Page 17 of 38
OG12.6 | Liver Disease in Pregnancy — SDL Guide (Part 2)
Management of Liver Disorders in Pregnancy
The cardinal management principle for pregnancy-specific liver diseases is that delivery is curative — the placenta and fetus are the source of the metabolic insult, and removing them allows hepatic recovery. The timing and urgency of delivery are calibrated to the severity of maternal and fetal compromise.
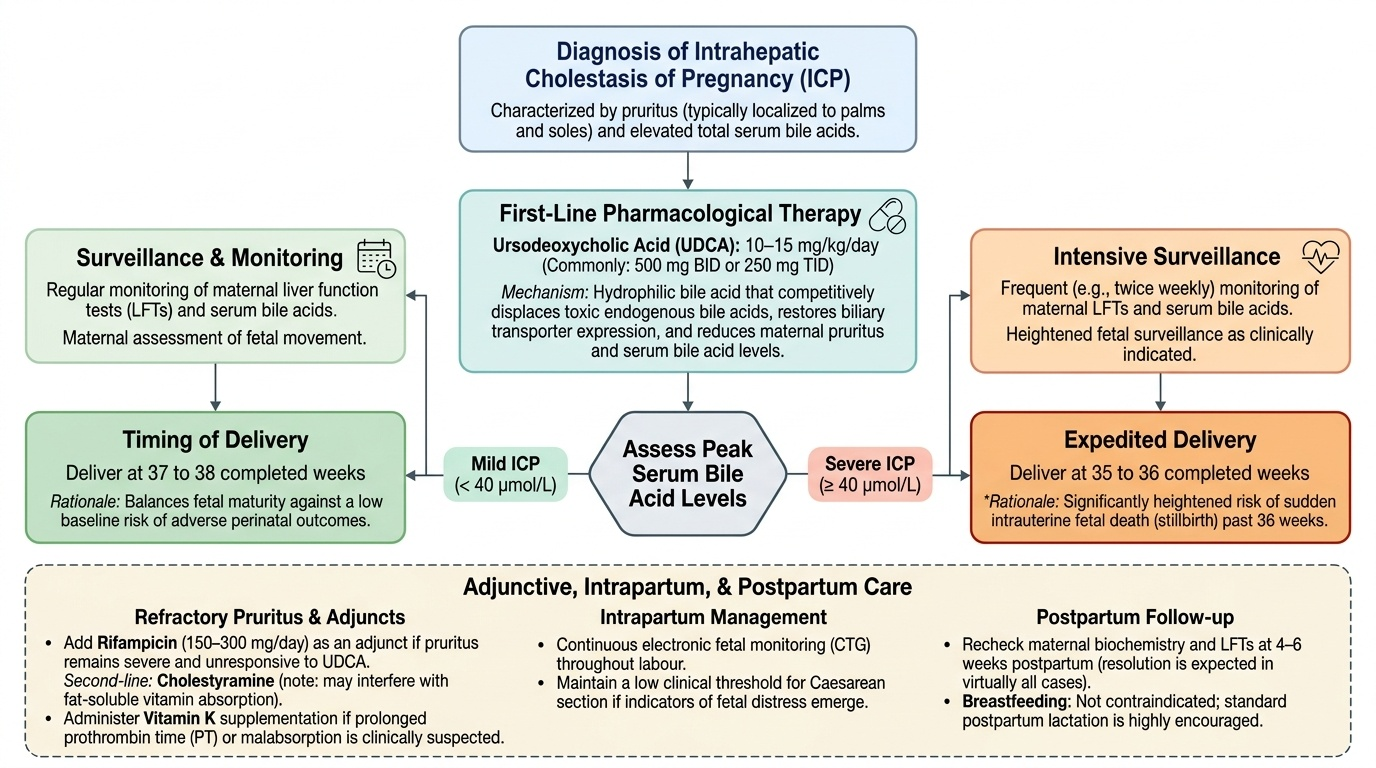
ICP — Intrahepatic Cholestasis of Pregnancy:
Ursodeoxycholic acid (UDCA) is the standard pharmacological treatment at a dose of 10–15 mg/kg/day (typically 500 mg twice daily or 250 mg three times daily). UDCA is a hydrophilic bile acid that competitively displaces toxic endogenous bile acids, restores biliary transporter expression, and reduces both pruritus and serum bile acid levels. The PITCH trial (2019, UK) showed that UDCA significantly reduced pruritus and improved biochemical markers but did not demonstrate a statistically significant reduction in composite adverse perinatal outcome; however, UDCA remains standard of care due to its safety profile and symptom benefit. Rifampicin (150–300 mg/day) may be added for refractory pruritus; cholestyramine is second-line and interferes with fat-soluble vitamin absorption. Vitamin K supplementation is important if prolonged PT is suspected due to malabsorption.
Delivery timing is determined by severity. For mild ICP (bile acids <40 µmol/L), delivery at 37–38 completed weeks is standard; severe ICP (bile acids ≥40 µmol/L) warrants delivery at 35–36 weeks due to heightened stillbirth risk. Continuous CTG in labour, with low threshold for caesarean section, is appropriate. Breastfeeding is not contraindicated; symptoms and biochemistry resolve within 4–6 weeks postpartum in virtually all cases.
AFLP — Acute Fatty Liver of Pregnancy:
AFLP is a medical emergency. The moment the diagnosis is suspected (Swansea criteria ≥6), the management is simultaneous stabilisation and expedited delivery, regardless of gestational age. Delivery removes the fetal LCHAD-deficient metabolic substrate from the maternal circulation.
- Correct hypoglycaemia with 10% dextrose infusions (monitor glucose hourly)
- Correct coagulopathy with fresh frozen plasma (FFP) and cryoprecipitate; platelet transfusion for counts <50×10⁹/L before delivery
- Manage hepatic encephalopathy: lactulose, low-protein diet, avoid sedatives
- Renal support: fluid balance, avoid nephrotoxic drugs, early nephrology involvement
- Deliver by the most expedient route — caesarean section if vaginal delivery not imminent; regional anaesthesia may be hazardous with coagulopathy
- Postpartum: liver function recovers in 1–4 weeks; the neonate should be tested for LCHAD deficiency (urine organic acids, acylcarnitine profile) as prompt dietary management prevents metabolic crises in the infant
HELLP Syndrome:
HELL is managed within the framework of pre-eclampsia (refer to cluster og6-hdp for detailed MgSO₄ regimens and antihypertensives). Specific additional points:
- Corticosteroids: dexamethasone IV (10 mg 12-hourly) or betamethasone for fetal lung maturity if <34 weeks; high-dose dexamethasone for platelet count recovery is controversial and not universally recommended
- Delivery: is the definitive treatment; delivery recommended once BP and coagulopathy are stabilised; ≥34 weeks = deliver promptly; <34 weeks = consider 24–48 h of corticosteroids first if mother is stable, then deliver
- Avoid NSAIDs (worsen platelet dysfunction); avoid ergometrine (contraindicated in hypertension — use oxytocin 10 IU IM or IV)
- Watch for hepatic haematoma: sudden shoulder-tip pain, increasing haemoperitoneum on USS — may require interventional radiology or surgery
Viral Hepatitis in Pregnancy:
- Hepatitis A: supportive; notify public health; no antiviral treatment; vaccination safe in pregnancy
- Hepatitis B: if acute HBV with fulminant features → tenofovir; in chronic HBV, begin tenofovir ≥28 weeks to reduce vertical transmission (especially if HBV DNA >200,000 IU/mL); neonatal HBV vaccine + HBIG within 12 h of birth
- Hepatitis C: antiviral therapy (DAA) deferred until after delivery; no neonatal prophylaxis available; breastfeeding allowed if no nipple cracking/bleeding
- Hepatitis E (India): supportive care is the mainstay; the woman is likely to require ICU-level care for fulminant hepatic failure — hypoglycaemia, coagulopathy (FFP, cryoprecipitate), renal support, lactulose; expedite delivery in late third-trimester HEV as removing the immunological burden of the fetoplacental unit may improve outcomes, though timing is controversial; no vaccine licensed in India (a Chinese vaccine, Hecolin, is not yet available); notify public health for water-source investigation
Provided image

AFLP vs HELLP Syndrome in Pregnancy
CLINICAL PEARL
The AFLP–HELLP differentiation pearl: Both present with jaundice, abdominal pain, and systemic illness in the third trimester. The key discriminators are: (1) Hypoglycaemia is a hallmark of AFLP (hepatocyte failure exhausting glycogen stores) but NOT of HELLP; check the blood glucose at the bedside immediately. (2) Thrombocytopaenia and microangiopathic haemolysis (raised LDH + schistocytes) are the dominant haematological feature of HELLP; in AFLP, the coagulopathy pattern is DIC with prolonged PT/APTT + low fibrinogen. (3) HELLP usually has accompanying hypertension; AFLP may have normal BP. (4) Encephalopathy and elevated ammonia point to AFLP. Clinically, treat both as obstetric emergencies requiring immediate delivery — the distinction guides supportive care but not the urgency of delivery. Additionally: Hepatitis E in pregnancy must always be considered in an Indian woman with acute jaundice — do not assume viral hepatitis is benign; take an epidemic/water-supply history.
SELF-CHECK
A woman with HELLP syndrome at 36 weeks requires oxytocin for the third stage of labour. Her BP is 158/102 mmHg. Which uterotonic is CONTRAINDICATED?
A. Oxytocin 10 IU IM
B. Misoprostol 800 µg sublingually
C. Ergometrine 0.5 mg IM
D. Carboprost 250 µg IM
Reveal Answer
Answer: C. Ergometrine 0.5 mg IM
Ergometrine (and methylergometrine) is contraindicated in hypertension and pre-eclampsia because its vasoconstrictive action can precipitate hypertensive crisis, stroke, and acute pulmonary oedema. HELLP is on the pre-eclampsia spectrum — ergometrine is absolutely contraindicated. Oxytocin 10 IU IM is the first-line uterotonic of choice; misoprostol is acceptable if oxytocin is unavailable. Carboprost (PGF2α) is contraindicated in asthma but not in hypertension.
SELF-CHECK
What is the serum bile acid threshold that defines SEVERE intrahepatic cholestasis of pregnancy (ICP) and is associated with significantly increased stillbirth risk?
A. ≥10 µmol/L
B. ≥20 µmol/L
C. ≥40 µmol/L
D. ≥80 µmol/L
Reveal Answer
Answer: C. ≥40 µmol/L
The diagnostic threshold for ICP is serum bile acids ≥10 µmol/L. The SEVERE threshold — associated with a clinically important increase in risk of stillbirth, spontaneous preterm birth, and meconium passage — is ≥40 µmol/L. Women with bile acids ≥40 µmol/L should be delivered at 35–36 weeks rather than 37–38 weeks. The 80 µmol/L threshold is not a separate clinical category used in guidelines.
Self-Assessment — Liver Disease in Pregnancy
Self-assessment consolidates the clinical reasoning you have built through this module. The scenarios below are drawn from real-world presentations: an undiagnosed woman deteriorating in the third trimester, a chronic hepatitis B carrier approaching delivery, and the integration of investigative findings into an immediate management plan. Work through each scenario systematically — apply the Swansea criteria formally before checking the answers, and verify your recall of serum bile acid thresholds, antiviral timing, and neonatal prophylaxis protocols. These are exactly the questions that appear in written examinations and viva voce assessments for obstetric medicine.
Scenario A: A 26-year-old primigravida at 33 weeks presents with a 3-day history of nausea, vomiting, right upper quadrant pain, and progressive jaundice. Her BP is 118/76 mmHg (no hypertension). Investigations: AST 420 IU/L, glucose 2.2 mmol/L (40 mg/dL), PT 19 seconds (control 12), platelets 110×10⁹/L, creatinine 180 µmol/L, ammonia 55 µmol/L, serum bile acids 8 µmol/L, ultrasound shows bright (echogenic) liver. The anti-HEV IgM is negative.
- What is the diagnosis? How many Swansea criteria are met?
- What is the immediate management priority?
- What neonatal investigation should be requested after delivery?
Scenario B: A 34-year-old with known hepatitis B (HBsAg positive, HBV DNA 350,000 IU/mL) presents at 30 weeks gestation. She is currently on no antiviral therapy.
- At what gestational age should you consider initiating antiviral therapy and which agent is preferred?
- What should the neonate receive within 12 hours of birth to prevent vertical transmission?
Scenario C (self-check): Review the Swansea criteria listed in this module. Practice applying them to the scenario in question A and count the criteria systematically before reading the answer.
Self-check answers: A1: AFLP; criteria met include vomiting (1), abdominal pain (2), elevated bilirubin (3), hypoglycaemia glucose <72 mg/dL [2.2 mmol/L here] (4), AST >42 (5), ammonia >47 µmol/L (6), renal impairment creatinine >150 µmol/L (7), coagulopathy PT >14 sec (8), echogenic US (9) — ≥9 criteria, easily ≥6 confirming AFLP. A2: Expedite delivery + correct hypoglycaemia (10% dextrose infusion) + FFP for coagulopathy + ICU support. A3: LCHAD deficiency screen — urine organic acids and acylcarnitine profile on the neonate. B4: Tenofovir from 28 weeks gestation (given DNA >200,000 IU/mL). B5: HBV vaccine + hepatitis B immunoglobulin (HBIG) within 12 hours of birth.