Page 20 of 38
OG12.7 | HIV in Pregnancy — SDL Guide (Part 2)
Management of HIV in Pregnancy — PPTCT/PMTCT
The NACO 2021 PPTCT programme integrates maternal treatment and infant prophylaxis into a seamless continuum of care. Its four components — ART, viral-load-guided delivery, infant prophylaxis, and infant feeding counselling — each address a distinct transmission window.
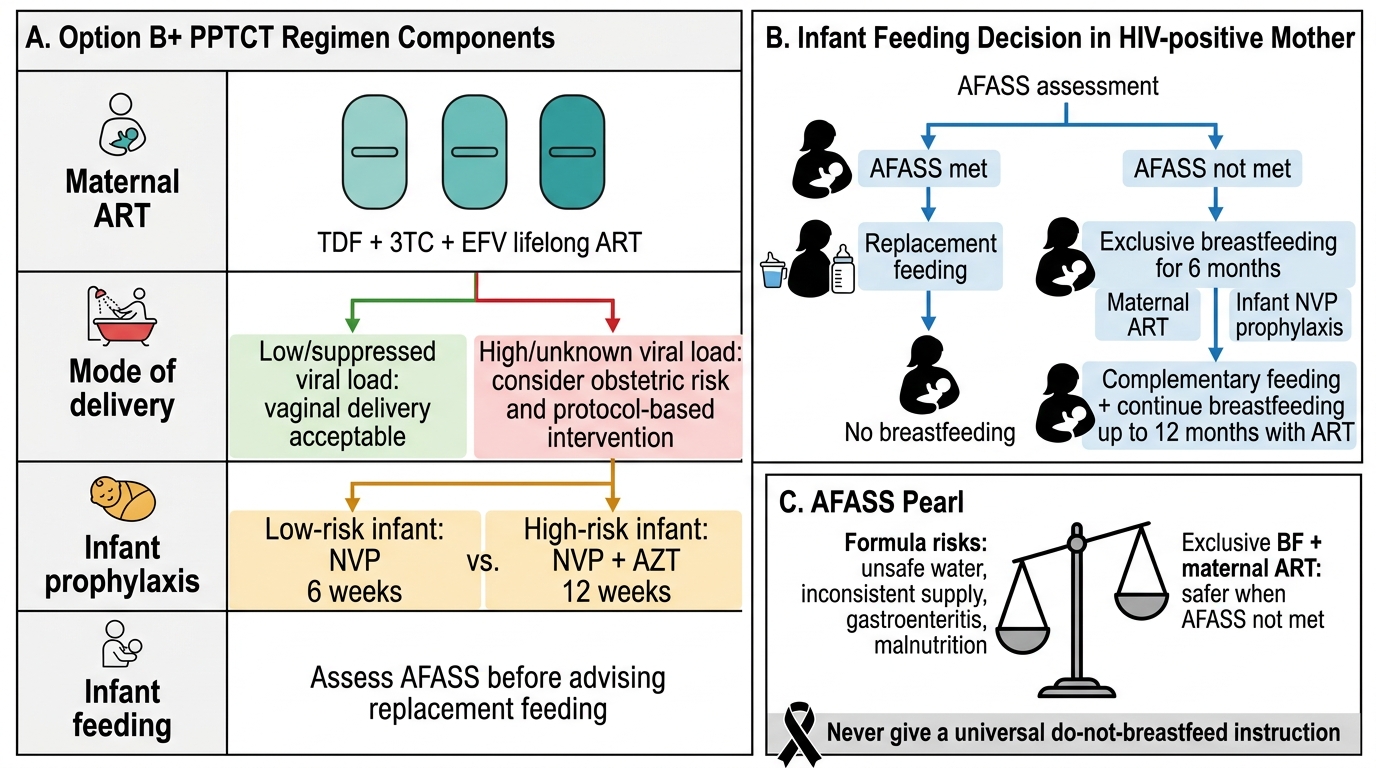
1. Maternal Antiretroviral Therapy — Option B+ (Lifelong ART):
The first-line regimen under NACO 2021 is TDF + 3TC + EFV (tenofovir disoproxil fumarate 300 mg + lamivudine 150 mg + efavirenz 600 mg) as a single fixed-dose combination (FDC) tablet once daily. This should be started as early as possible in pregnancy — ideally at the first ANC visit. Efavirenz was previously avoided in the first trimester due to concerns about neural tube defects, but the available evidence (largely from the Surveillance Monitoring for ART Toxicities study) suggests this risk is not significantly elevated at therapeutic doses; NACO and WHO recommend EFV throughout pregnancy including the first trimester. The goal of ART is to achieve an undetectable viral load (<50 copies/mL) — reducing MTCT risk to <1% with all other components in place. ART is continued lifelong after delivery regardless of breastfeeding status (Option B+ core principle).
Key drug side effects and monitoring during pregnancy:
- TDF: renal tubular toxicity (monitor creatinine and urine protein monthly); avoid in pre-existing renal impairment
- EFV: vivid dreams, dizziness (CNS effects), rash; monitor LFTs
- 3TC: generally well-tolerated; active against hepatitis B co-infection (important: do NOT stop 3TC in HBV co-infection — hepatic flare can occur)
- All ARVs: monitor for anaemia, hepatotoxicity, and drug interactions (particularly rifampicin for TB co-treatment → switch to dolutegravir-based regimen)
2. Viral-Load-Guided Mode of Delivery:
At 36 weeks, repeat viral load measurement is performed. The decision rule:
- VL <1,000 copies/mL: vaginal delivery is acceptable. In labour: avoid prolonged rupture of membranes (>4 hours), avoid amniotomy unless necessary, avoid fetal scalp electrode and invasive fetal blood sampling, perform episiotomy only when clinically indicated, and minimise perineal trauma.
- VL ≥1,000 copies/mL or unknown VL: elective lower segment caesarean section (LSCS) at 38 completed weeks is recommended. Emergency LSCS for obstetric indications when VL ≥1,000 does not negate the benefit but carry higher intrapartum exposure time.
- Intrapartum single-dose NVP (for the mother) is no longer routinely recommended when the mother is on optimally suppressive ART with VL <1,000 — it was used in the pre-Option B+ era for women not on ART.
3. Infant Prophylaxis:
All infants born to HIV-positive mothers receive antiretroviral prophylaxis from birth:
- Standard/low-risk: oral nevirapine (NVP) syrup for 6 weeks from birth, regardless of feeding method
- High-risk (mother not on ART at delivery, or maternal VL ≥1,000 copies/mL, or breastfeeding infant with unknown maternal VL): NVP + AZT (zidovudine) for 12 weeks
NVP syrup dose: 2 mg/kg/day for birth weight ≥2.5 kg; weight-adjusted for low birth weight. Daily NVP is given through the entire prophylaxis period.
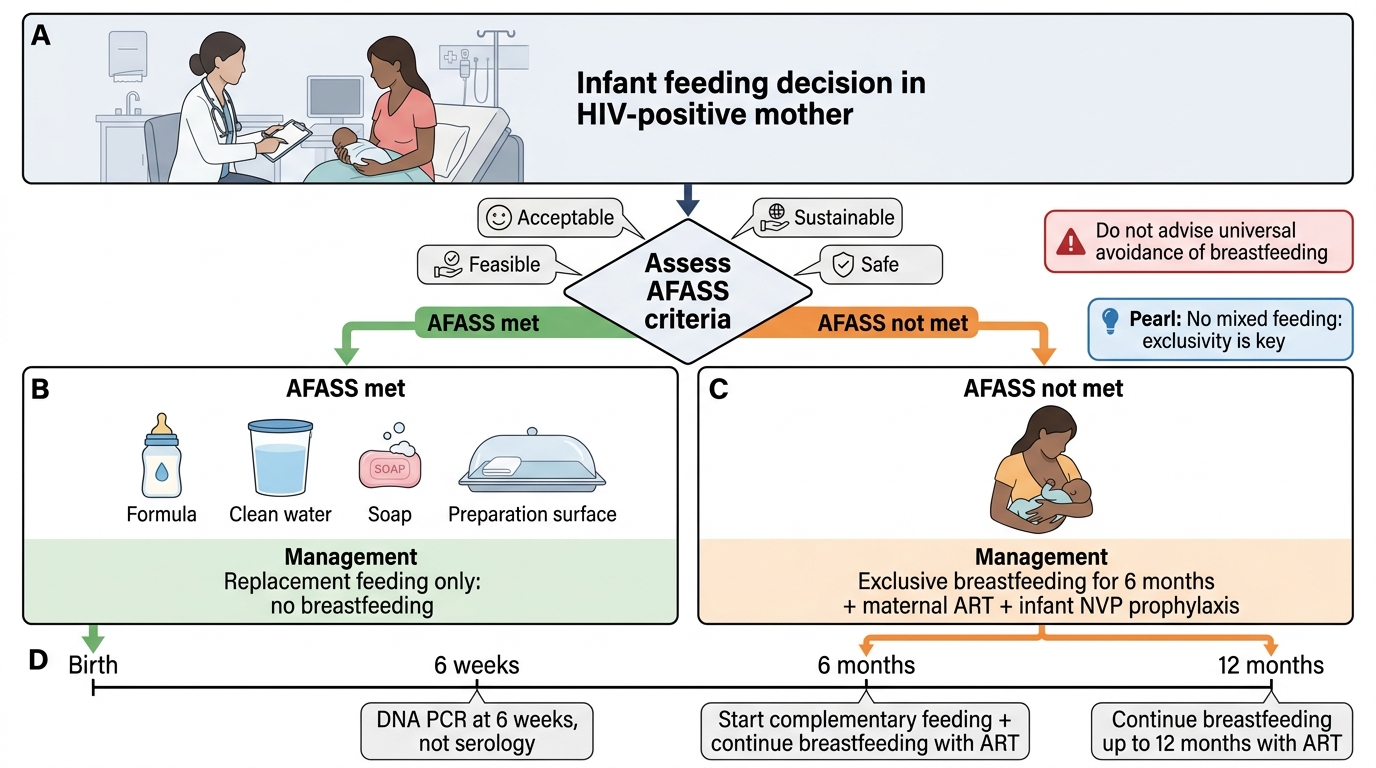
Infant HIV testing uses HIV DNA PCR (not antibody) at 6 weeks of age (because maternal antibodies cross the placenta and persist for 12–18 months — antibody tests are unreliable for infant diagnosis during this period). A positive PCR at 6 weeks confirms infant HIV infection; repeat at 6 and 12 months to confirm clearance if initial test is negative. Final HIV-negative confirmation at 18 months (after maternal antibodies have waned) uses standard serology.
4. Infant Feeding — The AFASS Decision:
This is the most nuanced and frequently misunderstood component. The key principle is that the feeding recommendation is context-specific, not universal:
AFASS criteria evaluate whether replacement feeding is:
- Affordable — family can consistently purchase and prepare formula
- Feasible — clean water available, utensils available, caregiver can prepare feeds hygienically
- Acceptable — socially and culturally acceptable; no stigma from formula-feeding
- Sustainable — can be maintained throughout the recommended duration (6 months of exclusive formula)
- Safe — safe water supply, no risk of contamination and gastroenteritis
If ALL AFASS criteria are met → exclusive replacement feeding (no breastfeeding) from birth. This eliminates postnatal HIV transmission entirely.
If AFASS criteria are NOT fully met (which is the reality for most Indian women in resource-limited settings) → exclusive breastfeeding for the first 6 months + continued breastfeeding with complementary feeding up to 12 months, with the mother on optimally suppressive ART (VL <1,000). The infant receives NVP prophylaxis throughout the breastfeeding period. Mixed feeding (breast + formula) is the WORST option and must be actively discouraged — it increases gut permeability and dramatically increases transmission risk.
When in doubt about AFASS status, the default in India under NACO guidelines is to support and sustain exclusive breastfeeding + maternal ART, which reduces breastfeeding transmission to <2%.
Option B+ PPTCT and AFASS Infant Feeding Algorithm
Infant Feeding Algorithm in HIV-Positive Mother
CLINICAL PEARL
The AFASS feeding pearl: The most common error students (and clinicians) make is to advise ALL HIV-positive women to avoid breastfeeding. This is WRONG in India for most women. Replacement feeding requires safe water, consistent formula supply, and hygienic preparation — in many rural and urban-poor settings, formula feeding carries its own significant mortality risk (gastroenteritis, malnutrition from under-dilution, inability to sustain supply). NACO guidelines explicitly state: if AFASS criteria are NOT met, exclusive breastfeeding + maternal ART reduces HIV transmission to levels comparable with formula feeding, while avoiding the nutritional and infectious risks of formula. The key is EXCLUSIVITY of breastfeeding (no mixed feeding ever) and maternal viral suppression. Always assess AFASS before advising against breastfeeding — never give a universal 'do not breastfeed' instruction. The second pearl: infant HIV diagnosis requires DNA PCR, not serology, at 6 weeks — maternal IgG antibodies cross the placenta and make serology unreliable in the first 12–18 months of life.
SELF-CHECK
A woman with confirmed HIV on TDF+3TC+EFV since 14 weeks delivers at term. Viral load at 36 weeks was 280 copies/mL. She lives in a rural village with no reliable clean water source. What is your FIRST feeding recommendation?
A. Exclusive replacement feeding (no breastfeeding) — she is on ART so formula is always preferred
B. Mixed feeding — breastfeed and supplement with formula to reduce HIV dose
C. Exclusive breastfeeding + continue maternal ART — AFASS criteria for replacement feeding are not met
D. Breastfeed for 1 month only, then switch to formula
Reveal Answer
Answer: C. Exclusive breastfeeding + continue maternal ART — AFASS criteria for replacement feeding are not met
AFASS criteria (Affordable, Feasible, Acceptable, Sustainable, Safe) are NOT met for this woman — no reliable clean water means replacement feeding carries high gastroenteritis risk. NACO guidelines recommend exclusive breastfeeding + maternal ART (which has reduced her VL to 280 <1,000 copies/mL) — this carries <2% transmission risk and avoids the dangers of formula feeding in resource-limited settings. Mixed feeding is the WORST option (damages gut mucosa, dramatically increases transmission). Formula is not 'always preferred' for women on ART — AFASS assessment is mandatory.
SELF-CHECK
A baby born to an HIV-positive mother at 38 weeks appears healthy. What is the correct test and timing for the FIRST infant HIV diagnostic test?
A. HIV ELISA antibody test at 6 weeks of age
B. HIV DNA PCR at 6 weeks of age
C. HIV ELISA antibody test at 18 months of age
D. HIV viral load (RNA) test at delivery
Reveal Answer
Answer: B. HIV DNA PCR at 6 weeks of age
Maternal HIV IgG antibodies cross the placenta and persist in the infant for 12–18 months — making antibody-based tests (ELISA/serology) unreliable for infant diagnosis during this period. The correct test is HIV DNA PCR (polymerase chain reaction on whole blood), which detects viral genetic material and is not confounded by maternal antibodies. The first PCR is performed at 6 weeks of age. Final HIV-negative confirmation at 18 months uses standard serology after maternal antibodies have waned.
Self-Assessment — HIV in Pregnancy
This self-assessment consolidates your understanding of the NACO PPTCT programme across its four core components: universal opt-out testing and diagnosis, initiation of Option B+ ART and monitoring, viral-load-guided mode of delivery decision-making, and the context-specific infant prophylaxis and feeding counselling that form the backbone of preventing mother-to-child transmission. The scenarios below reflect real presentations that you will encounter in teaching hospitals, district hospitals, and community health settings in India — the woman who was screened and started on ART early, and the woman who arrives at term without prior ANC, having fallen through the gaps of the healthcare system. Working through both scenarios will sharpen your decision-making for both the 'ideal' and the 'real' PPTCT encounter. Attempt all five questions systematically before checking the answers.
Scenario A: Sunita is HIV-positive, diagnosed at 18 weeks on routine ANC screening. CD4 is 320 cells/µL, VL is 8,400 copies/mL. She is started on TDF+3TC+EFV immediately. At 36 weeks, her repeat VL is 420 copies/mL. She asks if she needs a caesarean section.
- What mode of delivery would you recommend and why?
- Which infant prophylaxis regimen applies?
- On what day of the infant's life should the first HIV DNA PCR be performed?
Scenario B: Meera is an HIV-positive woman who was not on ART during pregnancy (lost to follow-up). She presents in active labour at 39 weeks. VL is unknown. She delivers vaginally.
- What infant prophylaxis regimen does this baby require?
- What feeding advice do you give if Meera lives in urban Chennai in adequate socioeconomic conditions?
Self-check answers: A1: VL 420 <1,000 copies/mL → vaginal delivery acceptable; monitor for prolonged ROM, avoid invasive fetal monitoring. A2: Standard low-risk regimen — NVP for 6 weeks (VL suppressed, mother on ART throughout). A3: HIV DNA PCR at 6 weeks of age. B4: High-risk regimen — NVP+AZT for 12 weeks (mother not on ART at delivery, VL unknown). B5: AFASS criteria likely met in urban Chennai with adequate socioeconomic conditions → exclusive replacement feeding (no breastfeeding) from birth is recommended; counsel on hygienic formula preparation and stress no mixed feeding ever.