be documented in the antenatal record. This approach removes the social stigma of a woman proactively requesting an HIV test, which in many communities is associated with perceived infidelity or high-risk behaviour, and has dramatically increased testing uptake compared to the earlier opt-in model. The test is performed alongside other routine first-trimester ANC investigations such as haemoglobin estimation, blood grouping and cross-matching, VDRL for syphilis, and HBsAg, making HIV screening a normalised part of the antenatal encounter rather than a singled-out procedure. Universal screening has been the single most powerful lever for increasing PPTCT programme coverage in India, particularly in high-prevalence states such as Maharashtra, Andhra Pradesh, Telangana, and Tamil Nadu.
The NACO HIV testing algorithm in pregnancy uses a sequential rapid diagnostic test (RDT) strategy that balances sensitivity with specificity:
- Test 1 (RDT-1): any ELISA or rapid test (high sensitivity); if NON-REACTIVE → negative, no further testing at this visit. If REACTIVE → proceed.
- Test 2 (RDT-2): a second assay with a different antigen preparation; if REACTIVE on both Test 1 and Test 2 → HIV POSITIVE, proceed to management.
- If Test 1 REACTIVE but Test 2 NON-REACTIVE → DISCORDANT → repeat testing after 2–4 weeks; meanwhile counsel and manage as possibly positive.
All reactive results require ICTC (Integrated Counselling and Testing Centre) confirmation and programme enrolment. In practice, two concordantly reactive rapid tests are operationally diagnostic; Western blot is used to resolve discordant results.
Baseline investigations at diagnosis:
- CD4+ T-cell count — for staging and OI prophylaxis decisions (co-trimoxazole prophylaxis if CD4 <200 or WHO stage III/IV)
- HIV viral load (plasma RNA copies/mL) — baseline and repeat at 36 weeks to guide delivery mode
- Complete blood count — anaemia (AZT myelosuppression if used), thrombocytopaenia (immune thrombocytopaenia in HIV)
- Liver function tests — hepatitis B/C co-infection screening; baseline before hepatotoxic ARVs
- Renal function and urinalysis — tenofovir (TDF) can cause tubulopathy; monitor creatinine
- HBsAg, anti-HCV, VDRL — co-infections that increase MTCT and complicate management
- TB screening — sputum AFB and chest X-ray (shielded); TB is the most common OI in HIV-positive Indians
- Glucose tolerance test — HIV and some ARVs increase diabetes risk
Partner testing and couple HIV counselling are mandatory under the NACO programme. For a discordant couple (one HIV-positive, one negative), the negative partner must be counselled on consistent condom use and offered Pre-Exposure Prophylaxis (PrEP).
SELF-CHECK
An HIV-positive pregnant woman at 36 weeks has a viral load of 650 copies/mL on ART started at 14 weeks. What mode of delivery would you recommend?
A. Elective caesarean section at 38 weeks — viral load is detectable
B. Vaginal delivery is acceptable — viral load <1,000 copies/mL
C. Emergency caesarean for any detectable viral load
D. Vaginal delivery is acceptable only if viral load is undetectable (<50 copies/mL)
Reveal Answer
Answer: B. Vaginal delivery is acceptable — viral load <1,000 copies/mL
The WHO/NACO threshold for recommending vaginal delivery is a viral load <1,000 copies/mL at 36 weeks — not necessarily undetectable. A VL of 650 copies/mL falls below the 1,000 threshold, so vaginal delivery is acceptable provided labour is managed carefully (avoid prolonged ROM >4 hours, avoid invasive fetal monitoring, minimise perineal trauma). Elective LSCS is recommended if VL ≥1,000 copies/mL or if VL status is unknown at term.