Page 7 of 17
OG16.2 | PPH Emergency Techniques — SDL Guide (Part 3)
Applied Practice and Simulation Scenarios
Competency in PPH emergency techniques is developed through repeated, supervised simulation practice before clinical application. As a final-year student, your learning objective in clinical placements is to observe and assist these procedures under supervision, understand each step and its rationale, and be prepared to perform them correctly in a supervised setting. The following guidance structures your learning in the skill laboratory and on the ward. Simulation-based training for PPH has been shown to reduce the time-to-intervention and reduce procedural errors in clinical emergencies; practising on a mannequin until the sequence is automatic means that the cognitive load during a real emergency is devoted to clinical decision-making rather than recalling procedural steps. The skill laboratory provides a forgiving environment to make and correct errors — the assembly of a condom catheter, the positioning of hands for bimanual compression, and the correct NASG segment sequence should each be practised until performed fluently before you encounter a real PPH. In clinical placements, shift from passive observation to active structured observation: identify each step, mentally annotate the team's decisions, and note any deviation from the standard technique and its outcome.
Common errors to recognise and avoid:
- Bimanual compression: Positioning the internal hand in the posterior (not anterior) fornix, which fails to elevate the uterus anteriorly and reduces compression efficiency; not maintaining adequate sustained pressure (letting up after a few minutes)
- Condom catheter assembly: Insecure condom attachment (leaking at the tie site) causing balloon deflation mid-procedure; inserting the balloon into the cervical canal rather than the uterine body
- NASG: Applying segments in the wrong (proximal-to-distal) order; placing the pelvic ball over the uterine fundus rather than the symphysis pubis; not removing segments gradually (abrupt removal causes rebound hypotension)
- General: Treating mechanical techniques as an alternative to uterotonics rather than a concurrent adjunct; not assessing response at defined time points; delaying escalation decision
Simulation practice objectives:
- On a pelvic mannequin: perform bimanual compression with correct hand positioning (verified by palpation of 'uterine body' between hands)
- Assemble a condom catheter tamponade device from supplied components; insert through a cervical model; inflate to 350 mL while observing for leaks
- Apply NASG to a mannequin in the correct distal-to-proximal sequence, placing the pelvic ball correctly over the symphysis
- Verbally narrate a tamponade test result and the escalation decision
| Technique | Indication | Key Step | Endpoint | Escalate When |
|---|---|---|---|---|
| Bimanual compression | Atonic uterus, first-line mechanical | Internal hand in anterior fornix, external on fundus | Uterus firms, bleeding stops | Not firm after 30 min + uterotonics |
| Aortic compression | Catastrophic haemorrhage bridge | Fist at umbilicus level, press posteriorly | Femoral pulse reduced | As soon as another method available |
| Balloon tamponade | Persistent atony after uterotonics | Insert balloon into uterine body; inflate 300–500 mL | Positive tamponade test | Negative tamponade test → surgery |
| NASG | Haemodynamic shock, bridge to transfer/surgery | Distal → proximal segment application | HR↓, BP↑, consciousness improved | Not responding in 20 min → add transfusion |
In clinical placements, you will primarily observe these procedures being performed by senior staff. Focus on understanding the sequence of events: when the decision to use each technique was made, which finding prompted escalation, and how the team communicated during the procedure. These observations will consolidate your simulation learning.
SELF-CHECK
After inserting an intrauterine condom catheter balloon and inflating it with 350 mL of warm saline, you observe continued significant bleeding through the drainage tube after 20 minutes. How do you interpret this and what is the next step?
A. Positive tamponade test — the bleeding is from the cervix rather than the uterus; apply vaginal packing and wait another 30 minutes
B. Negative tamponade test — balloon tamponade has not achieved haemostasis; proceed to surgical intervention without further delay
C. Indeterminate — inflate the balloon further to 700 mL to increase the hydrostatic pressure before declaring failure
D. The balloon is incorrectly placed — withdraw it and re-insert before making any escalation decision
Reveal Answer
Answer: B. Negative tamponade test — balloon tamponade has not achieved haemostasis; proceed to surgical intervention without further delay
Continued significant bleeding through the drainage port after 20 minutes of adequate balloon inflation constitutes a negative tamponade test — the balloon is not achieving haemostasis. The correct response is to escalate immediately to surgical management (B-Lynch suture, uterine devascularisation, or obstetric hysterectomy). Over-inflating the balloon beyond the recommended 500 mL risks uterine perforation and does not constitute an additional therapeutic option. While incorrect placement is a possibility if the balloon was not properly inserted, the clinical response (continued bleeding through the drainage port, which confirms intra-cavitary placement) indicates a genuine failure of tamponade, not a placement error.
Self-Assessment
Apply the procedural and decision-making knowledge from this module to test your readiness for clinical placements and OSCE skill stations. Work through each scenario systematically before reading the answer, as you would in an actual examination or clinical situation. The three scenarios below each isolate a different skill: correct hand positioning for bimanual compression, interpretation of the tamponade test, and the NASG application sequence. These are precisely the skill checkpoints assessed in the NMC MBBS practical examination and in OSCE circuits at most medical colleges. A confident, correct answer to all three is your minimum benchmark before proceeding to the clinical ward. If any answer surprises you, return to the relevant section — particularly the step-by-step technique descriptions — before your next skill laboratory session.
Scenario 1: A 24-year-old primigravida delivers at term. The uterus remains atonic despite oxytocin 20 IU IV infusion and ergometrine 0.5 mg IM. Blood loss is approximately 900 mL, heart rate 108/min, BP 100/68 mmHg.
- Question: What mechanical technique should be initiated first, and describe the correct technique step for positioning the internal hand.
- Answer: Bimanual uterine compression. The internal left hand is made into a fist and introduced vaginally into the anterior fornix (not the posterior), elevating the uterus anteriorly. The right (external) hand presses the fundus posteriorly from the abdominal wall, compressing the uterine body between them.
Scenario 2: The same patient as above — bimanual compression for 25 minutes with ongoing oxytocin has reduced but not stopped bleeding. You decide to insert an intrauterine condom catheter.
- Question: After inserting the device and inflating to 400 mL, you observe no blood from the drainage port and vaginal bleeding has ceased. How do you interpret this?
- Answer: This is a positive tamponade test — haemostasis has been achieved by balloon tamponade. Continue monitoring; leave the balloon in place for 12–24 hours; plan gradual deflation after uterotonic cover and with surgical backup available.
Scenario 3: A woman in PPH haemodynamic shock (BP 80/50, HR 130, confused) is being prepared for transfer. The NASG is available. In what order do you apply the segments?
- Answer: Distal to proximal: legs (ankle to mid-calf) → thighs (knee to upper thigh) → pelvis (with pelvic ball over symphysis pubis) → abdomen (iliac crests to costal margin). This sequence mobilises peripheral blood centrally as each segment is applied.
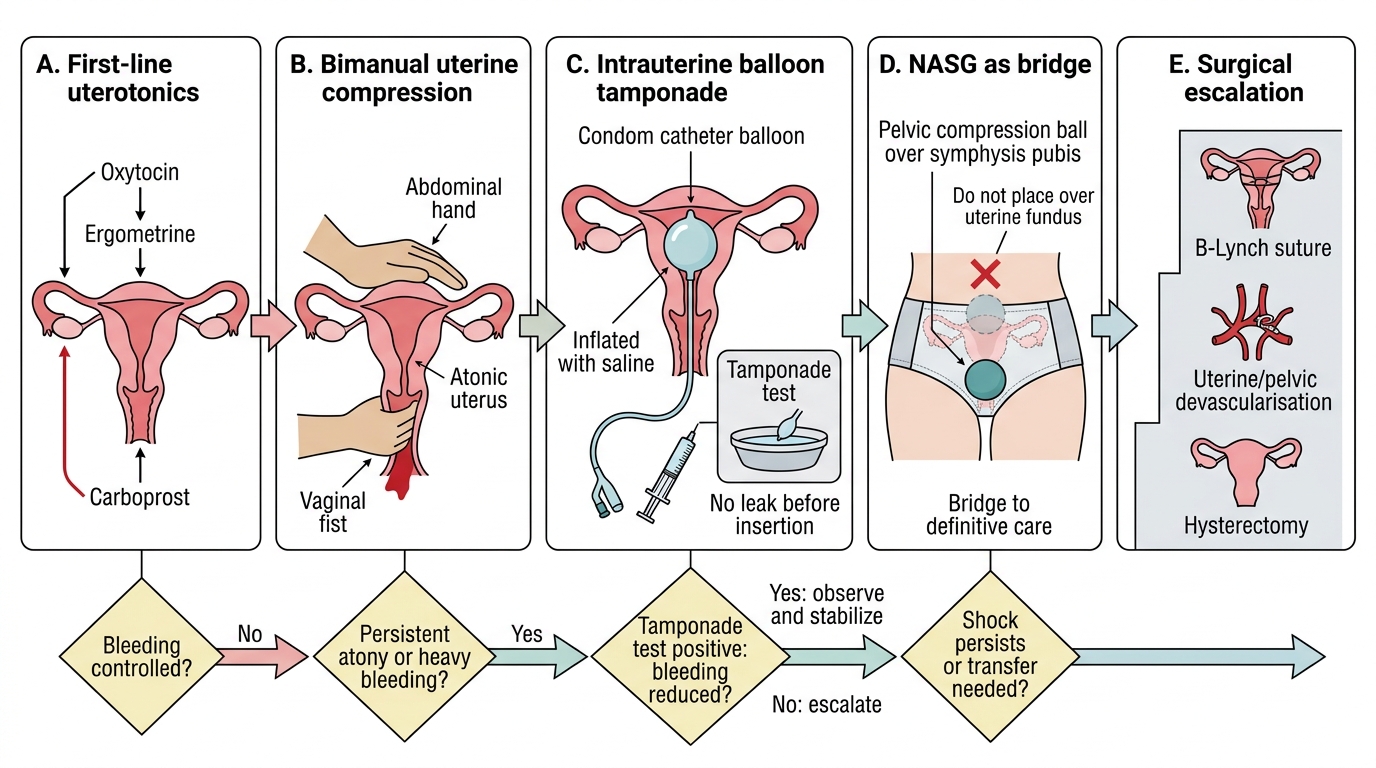
PPH Emergency Escalation Decision Ladder
CLINICAL PEARL
The condom catheter balloon is arguably the most important improvised medical device in obstetric emergency care. Assembling one correctly and inserting it confidently in a woman with uncontrolled PPH can prevent an obstetric hysterectomy. Always test the seal before insertion — inflate the assembled device with saline off the patient and confirm there is no leak before you introduce it vaginally. A critical NASG rule: always place the pelvic compression ball directly over the symphysis pubis, never over the uterine fundus — placing it over the fundus compresses the uterus externally but does not apply the targeted pelvic vascular compression that gives the NASG its haemostatic effect.