Page 2 of 17
OG16.1 | Post-Partum Haemorrhage — SDL Guide (Part 2)
Diagnosis and Initial Assessment
When PPH is suspected, clinical assessment and initial management must proceed simultaneously — do not pause treatment to await laboratory results. The primary clinical assessment involves three parallel actions: quantify the haemorrhage, assess haemodynamic status, and identify the cause.
Quantification of blood loss in practice relies on visual estimation combined with direct weighing of swabs and collection bags. Visual estimation alone underestimates true loss by 30–50%, particularly in dark rooms or when blood soaks into clothing and theatre drapes. The drape collection bag (a calibrated plastic drape applied under the perineum) is the most accurate method for vaginal deliveries and is now standard in many units. Sequential measurements of fundal height and uterine tone (soft vs firm) help identify atony.
Haemodynamic assessment uses standard vital signs supplemented by the shock index (heart rate ÷ systolic BP). A shock index >0.9 signals significant haemodynamic compromise; >1.7 indicates life-threatening haemorrhage requiring immediate blood transfusion even before laboratory confirmation of anaemia. In young women, tachycardia is often the first sign; hypotension is a late and ominous sign indicating >30% blood volume loss. Monitor urine output (target ≥30 mL/h) as a surrogate for end-organ perfusion.
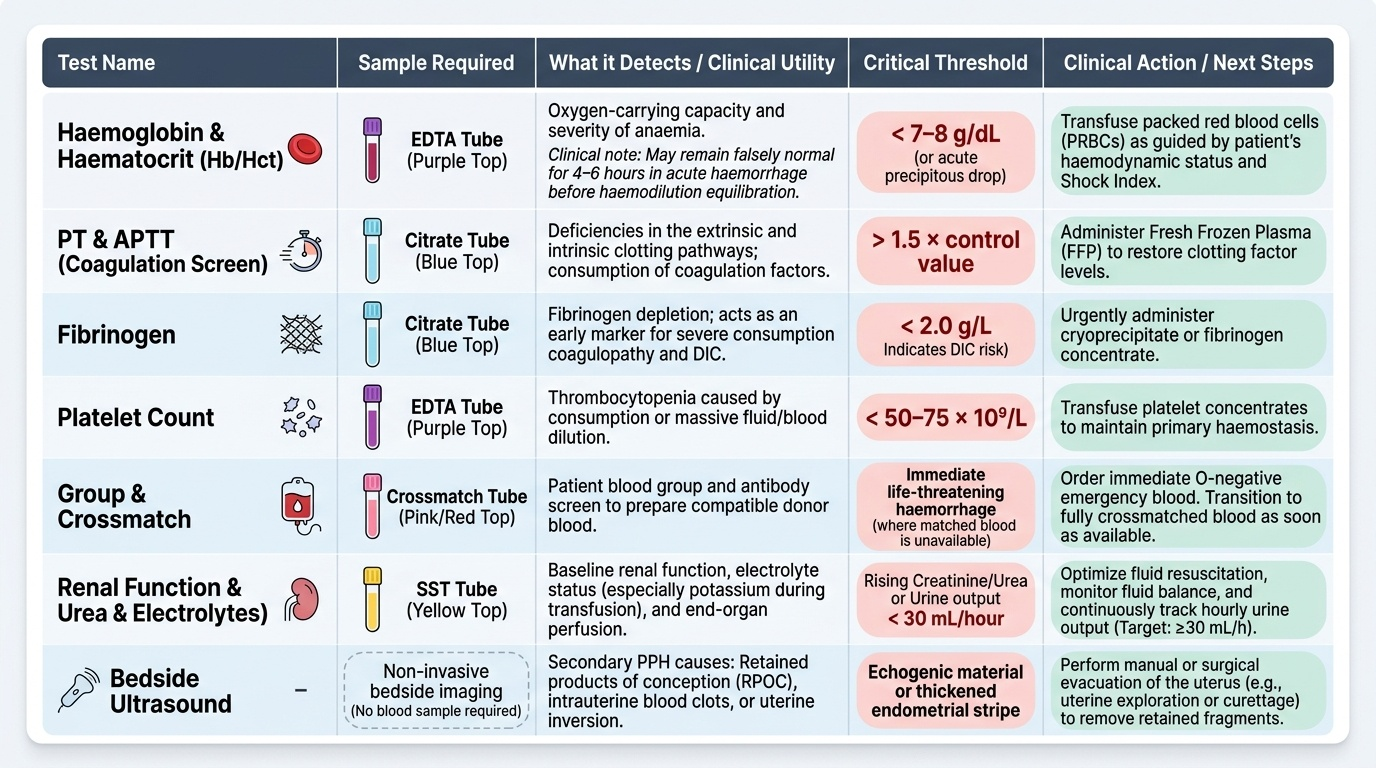
Investigations to arrange urgently:
- Full blood count — haemoglobin, haematocrit (note: in acute haemorrhage, Hb may be falsely normal for 4–6 hours before haemodilution equilibrates)
- Coagulation screen — PT, APTT, fibrinogen (fibrinogen <2 g/L = DIC, needs cryoprecipitate); d-dimers
- Group and crossmatch — type and screen urgently; order O-negative blood if crossmatch is not yet available and transfusion is life-saving
- Serum urea, electrolytes, and renal function
- Ultrasound — if retained products of conception are suspected (secondary PPH), bedside ultrasound identifies echogenic material in the uterine cavity
The clinical examination to identify the cause proceeds in parallel: inspect the lower genital tract systematically under good lighting for cervical and vaginal lacerations; palpate the uterus to assess tone; review the delivered placenta and membranes for completeness (a missing cotyledon or torn membrane edge suggests retained fragments); send blood for clotting studies if DIC is suspected.
Provided image
SELF-CHECK
A 32-year-old G4P3 woman delivered vaginally 15 minutes ago. The uterus is soft and non-contracting. Estimated blood loss is 700 mL and her heart rate is 115/min, BP 100/70 mmHg. What is the shock index and what does it indicate?
A. Shock index = 0.87 — mild compromise, observe and give oral fluids
B. Shock index = 1.15 — haemodynamic compromise, requires immediate IV access, oxytocin and IV fluids
C. Shock index = 0.64 — within normal limits, no immediate intervention needed
D. Shock index = 1.15 — severe haemorrhage, immediate transfusion of O-negative blood is mandatory without further assessment
Reveal Answer
Answer: B. Shock index = 1.15 — haemodynamic compromise, requires immediate IV access, oxytocin and IV fluids
Shock index = HR ÷ SBP = 115 ÷ 100 = 1.15. A value >1.0 reliably identifies haemodynamic compromise requiring immediate intervention: IV access, uterotonic (oxytocin), IV crystalloid resuscitation, and close monitoring. O-negative blood transfusion is recommended when the shock index exceeds 1.7 or when haemodynamic instability persists; at 1.15 with a responding patient, transfusion is prepared (group and crossmatch) but may not yet be mandatory. Option A incorrectly calculates the index, and option C is wrong. Option D overstates the immediate transfusion threshold — 1.15 requires urgent action but 1.7+ is the threshold for immediate unmatched blood.
Medical Management — Uterotonic Therapy
The cornerstone of PPH treatment — particularly for uterine atony — is prompt, stepwise uterotonic therapy. The principle is to achieve sustained, coordinated myometrial contraction to compress the open placental bed vessels. The agents are used in a defined escalating sequence, each with specific doses, routes, and critically important contraindications.
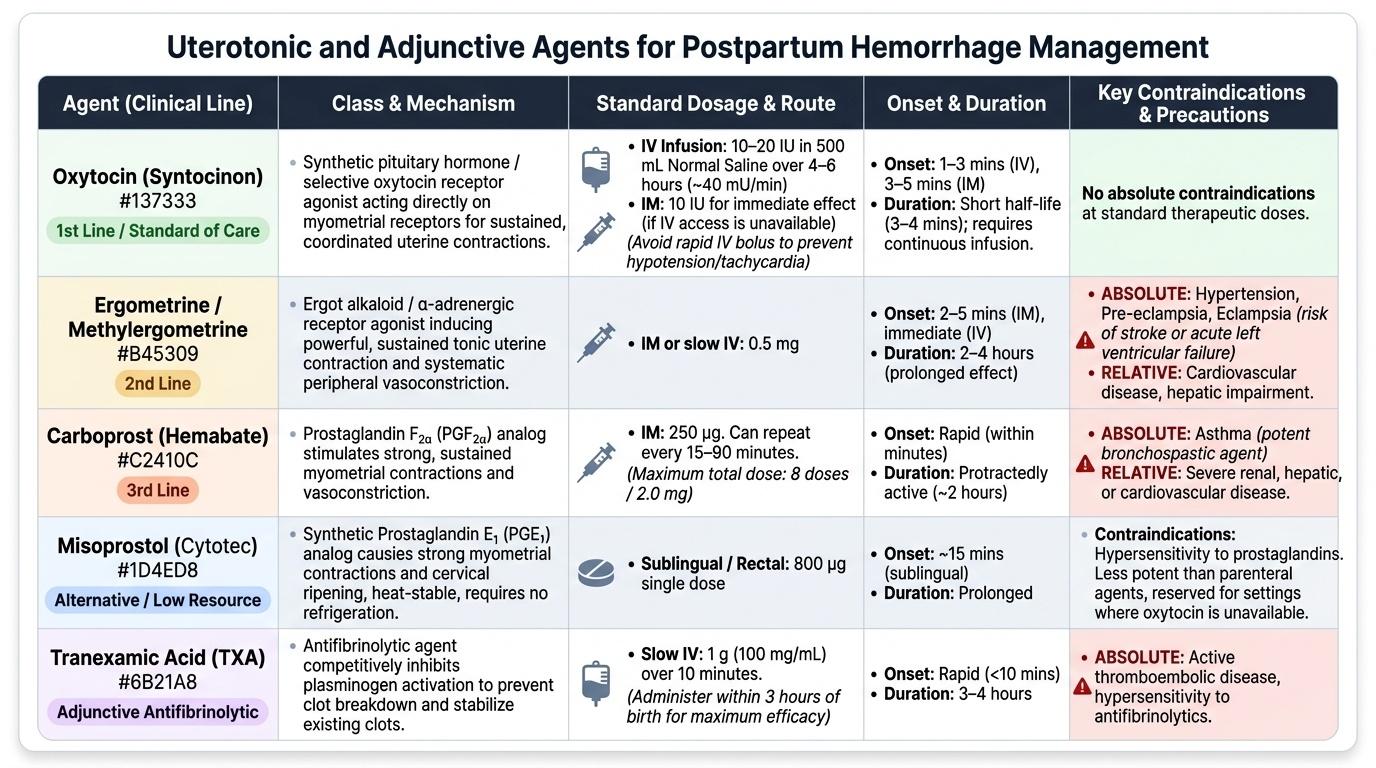
First line: Oxytocin (Syntocinon)
Oxytocin is the uterotonic of choice for both prevention (AMTSL) and treatment of PPH. For treatment: 10–20 IU in 500 mL normal saline IV infusion over 4–6 hours (approximately 40 mU/min), or 10 IU IM for immediate effect. It acts within 1–3 minutes of IV administration. Oxytocin has a short half-life of 3–4 minutes and must be given as a sustained infusion. It has cardiovascular effects at high doses — hypotension and tachycardia — therefore the large bolus dose (10 IU rapid IV push) is avoided; a diluted infusion or slow IV bolus is preferred. Oxytocin has no absolute contraindications at standard doses.
Second line: Ergometrine (ergonovine) / Methylergometrine (Methergine)
Ergometrine 0.5 mg IM or slow IV produces sustained tonic uterine contraction within 2–5 minutes, with a prolonged effect of 2–4 hours. It is an α-adrenergic agonist causing systemic vasoconstriction, which raises blood pressure. Therefore, ergometrine and methylergometrine are absolutely contraindicated in hypertension and pre-eclampsia/eclampsia — administration in such patients risks stroke, hypertensive crisis, or acute left ventricular failure. Also contraindicated in cardiovascular disease and hepatic impairment.
Third line: Carboprost (15-methyl PGF₂α, Hemabate)
Carboprost 250 µg IM can be repeated every 15–90 minutes to a maximum of 8 doses (2 mg total). It produces powerful, sustained uterine contraction. Carboprost is absolutely contraindicated in asthma because PGF₂α causes potent bronchospasm; it is also relatively contraindicated in severe hepatic, renal, and cardiovascular disease. Side effects include diarrhoea, vomiting, flushing, and hypertension.
Alternative: Misoprostol
Misoprostol 800 µg sublingually or rectally is the recommended alternative in settings where parenteral oxytocin is unavailable (home deliveries, remote facilities). It requires no refrigeration, has a longer shelf life, and is orally active. It is less potent than parenteral oxytocin but has been shown in the FIGO/WHO guidance to reduce PPH mortality in resource-limited settings. Side effects include pyrexia and shivering.
Adjunct: Tranexamic acid (TXA)
Tranexamic acid 1 g IV infused over 10 minutes, followed by a second 1 g if bleeding continues after 30 minutes, should be given within 3 hours of PPH onset. It acts as an antifibrinolytic — it inhibits the activation of plasminogen to plasmin, thereby preventing fibrin clot dissolution. The WOMAN trial (2017, >20,000 women across 21 countries) demonstrated that TXA given within 3 hours of PPH onset reduced all-cause mortality from PPH without increasing thromboembolic events. It does NOT treat atony — it is an adjunct, not a replacement for uterotonics.
Provided image
SELF-CHECK
A woman has PPH due to uterine atony following an emergency caesarean section performed for severe pre-eclampsia. She has received oxytocin infusion but the uterus remains atonic. Which uterotonic should be given NEXT?
A. Ergometrine 0.5 mg IM — it is the most potent second-line uterotonic
B. Carboprost 250 µg IM — it is the appropriate second-line agent
C. Ergometrine 0.5 mg IV for rapid effect given the emergency
D. Misoprostol 800 µg sublingual — first check whether parenteral agents are available
Reveal Answer
Answer: B. Carboprost 250 µg IM — it is the appropriate second-line agent
Ergometrine is absolutely contraindicated in pre-eclampsia and hypertension because it raises blood pressure through vasoconstriction, risking stroke or hypertensive crisis. The correct second-line agent after oxytocin failure is carboprost 250 µg IM — provided the patient does not have asthma (carboprost is contraindicated in asthma). Misoprostol is an alternative but is generally reserved for settings without access to parenteral therapy. Options A and C are both wrong because they select ergometrine, which is absolutely contraindicated in this patient.
Surgical and Interventional Management
When uterotonic therapy fails to control haemorrhage — or when the cause is anatomical (genital tract trauma, retained placenta) — surgical management is escalated in a stepwise fashion, always with the goal of preserving the uterus where possible. Each step represents an increase in invasiveness, and the decision to proceed is driven by the haemodynamic response to each intervention.
Bimanual uterine compression is the first mechanical intervention for atony: one hand is inserted vaginally into the vaginal fornix and the other presses the uterine fundus externally, compressing the uterus between both hands. This mechanically tamponades the placental bed and provides time for uterotonics to take effect. It can be maintained for 20–30 minutes.
Uterine packing and intrauterine balloon tamponade are the next step when bimanual compression does not achieve haemostasis. The Bakri balloon (designed for obstetric use) or improvised Condom catheter (an effective and low-cost alternative validated in resource-limited settings) is inserted into the uterine cavity and inflated with 300–500 mL of warm normal saline. The balloon exerts hydrostatic pressure on the myometrium, mechanically compressing the placental bed vessels. A 'tamponade test' is considered positive (surgical intervention unlikely needed) if bleeding stops after balloon inflation.
B-Lynch compression suture is a brace suture technique applied when the uterus is exteriorised at caesarean section and bimanual compression temporarily controls bleeding, but the uterus relaxes immediately on release. A no. 2 Vicryl suture is looped over the uterine fundus and tied below the level of the lower segment on both sides, compressing the uterus and obliterating the cavity. Success rates of 60–80% are reported in series; it is particularly useful as an adjunct after caesarean-related atony.
Stepwise uterine devascularisation reduces uterine perfusion by progressively ligating the uterine arteries (bilateral), followed by the utero-ovarian ligaments. This reduces pulse pressure to the uterus and, combined with uterotonics, allows haemostasis in 75–80% of cases. Internal iliac (hypogastric) artery ligation reduces pulse pressure to the pelvis by approximately 85% and is a highly effective salvage procedure, though technically demanding.
Non-pneumatic anti-shock garment (NASG) is a compression garment applied from the lower limbs and abdomen upward to redistribute blood centrally from peripheral vascular beds. It can reduce blood loss by 40–50% and is particularly valuable as a bridge to surgical intervention or during transfer from a lower to a higher facility.
Obstetric hysterectomy (subtotal or total, depending on the site of bleeding) is the definitive last resort when all other measures fail. Life takes precedence over uterine preservation. It is the most common indication for peripartum hysterectomy and must be performed without hesitation when haemorrhage is life-threatening.
Interventional radiology — uterine artery embolisation (UAE) or internal iliac artery embolisation — is an option in haemodynamically stable patients in centres with 24-hour IR availability. It preserves fertility and is particularly useful in placenta accreta spectrum.
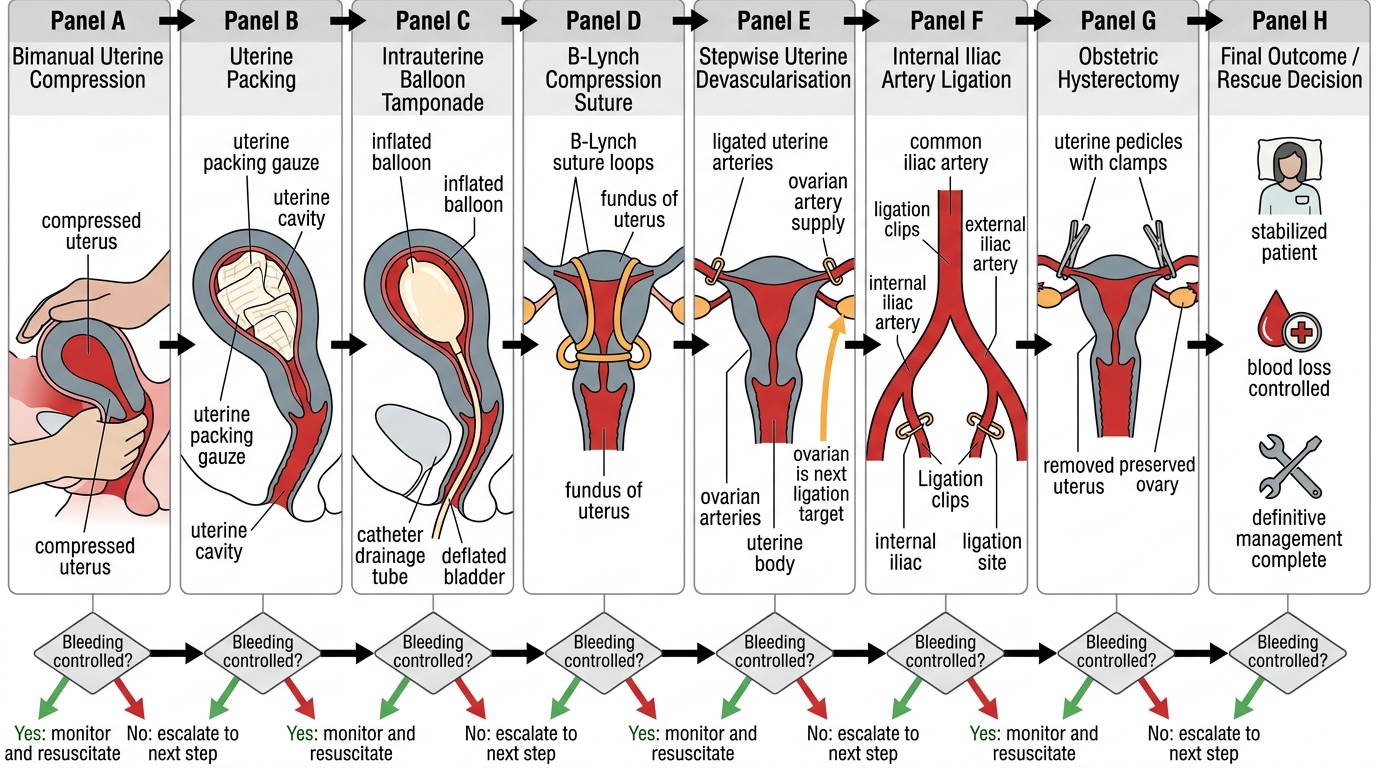
Surgical Escalation Ladder for Refractory PPH