Page 1 of 17
OG16.1 | Post-Partum Haemorrhage — SDL Guide
Learning Objectives
- Define postpartum haemorrhage and classify it as primary or secondary using standard criteria
- Enumerate the causes of PPH using the 4 T's framework (Tone, Tissue, Trauma, Thrombin)
- Describe the components of Active Management of the Third Stage of Labour (AMTSL) and identify oxytocin as the uterotonic of choice
- Select appropriate uterotonics for PPH management with correct doses, routes, and contraindications
- Outline the stepwise management of PPH from medical therapy through surgical escalation
- Justify the appropriate use of blood and blood products including massive transfusion protocols in severe PPH
INSTRUCTIONS
Postpartum haemorrhage is the leading cause of maternal mortality worldwide, accounting for approximately 27% of maternal deaths globally and a significant proportion in India. Understanding PPH — from its predictable risk factors and preventable causes to its stepwise medical and surgical management — is an essential competency for every obstetric practitioner. This module guides you through the clinical recognition, pathophysiology, evidence-based prevention, and comprehensive management of PPH including appropriate blood product use, preparing you to act decisively when minutes matter.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Ch. 22 (textbook)
- Williams Obstetrics, 26th edition, Ch. 41 (Obstetric Haemorrhage) (textbook)
- WHO Recommendations for the Prevention and Treatment of Postpartum Haemorrhage, 2012 (guideline)
- FOGSI Good Clinical Practice Recommendation: Management of PPH, 2020 (guideline)
- WOMAN trial (Shakur-Still et al., Lancet 2017) — tranexamic acid in PPH (journal)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 2 AM. A 28-year-old woman, G3P2, has just delivered vaginally at 38 weeks after a prolonged second stage. Thirty minutes after delivery the nurse calls you urgently: the uterus is soft, not contracting, and blood is pooling rapidly on the delivery table. Estimated blood loss so far is approximately 600 mL and the patient is anxious, her pulse is 110 per minute, blood pressure 96/62 mmHg. Her two previous deliveries were uncomplicated. The placenta has been delivered and appears complete. What is happening? What do you do — and in what order? In the next 60 minutes you will learn to answer those questions decisively, drawing on the four causes of PPH, the evidence-based management ladder, and the pharmacology of uterotonics.
WHY THIS MATTERS
Postpartum haemorrhage is the single most common cause of maternal mortality worldwide, responsible for roughly one maternal death every four minutes globally. In India, haemorrhage accounts for approximately 38% of all maternal deaths, a rate disproportionately high because most deaths occur in settings where oxytocin administration and blood transfusion services are delayed or absent. As a final-year student entering clinical practice in any setting — district hospital, medical college, or community health centre — you will encounter PPH. The management decisions you make in the first 30 minutes are the ones that save lives. This module gives you the framework to make those decisions correctly: causes you can anticipate antenatally, prevention you can implement routinely, and a stepwise treatment plan you can execute under pressure.
RECALL
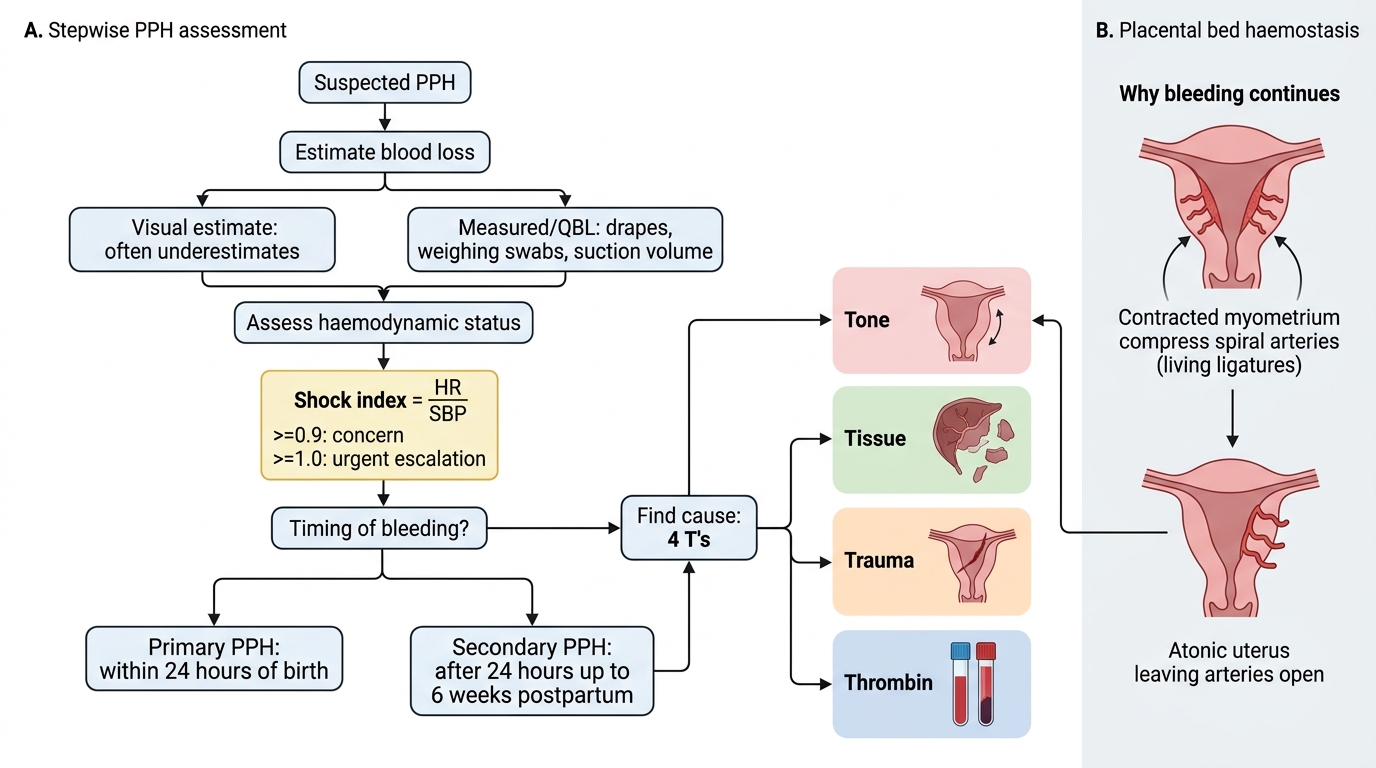
Before we proceed, ground yourself in these prerequisites. Recall that haemostasis following placental separation depends on two mechanisms: myometrial contraction, which mechanically compresses the spiral arteries supplying the placental bed (the 'living ligatures'), and activation of the coagulation cascade at the wound surface. When myometrial contraction fails — as in uterine atony — the spiral arteries remain open and uncontrolled haemorrhage follows. Recall also the normal third stage of labour: after delivery of the baby, uterine retraction causes shearing of the placenta from the decidua basalis, followed by retroplacental haematoma formation and expulsion of the placenta within 30 minutes. A uterus that does not retract, or in which placental fragments are retained, cannot achieve haemostasis by either mechanism. Finally, recall from your pharmacology that oxytocin is a nonapeptide synthesised in the hypothalamus and released from the posterior pituitary; it acts on myometrial oxytocin receptors to produce rhythmic contractions, and its synthetic form can be administered intramuscularly or intravenously to achieve the same effect.
Clinical Presentation of PPH
Postpartum haemorrhage (PPH) is defined as blood loss of ≥500 mL following a vaginal delivery, or ≥1000 mL following caesarean section, within 24 hours of delivery. Clinically, however, any amount of blood loss that causes haemodynamic instability — irrespective of the measured volume — meets the threshold for treatment; visual estimation consistently underestimates true loss by 30–50%. Primary PPH occurs within the first 24 hours after delivery; it is more common and more dangerous, accounting for the majority of PPH-related mortality. Secondary PPH (also called delayed PPH) occurs between 24 hours and 12 weeks postpartum, most commonly between days 8 and 14, and typically results from retained products of conception or endometritis rather than uterine atony.
The haemodynamic presentation depends on the rate and volume of blood loss. Mild hypovolaemia (500–1000 mL loss, Class I shock) may present with tachycardia alone; moderate loss (1000–1500 mL, Class II) produces pallor, diaphoresis, and narrowing pulse pressure; severe loss (>1500 mL, Class III–IV) causes hypotension, altered consciousness, and oliguria. The shock index (heart rate ÷ systolic blood pressure) is a rapid bedside tool: a value >1.0 reliably identifies haemodynamic compromise requiring immediate transfusion, and >1.7 signals life-threatening haemorrhage. All clinical signs may be delayed in young, healthy women with excellent physiological reserve — do not wait for hypotension before acting.
The clinical differential diagnosis of PPH is usefully organised by the 4 T's mnemonic:
- Tone (uterine atony) — the uterus is soft, boggy, and fails to contract; responsible for 70–80% of all PPH cases
- Tissue (retained placenta or membranes) — incomplete placenta or membranes on inspection; placenta accreta spectrum prevents separation
- Trauma (genital tract lacerations) — tears of the cervix, vagina, or perineum; uterine rupture or inversion
- Thrombin (coagulation failure) — pre-existing coagulopathy, DIC complicating severe haemorrhage, amniotic fluid embolism
In any PPH presentation, assess all four causes simultaneously rather than assuming atony until other causes are excluded.
Stepwise Assessment of Postpartum Haemorrhage
Pathophysiology: Why the Uterus Bleeds
Understanding why PPH occurs requires understanding the normal physiology of haemostasis at the placental bed. At term, blood flow through the uteroplacental circulation is approximately 600–800 mL per minute — an enormous volume sustained by the low-resistance intervillous space. Following placental expulsion, haemostasis depends almost entirely on myometrial contraction: the oblique and transverse uterine muscle fibres, arranged in a figure-of-eight pattern around the blood vessels, act as 'living ligatures' — as they shorten they mechanically compress the open spiral arteries at the placental site. A soft, non-contracting uterus (atony) leaves these vessels patent and bleeding continues at the full cardiac-output rate.
Uterine atony — the cause of 70–80% of primary PPH — results from factors that impair myometrial contractility: overdistension (multiple pregnancy, polyhydramnios, macrosomia), exhaustion from prolonged or rapid labour, halogenated anaesthetic agents (halothane, isoflurane) which directly relax uterine muscle, magnesium sulphate used in pre-eclampsia management, and structural anomalies such as fibroids. Grand multiparity is a risk factor because repeated pregnancies reduce the proportion of functional myometrial fibres through fibrosis.
Retained placenta or membranes prevent the placental site from contracting down. A complete placenta that fails to deliver within 30 minutes of the baby (prolonged third stage) accounts for 5–10% of PPH; abnormal placentation (placenta accreta, increta, percreta) — increasingly common with prior uterine surgery — causes a defect of the decidua basalis that prevents physiological separation and can result in massive, life-threatening haemorrhage.
Genital tract trauma — cervical, vaginal, or perineal lacerations — bleeds from torn blood vessels independent of uterine tone. These are particularly important causes when the uterus appears well contracted but bleeding continues (diagnose by careful inspection under good light). Uterine rupture presents with acute haemorrhage, fetal distress, and loss of uterine contour; it is a surgical emergency.
Coagulation failure either pre-exists (e.g. von Willebrand disease, ITP, antiphospholipid syndrome) or develops secondary to massive haemorrhage as a consumptive coagulopathy. Disseminated intravascular coagulation (DIC) can be triggered by placental abruption, amniotic fluid embolism, and sepsis, and creates a vicious cycle: coagulopathy prevents haemostasis, haemorrhage worsens, and DIC deepens.
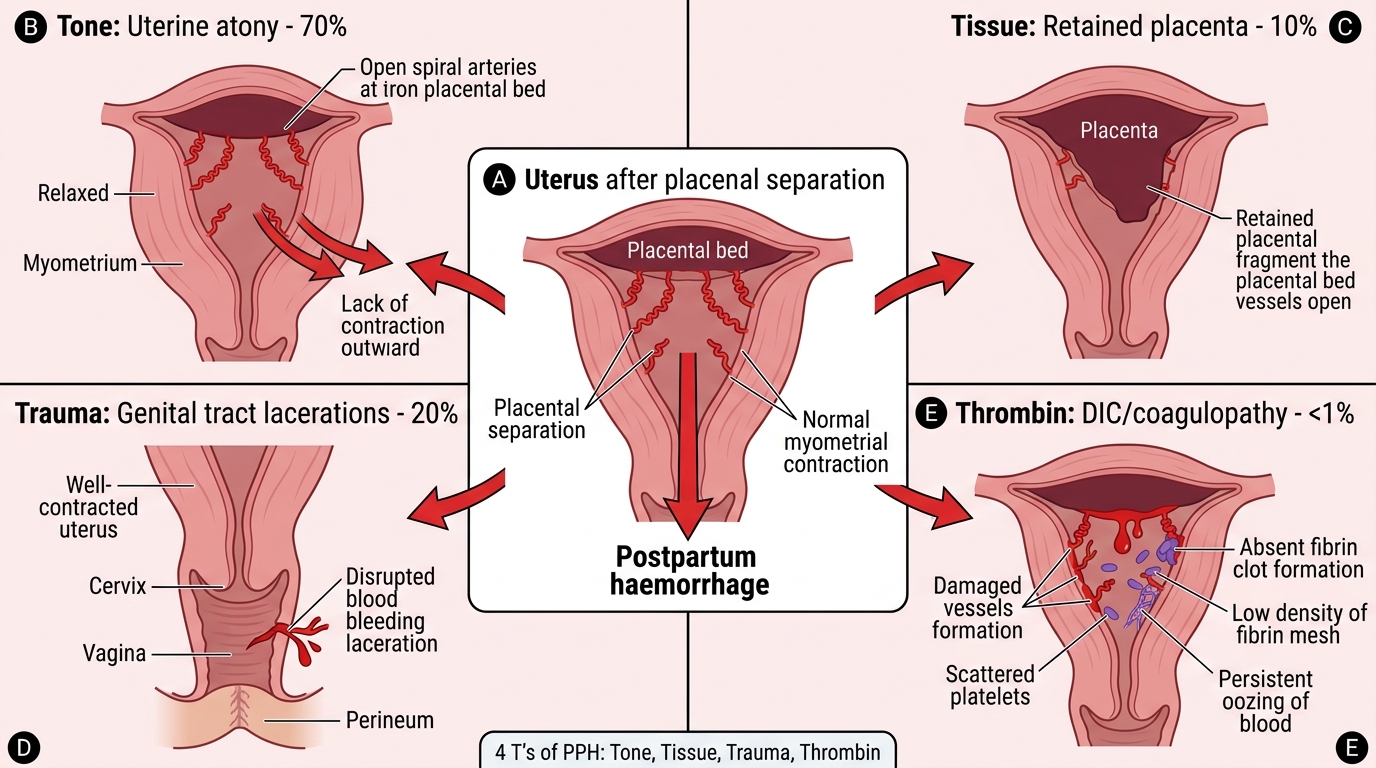
Four Pathways of Postpartum Haemorrhage: The 4 T's
Risk Factors and Prevention — AMTSL
Prevention is the most effective intervention against PPH mortality. Risk factors can be stratified by when they are identified:
Antenatal risk factors include grand multiparity (≥5 deliveries), previous PPH or retained placenta, placenta praevia or placenta accreta, multiple pregnancy (twins, triplets), polyhydramnios, large-for-gestational-age fetus, anaemia (Hb <8 g/dL — a woman who bleeds from a low baseline has less physiological reserve), uterine fibroids, and coagulation disorders. Every antenatal booking should document these; women at high risk should deliver in centres with blood bank and surgical facilities.
Intrapartum risk factors include prolonged first or second stage of labour, precipitate labour, oxytocin augmentation (downregulates receptors — less effective uterotonic after delivery), instrumental delivery (forceps or vacuum), general anaesthesia, and manual removal of placenta.
Identifying risk factors is important, but it has limited predictive value: up to 40% of PPH cases occur in women with no identifiable antenatal risk factor. This is the scientific rationale for offering Active Management of the Third Stage of Labour (AMTSL) routinely to all women.
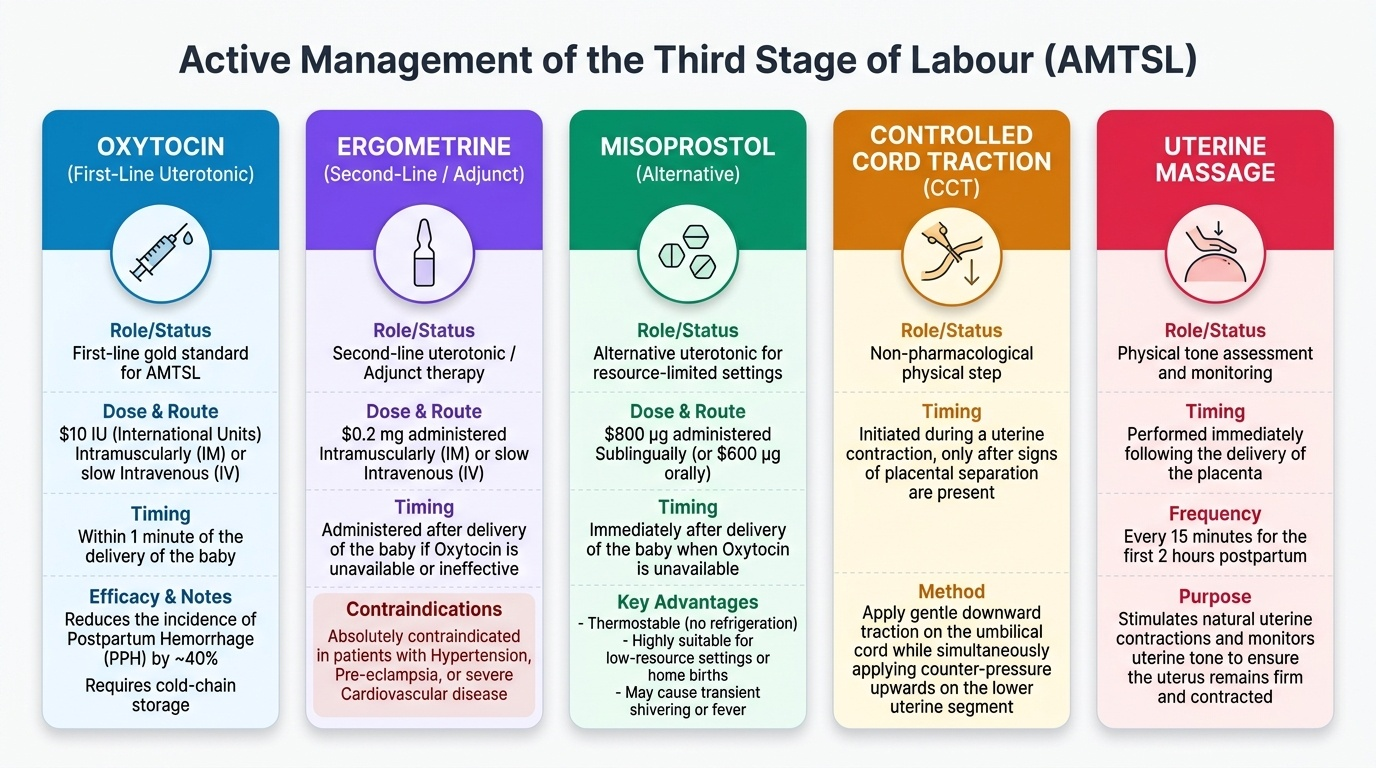
The three components of AMTSL are:
1. Uterotonic administration — oxytocin 10 IU IM (or slow IV if IV access is in place) within 1 minute of delivery of the anterior shoulder or immediately after delivery of the baby; this is the most important step and reduces PPH incidence by approximately 40% compared with expectant management
2. Controlled cord traction — gentle, sustained traction on the umbilical cord (Brandt-Andrews technique) with counter-pressure above the symphysis pubis to prevent uterine inversion, once the uterus has contracted
3. Uterine massage — sustained uterine massage after placental expulsion (no longer universally recommended after placental delivery, but bimanual massage is indicated when the uterus remains atonic)
Provided image
| Risk Category | Examples |
|---|---|
| Grand multiparity | ≥5 previous deliveries |
| Uterine overdistension | Multiple pregnancy, polyhydramnios, macrosomia (>4 kg) |
| Placental problems | Praevia, abruption, accreta spectrum, prolonged 3rd stage |
| Previous uterine surgery | Caesarean scar, myomectomy |
| Coagulation | Known coagulopathy, antiphospholipid syndrome, ITP |
| Labour factors | Prolonged labour, instrumental delivery, general anaesthesia |
| Anaemia | Hb <8 g/dL at onset of labour |