Page 5 of 17
OG16.2 | PPH Emergency Techniques — SDL Guide
Learning Objectives
- Describe the rationale and indications for mechanical and physical techniques in PPH management
- Demonstrate the correct technique for bimanual uterine compression and aortic compression
- Describe the steps for intrauterine balloon tamponade using a Bakri balloon or condom catheter
- Explain how to apply the Non-Pneumatic Anti-Shock Garment (NASG) and its physiological rationale
- Interpret the response to each technique and identify the decision point for surgical escalation
INSTRUCTIONS
Knowing which uterotonic to give is essential — but in many PPH emergencies, mechanical and physical techniques are what stop the bleeding while the drugs take effect, or bridge a patient to surgical intervention. This skills-focused module teaches you the hands-on techniques for PPH control: bimanual and aortic compression, intrauterine balloon tamponade, and the NASG. These are the techniques specifically named in NMC competency OG16.2 and assessed in skill laboratories and OSCEs. Each technique is grounded in anatomy and physiology so you understand not just how to perform it but why it works.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Ch. 22 (Management of PPH) (textbook)
- Williams Obstetrics, 26th edition, Ch. 41 (textbook)
- WHO Technical Brief: Use of Uterine Balloon Tamponade for the Management of PPH, 2012 (guideline)
- FOGSI: NASG Guidelines for Resource-Limited Settings, 2018 (guideline)
- Hofmeyr GJ et al. Condom catheter uterine balloon tamponade for PPH — Cochrane Review, 2015 (journal)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the only doctor at a rural secondary-care centre at midnight. A 26-year-old woman, G2P1, has just delivered her second baby vaginally. Forty-five minutes later the uterus is still soft and you have given two doses of oxytocin plus ergometrine — the bleeding has slowed but not stopped. Blood pressure is falling, heart rate is 124. You have no blood bank and the referral hospital is 90 minutes away. What can you do with your hands, a catheter, and a rubber condom to save this woman's life before the ambulance arrives? This module answers that question. The mechanical and physical techniques you learn here are the difference between a preventable death and a patient who arrives at the tertiary centre alive and haemodynamically stable.
WHY THIS MATTERS
Mechanical techniques for PPH control are not textbook curiosities — they are essential frontline skills that every obstetrician and general medical officer must master. In settings without blood banks, 24-hour surgical facilities, or interventional radiology, these techniques can sustain circulation and control haemorrhage for long enough to transfer the patient or allow uterotonics to act. The condom catheter tamponade — a technique assembled from a Foley catheter, a rubber condom, and a syringe — has been validated in randomised controlled trials across Bangladesh, India, and sub-Saharan Africa to be as effective as the commercially-available Bakri balloon. The NASG has been shown to reduce blood loss by 40–50% and reduce mortality in resource-limited settings. These are not just developing-world techniques: balloon tamponade is recommended in WHO, FIGO, and RCOG guidelines as second-line therapy for atonic PPH worldwide. Bimanual compression is a skill tested in every MBBS OSCE. You must know these.
RECALL
Before we begin the techniques, ground yourself in the underlying anatomy and physiology. Recall that uterine atony — the most common cause of PPH — results from failure of the myometrium to contract and compress the spiral arteries at the placental bed ('living ligatures'). The uterus at term receives approximately 600–800 mL of blood per minute via the uterine arteries (branches of the internal iliac arteries) and to a lesser extent the ovarian arteries (direct branches of the abdominal aorta). This dual supply means that reducing flow in the uterine arteries alone is only partially effective; techniques that act on the aorta or compress the entire uterine body address both supplies simultaneously. Recall also that the abdominal aorta bifurcates into the two common iliac arteries at the level of L4, which corresponds approximately to the level of the umbilicus in most adults — a landmark you will use for aortic compression. Finally, recall the principles of haemostasis: mechanical pressure applied to bleeding vessels reduces transmural pressure, promotes platelet aggregation, and supports clot formation.
Clinical Indication and Rationale
Mechanical and physical techniques for PPH control are second-line interventions employed when uterotonic therapy alone is insufficient to achieve haemostasis, or as immediate life-sustaining measures while definitive treatment (surgery, blood products, transfer) is being arranged. They do not replace uterotonics — they are applied concurrently or when uterotonics have been maximised without adequate response.
The clinical indication for moving from medical to mechanical management is typically one or more of the following: (a) continued significant haemorrhage (blood loss >500 mL ongoing) despite first- and second-line uterotonics, (b) deteriorating haemodynamic status (shock index >1.0, falling BP, rising pulse), (c) uterus that does not respond to bimanual massage, or (d) need to bridge to transfer or surgical intervention. The decision to escalate should be made decisively — delayed escalation from uterotonic-only therapy is a common avoidable cause of PPH mortality.
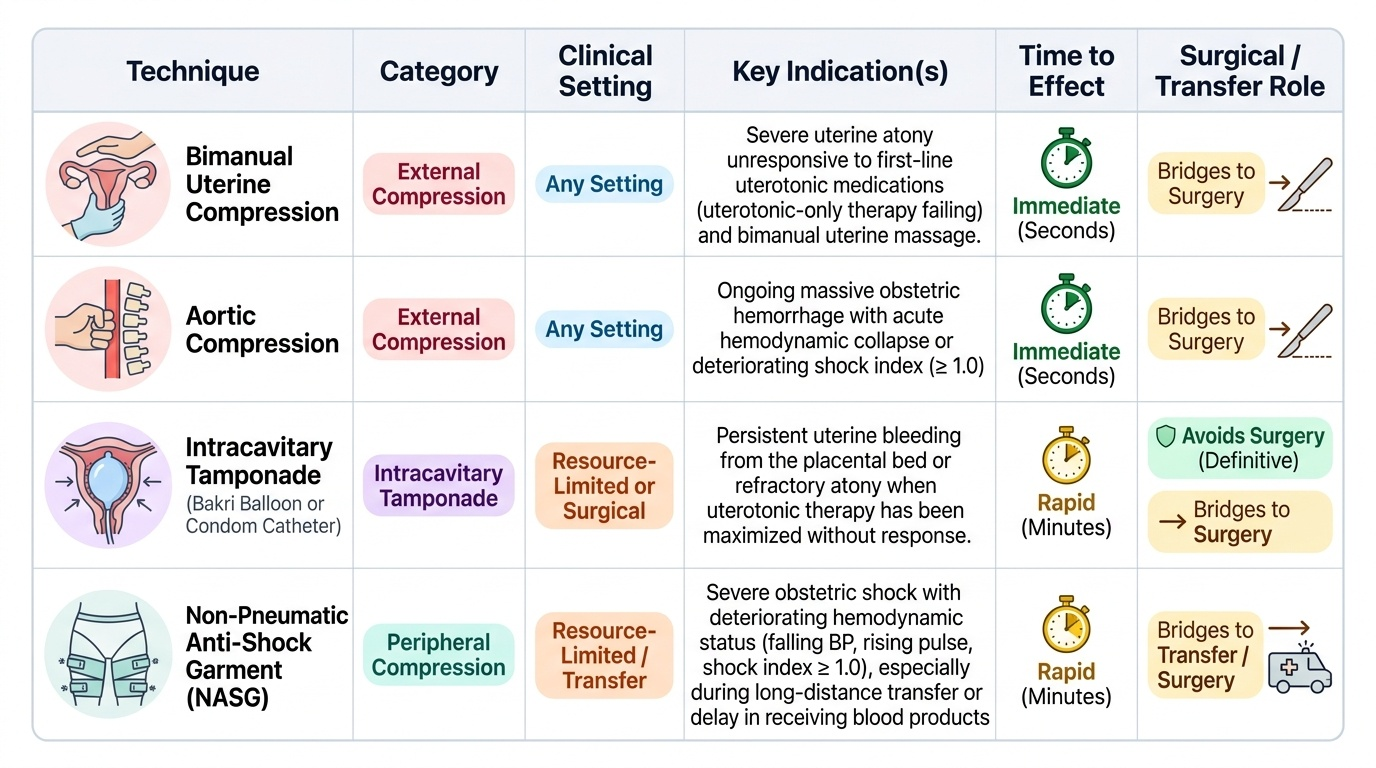
The three principal categories of technique covered in this module are:
- External mechanical compression: bimanual uterine compression (internal + external) and aortic compression — both use the clinician's hands to physically reduce blood flow to the uterus
- Intracavitary tamponade: intrauterine balloon (Bakri balloon or condom catheter) — hydrostatic pressure from within the uterine cavity compresses the placental bed vessels
- Peripheral compression: Non-Pneumatic Anti-Shock Garment (NASG) — circumferential limb and abdominal compression redistributes blood centrally and reduces pelvic perfusion pressure
Understanding when to use each and how to transition between them is as important as knowing the technique itself. These skills are practiced in simulation before clinical application; your role as a final-year student is to be able to perform each technique correctly under supervision and to recognise when it has achieved its endpoint — or when it has not and further escalation is needed.
Provided image
Anatomy Governing PPH Techniques
Each PPH technique exploits a specific anatomical feature of the uterine vasculature. Understanding the anatomy allows you to perform the technique correctly and to explain its mechanism — essential for both clinical practice and examination.
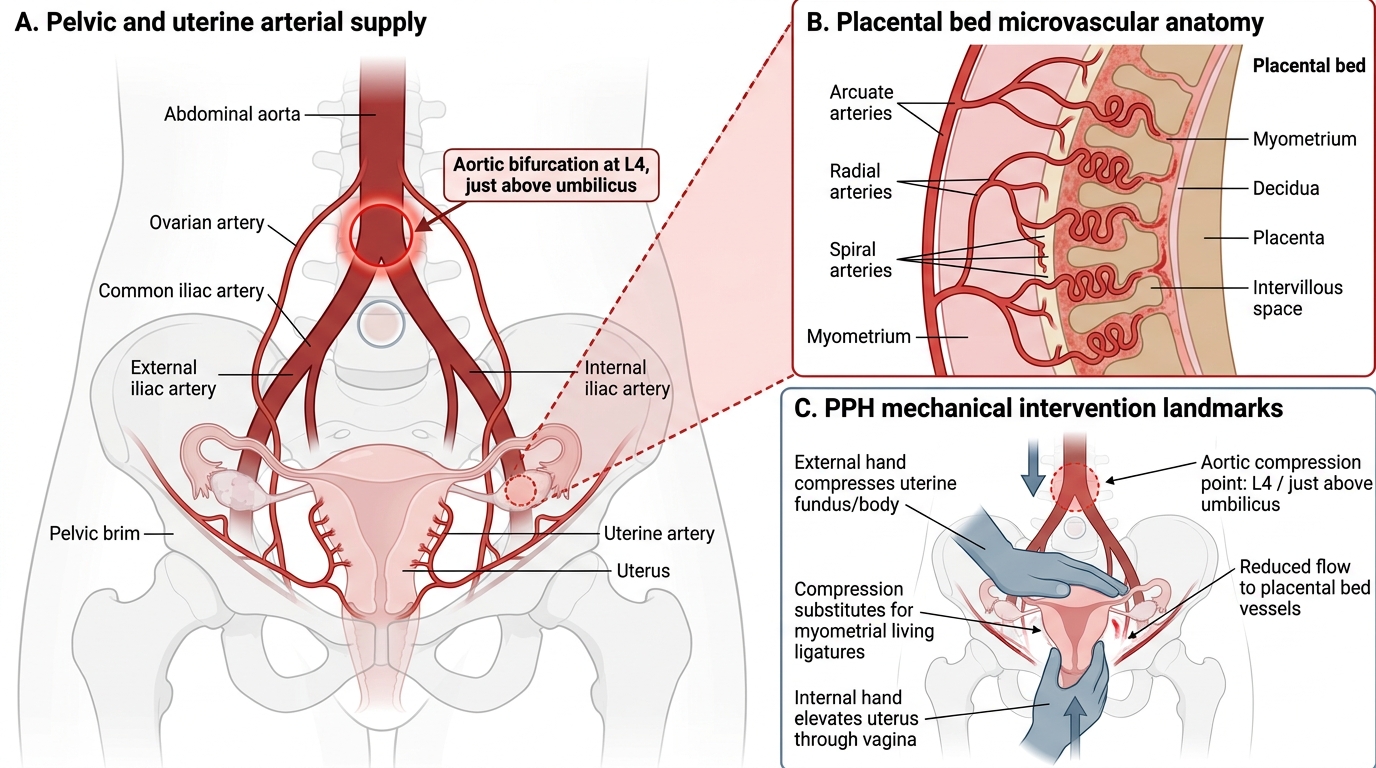
The uterus at term is a heavily vascularised muscular organ with its principal arterial supply from the uterine arteries, which arise from the anterior division of the internal iliac (hypogastric) artery on each side, and ascend lateral to the uterus before branching into the arcuate arteries within the myometrium. The arcuate arteries give rise to radial arteries, which penetrate the myometrium and terminate as spiral arteries at the decidua — the vessels that supply the intervillous space of the placenta. Venous drainage follows the same routes in reverse. The dual blood supply from the ovarian arteries (direct branches of the abdominal aorta, descending in the infundibulopelvic ligaments) accounts for approximately 10–15% of uterine blood flow at term.
The aortic bifurcation into the two common iliac arteries occurs at the L4 vertebral level, which corresponds to a point just below (or at) the umbilicus in the supine pregnant woman. At this level, the aorta lies directly anterior to the vertebral bodies, separated only by the anterior longitudinal ligament. External pressure applied with a closed fist at this point — pressing firmly posteriorly and slightly toward the patient's left to clear the inferior vena cava — can substantially reduce pelvic perfusion pressure. This aortic compression technique is particularly useful as an immediate bridge manoeuvre while a second operator sets up IV access, collects blood, or prepares balloon tamponade equipment.
The uterine cavity at term has a volume of approximately 4–6 litres; however, after delivery the uterus contracts and the cavity volume is much smaller. The lower segment (isthmus) connects the body of the uterus to the cervix and is the insertion point for balloon tamponade devices — the balloon must be placed within the uterine body (above the internal os) to exert effective tamponade on the placental bed, which lies on the anterior or posterior wall of the body.
Uterine Blood Supply and PPH Compression Landmarks
Bimanual Uterine Compression
Bimanual uterine compression is the first and most immediately available mechanical technique for atonic PPH. It requires no equipment — only two hands — and can be initiated within seconds of recognising inadequate uterine contraction. The principle is to compress the uterine body between a vaginally-placed internal hand and an abdominally-placed external hand, mechanically occluding the placental bed vessels and providing a substitute for the myometrial contraction that is failing. The technique exploits the same principle as the 'living ligatures' — direct mechanical compression of the blood vessels within the myometrium — but applies it externally when the myometrium has failed to do so spontaneously. It is always performed with concurrent uterotonic administration, not as a replacement for uterotonics; bimanual compression provides immediate physical haemostasis while the drugs act to restore myometrial tone over the following minutes. The procedure should be sustained for a minimum of 20–30 minutes, with periodic reassessment of uterine tone and haemodynamic status throughout.
Technique — bimanual compression (step by step):
1. Inform the patient and ensure adequate analgesia or regional anaesthesia if available
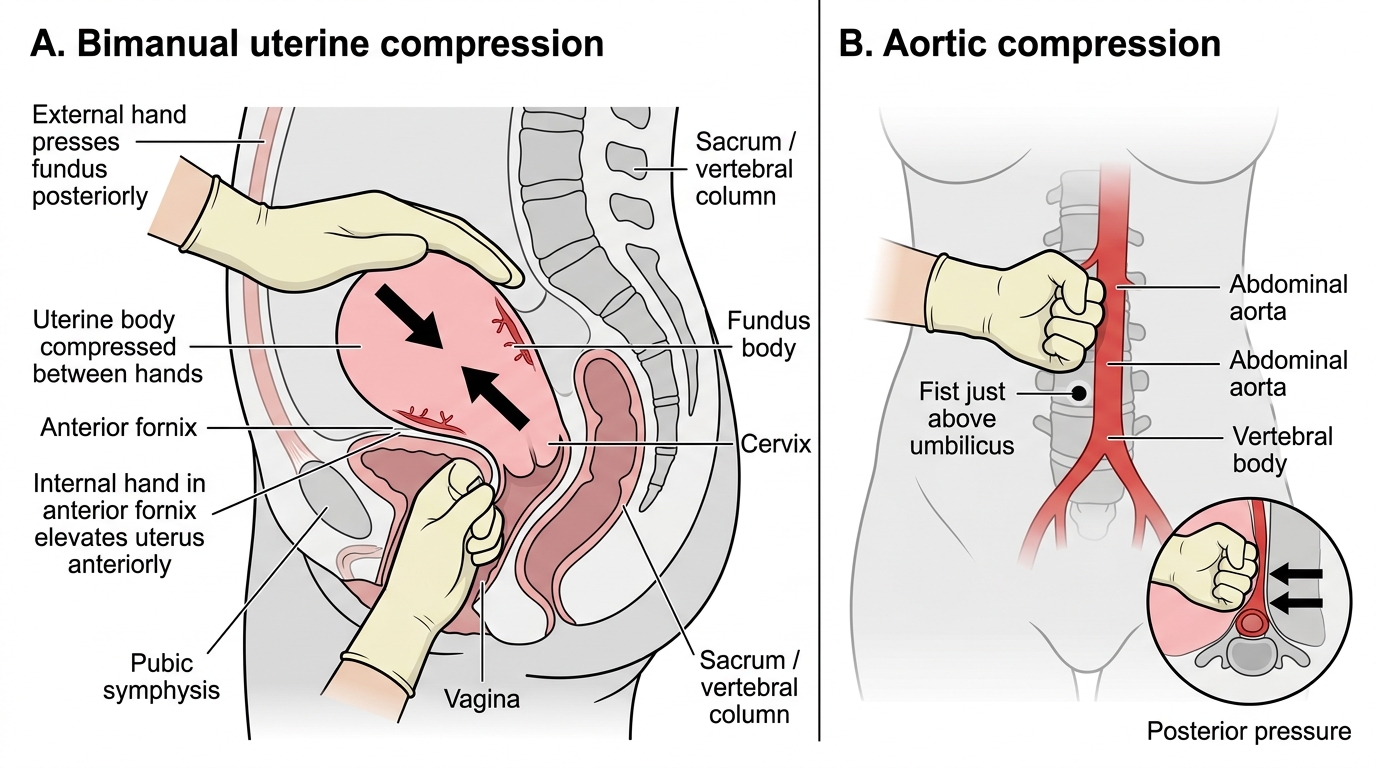
2. The operator stands on the patient's right side; the left (internal) hand is made into a fist and introduced vaginally into the anterior fornix, elevating the uterus anteriorly
3. The right (external) hand cups the uterine fundus through the abdominal wall and presses it posteriorly, compressing the uterine body between the two hands
4. Firm, sustained pressure is applied — the endpoint is reduction or cessation of bleeding from the cervical os
5. Compression is maintained for a minimum of 20–30 minutes while uterotonics are simultaneously administered
6. The uterus is checked every few minutes for evidence of contraction developing; when the uterus contracts firmly on its own, the internal hand is gently withdrawn
Aortic compression technique:
When bleeding is catastrophic and bimanual compression is insufficient or an additional measure is needed, aortic compression can be applied by a second operator simultaneously:
1. Locate the aortic bifurcation at approximately the level of the umbilicus by palpation
2. Make a closed fist and press firmly and posteriorly just above the umbilicus, compressing the aorta against the vertebral column
3. Compression is effective when the femoral pulses are reduced or absent (palpate the femoral artery as a check)
4. Maintain pressure until vascular control is achieved by another method; release gradually rather than abruptly
5. This is a temporary manoeuvre only; sustained aortic compression for more than a few minutes risks ischaemic complications to the lower limbs and viscera
Bimanual Uterine and Aortic Compression Techniques
SELF-CHECK
During bimanual uterine compression for atonic PPH, the external hand should press the uterine fundus in which direction while the internal (vaginal) hand elevates anteriorly?
A. Upward toward the diaphragm — to elongate the uterus and reduce the placental bed surface area
B. Posteriorly (toward the vertebral column) — to compress the uterine body between the two hands
C. Laterally to the left — to occlude the left uterine artery against the pelvic sidewall
D. Inferiorly toward the perineum — to push the placental bed down and improve venous drainage
Reveal Answer
Answer: B. Posteriorly (toward the vertebral column) — to compress the uterine body between the two hands
The mechanics of bimanual compression require the external hand to press the fundus posteriorly while the internal (vaginal) hand is positioned in the anterior fornix elevating the uterus anteriorly. This creates a compressive sandwich around the uterine body, directly occluding the placental bed vessels between the two hands. Pressing upward, laterally, or inferiorly would not achieve the same bilateral compression of the uterine body.