Page 16 of 38
OG12.6 | Liver Disease in Pregnancy — SDL Guide
Learning Objectives
- Classify liver diseases complicating pregnancy by aetiology and trimester of onset
- Describe the clinical features, pathophysiology, and maternal-fetal impact of intrahepatic cholestasis of pregnancy (ICP), acute fatty liver of pregnancy (AFLP), and HELLP syndrome
- Explain why hepatitis E is uniquely dangerous in pregnancy
- Apply diagnostic criteria (Swansea criteria, bile acid thresholds) and interpret relevant investigations
- Outline the management of ICP, AFLP, HELLP, and viral hepatitis in pregnancy including timing of delivery
INSTRUCTIONS
Liver disease in pregnancy ranges from the common but distressing itch of obstetric cholestasis to the life-threatening triad of AFLP and HELLP syndrome. Recognising which condition you are dealing with — and in which trimester — determines whether a woman lives or dies, and whether her baby survives. This module takes you through a trimester-anchored clinical framework, the distinctive biochemical fingerprints of each condition, and the management principles that have transformed outcomes in modern obstetric care.
References
- DC Dutta's Textbook of Obstetrics, 9th ed., Ch 18 — Medical Disorders in Pregnancy (textbook)
- Williams Obstetrics, 26th ed., Ch 55 — Hepatic, Biliary, and Pancreatic Disorders (textbook)
- RCOG Green-top Guideline No. 43 — Obstetric Cholestasis (2011, updated 2022) (guideline)
- Williamson C et al. Intrahepatic Cholestasis of Pregnancy. Lancet 2023 (journal)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 30-year-old primigravida at 34 weeks gestation presents to the antenatal clinic with a two-week history of intense itching — worse on the palms and soles at night, disturbing her sleep. She has no rash. Her serum bile acids return at 58 µmol/L and ALT is 120 IU/L. The same evening, a 28-year-old multigravida at 36 weeks arrives in the emergency room with acute-onset right upper quadrant pain, vomiting, jaundice, and confusion. Her platelets are 48×10⁹/L, AST 980 IU/L, and her blood glucose is 1.8 mmol/L. Both women have 'liver disease in pregnancy' — but they need completely different management, and one of them is in imminent danger of dying. How do you tell them apart, and what do you do in the next thirty minutes?
WHY THIS MATTERS
Liver disorders complicate approximately 3–5% of all pregnancies. While most cases are mild, conditions such as AFLP and HELLP syndrome carry maternal mortality rates of 1–18% without prompt diagnosis and delivery. Intrahepatic cholestasis of pregnancy (ICP) — the most common pregnancy-specific liver disorder — is treatable but demands timely recognition because bile acids ≥40 µmol/L are associated with a doubling of stillbirth risk. Hepatitis E, endemic in India, kills 20–25% of infected pregnant women compared with only 1–2% in the general population. As a final-year student rotating through obstetric wards in a country where viral hepatitis, tropical infection, and nutritional deficiency are prevalent, you will encounter these conditions and must be the first to recognise them.
RECALL
Before proceeding, recall from your biochemistry studies how bilirubin is processed: unconjugated bilirubin formed from haemoglobin breakdown is transported bound to albumin to the liver, where glucuronyl transferase conjugates it to water-soluble bilirubin diglucuronide for biliary excretion. In HELLP syndrome, haemolysis raises unconjugated bilirubin while hepatocellular injury raises conjugated. Recall from physiology that the liver produces coagulation factors I, II, V, VII, IX, X and XIII — so acute hepatic failure rapidly uncouples haemostasis. Recall also from your pre-eclampsia studies that BP ≥140/90 after 20 weeks is the defining threshold, because HELLP syndrome lies on that spectrum.
A Pregnant Woman with Jaundice — Who Is at Risk?
The clinical presentation of liver disease in pregnancy is shaped by the trimester in which it occurs and whether the condition is pregnancy-specific or coincidental. Understanding the trimester pattern is the most powerful first-line filter at the bedside.
In the first trimester, the predominant liver disturbance is hyperemesis gravidarum (HG) — intractable nausea and vomiting causing fluid and electrolyte loss, ketonaemia, and in severe cases hepatocellular injury with mild transaminase elevation (typically <300 IU/L) and conjugated hyperbilirubinaemia. HG is a diagnosis of exclusion that resolves with the first trimester; it rarely causes frank jaundice.
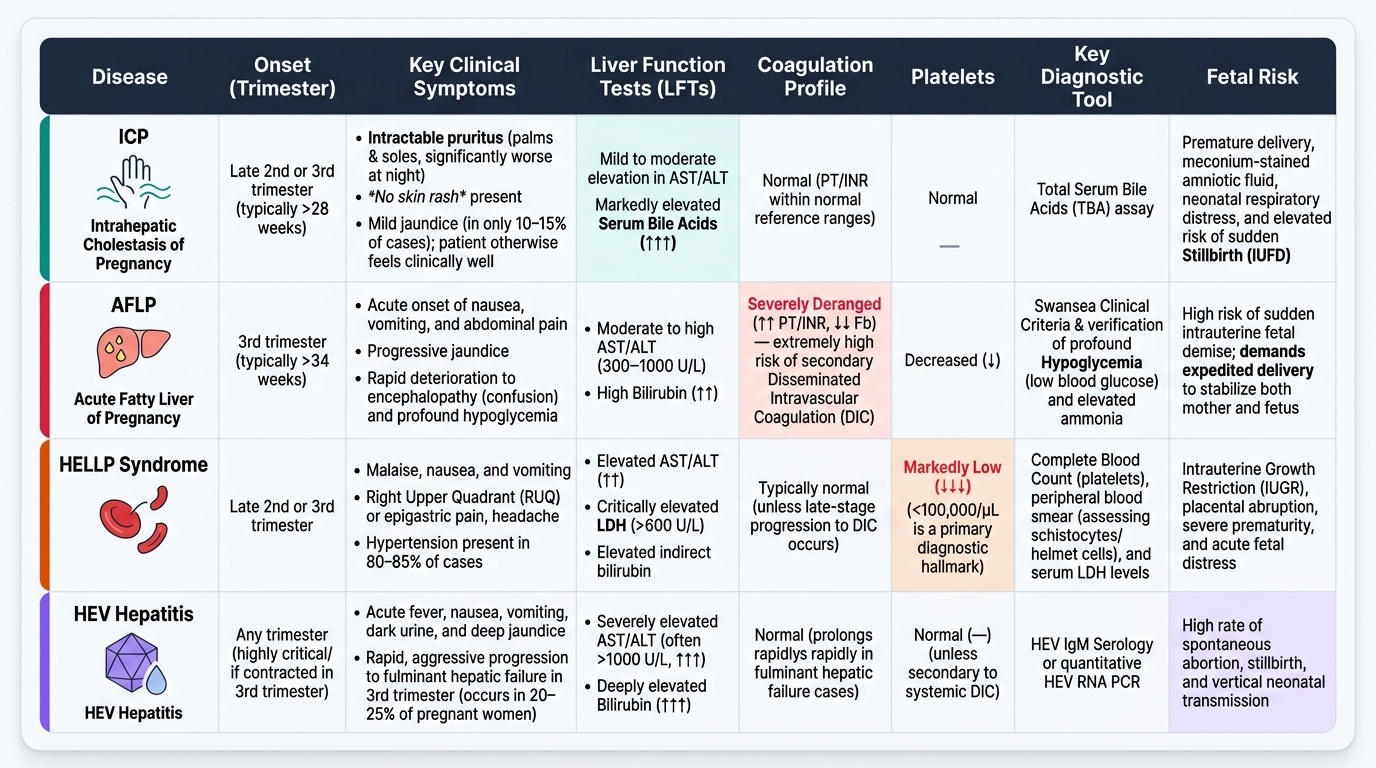
In the second and third trimesters, the pregnancy-specific disorders dominate. Intrahepatic cholestasis of pregnancy (ICP), also called obstetric cholestasis, typically presents after 28 weeks with intractable pruritus — worst on the palms and soles, particularly at night — without a primary skin rash. The itch is caused by the deposition of bile acids in the skin. Jaundice occurs in only 10–15% of cases. The woman often appears well between the itching episodes. On the severe end of the spectrum, HELLP syndrome presents with malaise, nausea, vomiting, and right upper quadrant or epigastric pain in the late second or third trimester, typically in association with hypertension; 15–20% of HELLP cases occur without pre-eclampsia. Acute fatty liver of pregnancy (AFLP) also presents in the third trimester, often after 34 weeks, with a 1–2-week prodrome of nausea, vomiting, abdominal pain, and progressive jaundice, then rapid deterioration into acute liver failure with coagulopathy, hypoglycaemia, and encephalopathy.
Coincidental liver diseases are present throughout pregnancy. Viral hepatitis — especially hepatitis A (faeco-oral, acute), hepatitis B (blood/vertical, chronic), hepatitis C (blood, chronic), and critically hepatitis E (HEV) — can present at any trimester. HEV deserves special emphasis in the Indian context: it is an RNA virus transmitted via contaminated water, causes an acute icteric illness in the general population, but in pregnant women — particularly in the third trimester — it progresses to fulminant hepatic failure in 20–25% of cases, probably because of pregnancy-induced impairment of cellular immunity and an HEV genotype 1 effect on trophoblast biology. Maternal mortality from HEV in India is among the highest recorded for any infectious cause in pregnancy.
Autoimmune hepatitis, Wilson's disease first presenting in pregnancy, and pre-existing cirrhosis with portal hypertension complete the differential. A simple aide-memoire by trimester:
- T1: Hyperemesis gravidarum; viral hepatitis (any type)
- T2–T3: ICP (from 28 weeks), HELLP (late T2 / T3), viral hepatitis, autoimmune flare
- T3 / peripartum: AFLP (peak 34–36 weeks), HELLP, HEV fulminant hepatitis
IMAPT: the clinical features overlap considerably between AFLP and HELLP — both present with jaundice, abdominal pain, and systemic illness. The history, physical, and a targeted biochemical panel allow differentiation.
Provided image
SELF-CHECK
A 32-year-old woman at 35 weeks gestation presents with severe generalised pruritus (palms/soles, nocturnal) without jaundice or rash. ALT is 95 IU/L and serum bile acids are 62 µmol/L. What is the most likely diagnosis?
A. Acute fatty liver of pregnancy
B. Intrahepatic cholestasis of pregnancy — severe
C. HELLP syndrome
D. Hepatitis E infection
Reveal Answer
Answer: B. Intrahepatic cholestasis of pregnancy — severe
The clinical picture of nocturnal pruritus on palms and soles without a primary rash, elevated bile acids ≥40 µmol/L (here 62 µmol/L = severe range), mild ALT elevation, and normal platelets/coagulation is characteristic of ICP (obstetric cholestasis). AFLP and HELLP would show coagulopathy and thrombocytopaenia respectively. HEV presents with prodromal fever, nausea, and jaundice rather than isolated pruritus.
Why Pregnancy Changes the Liver — Pathophysiology
Normal pregnancy induces a predictable set of hepatic adaptations that, in susceptible women, tip into pathology. Understanding the molecular mechanisms explains both why these disorders are pregnancy-specific and why they resolve (or must be terminated) after delivery.
In ICP, the central mechanism is impaired canalicular bile acid transport. Oestrogen — rising to 100-fold above non-pregnant levels by the third trimester — downregulates the expression and activity of the hepatocanalicular transporters ABCB11 (bile salt export pump, BSEP) and ABCB4 (phospholipid flippase). In genetically predisposed women (heterozygous loss-of-function variants in ABCB4, ABCB11, or ATP8B1 genes), even physiological oestrogen levels overwhelm the remaining transport capacity. The result is intrahepatic cholestasis: serum bile acids accumulate, deposit in the skin (causing pruritus), and — critically — cross the placenta into the fetal circulation. In the fetus, bile acids cause vasoconstriction of chorionic veins, trigger cardiac arrhythmias, and may induce sudden fetoplacental vasoconstriction and stillbirth, a risk that rises sharply above 40 µmol/L.
In AFLP, the pathogenesis involves mitochondrial fatty acid β-oxidation failure. Approximately 20% of AFLP cases are associated with a fetus carrying a homozygous long-chain 3-hydroxyacyl-CoA dehydrogenase (LCHAD) deficiency. The fetus cannot oxidise long-chain fatty acids; these accumulate and are delivered transplacentally to the maternal liver. In the mother — often a heterozygous carrier — the combined metabolic load overwhelms mitochondrial function, causing microvesicular steatosis: fat droplets accumulate within hepatocyte cytoplasm without displacing the nucleus (in contrast to macrovesicular steatosis). The result is global hepatocellular dysfunction: hypoglycaemia (glycogen depletion), coagulopathy (factor synthesis failure), encephalopathy (hyperammonaemia), and renal failure (hepatorenal syndrome). Delivery removes the fetal fatty-acid load and the placenta; the liver can regenerate once the substrate is removed.
In HELLP syndrome, the mechanism is an extension of pre-eclamptic endothelial disease: placental ischaemia triggers systemic endothelial dysfunction, microvascular fibrin deposition, and mechanical haemolysis as red cells are sheared across fibrin strands (microangiopathic haemolytic anaemia, MAHA). The liver is injured by hepatic sinusoidal obstruction with fibrin deposition, leading to periportal haemorrhage and necrosis. Hepatic haematoma or rupture is a rare but catastrophic complication. Because HELLP is a systemic endothelial disease, it overlaps with — but is not synonymous with — severe pre-eclampsia: up to 30% of HELLP cases have no proteinuria.
In hepatitis E in pregnancy, the virus is a non-enveloped RNA virus (Orthohepevirus A, genotype 1 in India) transmitted faeco-orally. In pregnant women, especially the third trimester, an oestrogen-driven T-helper-2 shift in immunity facilitates viral replication; the placenta expresses HEV receptor neuropilin-1 and viral proteins have been detected in trophoblasts. Fulminant hepatic failure with DIC, renal failure, and vertical transmission to the fetus result in rates of maternal and neonatal death that are dramatically higher than in non-pregnant hosts.
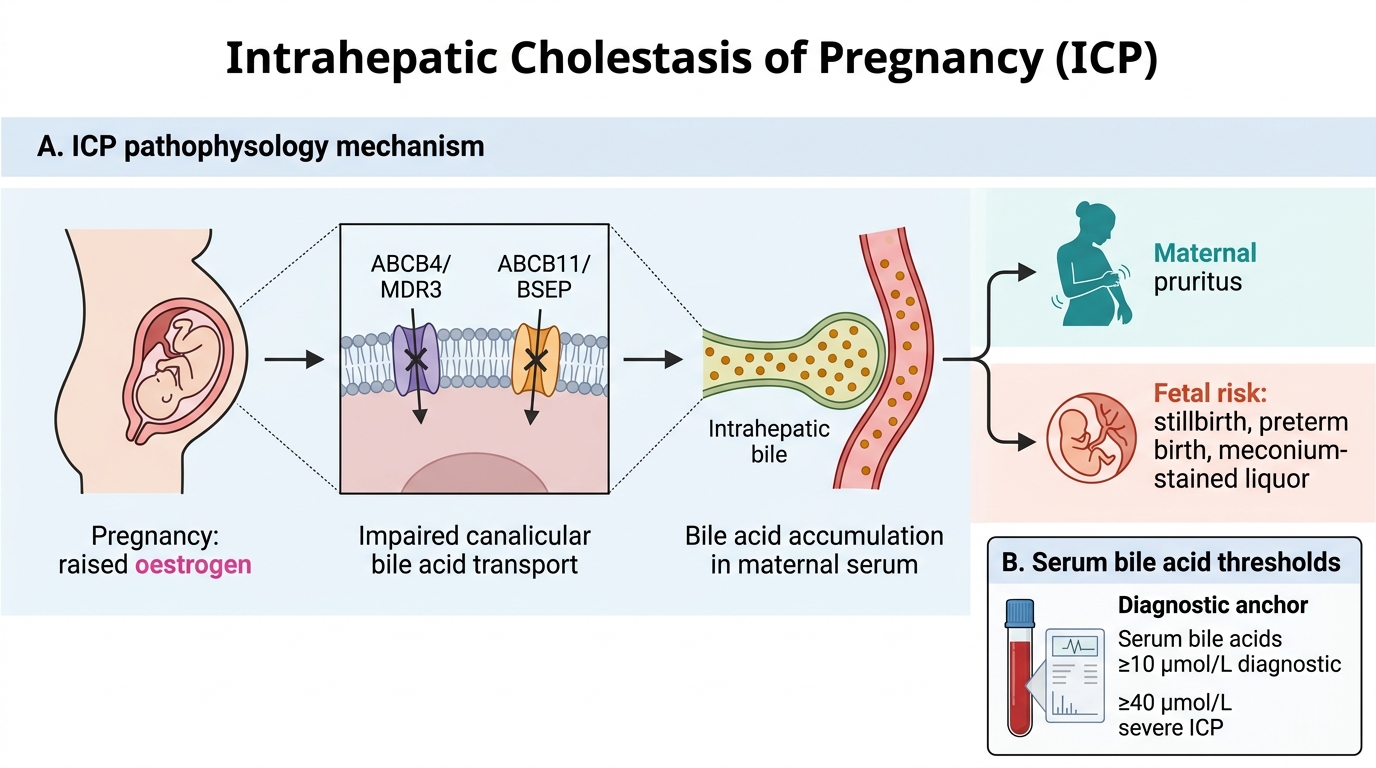
Pathophysiology of Intrahepatic Cholestasis of Pregnancy
Diagnosing Liver Disease in Pregnancy — Investigations
The diagnostic workup for a pregnant woman with suspected liver disease must be both systematic and rapid — in AFLP and HELLP, a delay of hours can be fatal. The history (trimester, symptom onset, hypertension, viral exposure) and examination (BP, epigastric tenderness, icterus, asterixis) immediately narrow the differential, after which targeted investigations confirm the diagnosis.
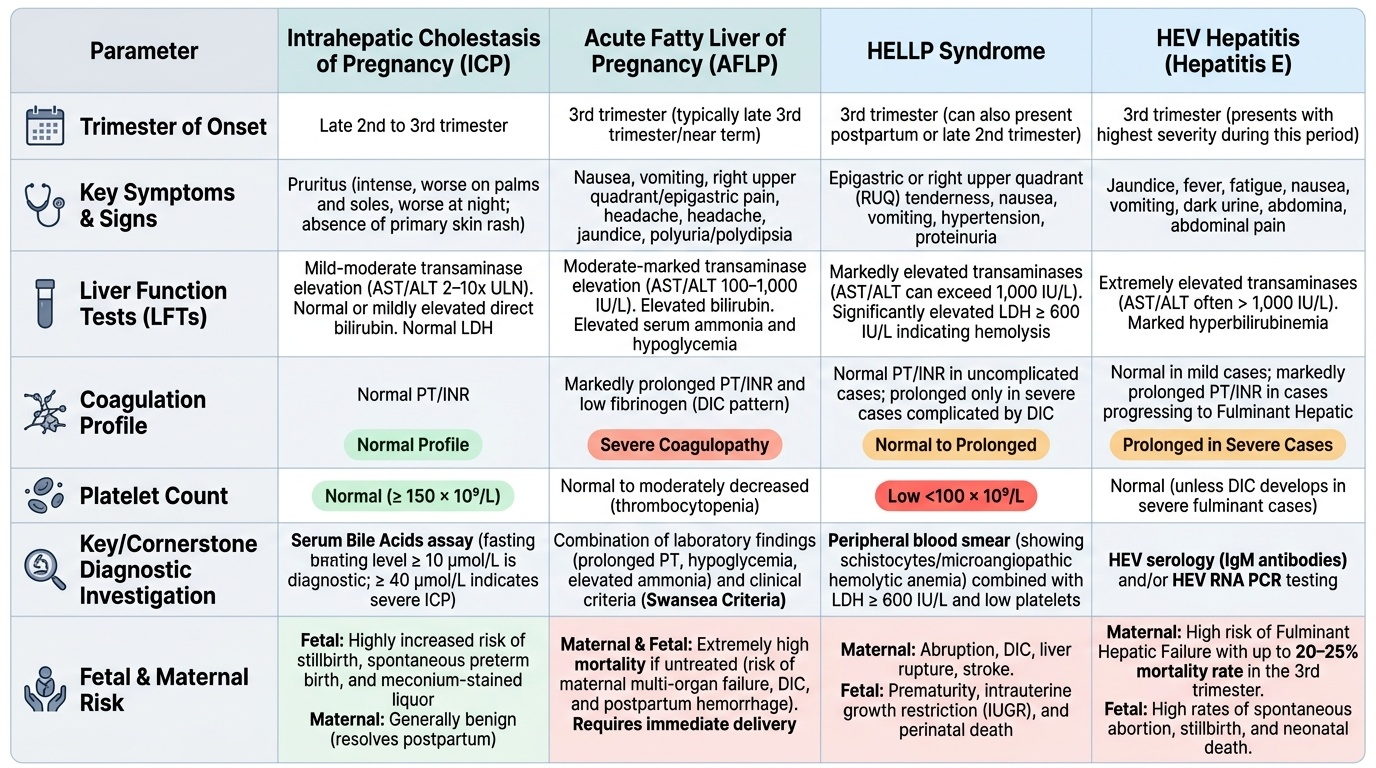
Serum bile acids are the cornerstone investigation for ICP. A fasting level ≥10 µmol/L is diagnostic. The critical threshold is ≥40 µmol/L, which defines severe ICP and is associated with a significantly increased risk of stillbirth, spontaneous preterm birth, and meconium-stained liquor. Bile acid assay requires a dedicated sample (not standard LFTs); in resource-limited settings, the combination of unexplained pruritus + elevated ALT with no alternative explanation supports a clinical diagnosis. ALT/AST are elevated (typically 2–10× ULN) but LDH, platelet count, and coagulation screen are normal in uncomplicated ICP.
Liver function tests (LFTs) in all three pregnancy-specific disorders show transaminase elevation, but the pattern differs:
- ICP: AST/ALT elevated (2–10× ULN), direct bilirubin mildly elevated or normal, normal PT, normal platelets
- HELLP: AST/ALT markedly elevated (can exceed 1,000 IU/L), LDH >600 IU/L (haemolysis marker), platelets <100×10⁹/L, peripheral blood film showing schistocytes (microangiopathic haemolytic anaemia), prolonged PT only in severe cases
- AFLP: AST/ALT elevated (100–1,000 IU/L), elevated bilirubin, markedly prolonged PT/INR, fibrinogen low (DIC pattern), elevated serum ammonia, hypoglycaemia (a distinguishing feature), elevated creatinine
For AFLP, the Swansea criteria provide a validated bedside diagnosis without biopsy. Diagnosis requires ≥6 of the following 14 features:
1. Vomiting
2. Abdominal pain
3. Polydipsia/polyuria
4. Encephalopathy
5. Elevated bilirubin >0.8 mg/dL
6. Hypoglycaemia <72 mg/dL
7. Elevated urate >340 µmol/L
8. Leucocytosis >11×10⁹/L
9. AST/ALT >42 IU/L
10. Ammonia >47 µmol/L
11. Renal impairment (creatinine >150 µmol/L)
12. Coagulopathy (PT >14 sec or APTT >34 sec)
13. Microvesicular steatosis on liver biopsy
14. Ultrasound: echogenic liver (increased echogenicity suggesting fat)
Ultrasound of the liver should be obtained early — echogenic liver supports AFLP, hepatic haematoma may be visible in HELLP. CT abdomen is useful to detect subcapsular haematoma if HELLP-related hepatic rupture is suspected.
Viral serology is mandatory when the diagnosis is unclear: anti-HEV IgM (current infection), HBsAg + anti-HBc IgM (acute hepatitis B), anti-HAV IgM, anti-HCV. HEV-RNA PCR confirms viraemia in early or immunosuppressed cases. A key clinical clue for HEV is an epidemic context (contaminated water supply, monsoon season in India) and rapid progression to jaundice with constitutional symptoms.
Fetal surveillance is an integral part of the workup in any hepatic condition: cardiotocography (CTG) for fetal heart rate monitoring, biophysical profile, and — in ICP — umbilical artery Doppler to assess placental perfusion, though Doppler does not predict the sudden-onset bile-acid-mediated stillbirth unique to ICP.
Provided image
SELF-CHECK
A 29-year-old at 37 weeks gestation has jaundice, epigastric pain, vomiting for 5 days, and confusion since yesterday. Investigations: AST 540 IU/L, bilirubin 4 mg/dL, glucose 44 mg/dL (2.4 mmol/L), PT 22 sec (control 12), platelets 85×10⁹/L, creatinine 210 µmol/L, NH3 65 µmol/L, ultrasound shows echogenic liver. How many Swansea criteria are met?
A. 4 criteria
B. 6 criteria
C. 8 criteria
D. 10 criteria
Reveal Answer
Answer: C. 8 criteria
Counting: vomiting (1), abdominal pain (2), encephalopathy/confusion (3), elevated bilirubin (4), hypoglycaemia <72 mg/dL (5), leucocytosis not stated — skip, elevated AST >42 IU/L (6), elevated ammonia >47 µmol/L (7), renal impairment creatinine >150 µmol/L (8), coagulopathy PT >14 sec (9), US echogenic liver (10). Here at least 8–10 criteria are met (depending on leucocyte count). ≥6 criteria confirms AFLP diagnosis without biopsy.