Page 3 of 32
OP10.1 | Extraocular Movement Examination: Uniocular and Binocular Technique — SDL Guide (Part 3)
Interpreting Findings: Normal vs Abnormal EOM
Accurate interpretation requires a mental map linking movement limitations to specific muscles and their nerve supply. The key interpretive principle is the field of action rule: each extraocular muscle is best assessed (and shows its deficit most clearly) in its field of primary action. For the superior rectus: up-and-out gaze; for the inferior rectus: down-and-out; for the superior oblique: down-and-in; for the inferior oblique: up-and-in.
Provided image
Distinguishing comitant from incomitant deviation: A comitant (concomitant) deviation is one in which the angle of deviation is equal in all positions of gaze — the deviation does not increase in any particular direction. This is characteristic of childhood strabismus (infantile esotropia, accommodative esotropia) where the deviation is due to an imbalance of binocular control rather than a muscle or nerve problem. The patient typically does not complain of diplopia because suppression develops. An incomitant deviation is one in which the deviation varies with direction of gaze — it is greatest in the field of action of the paretic muscle or in the direction of the restricted movement. This pattern is characteristic of muscle palsy or restriction.
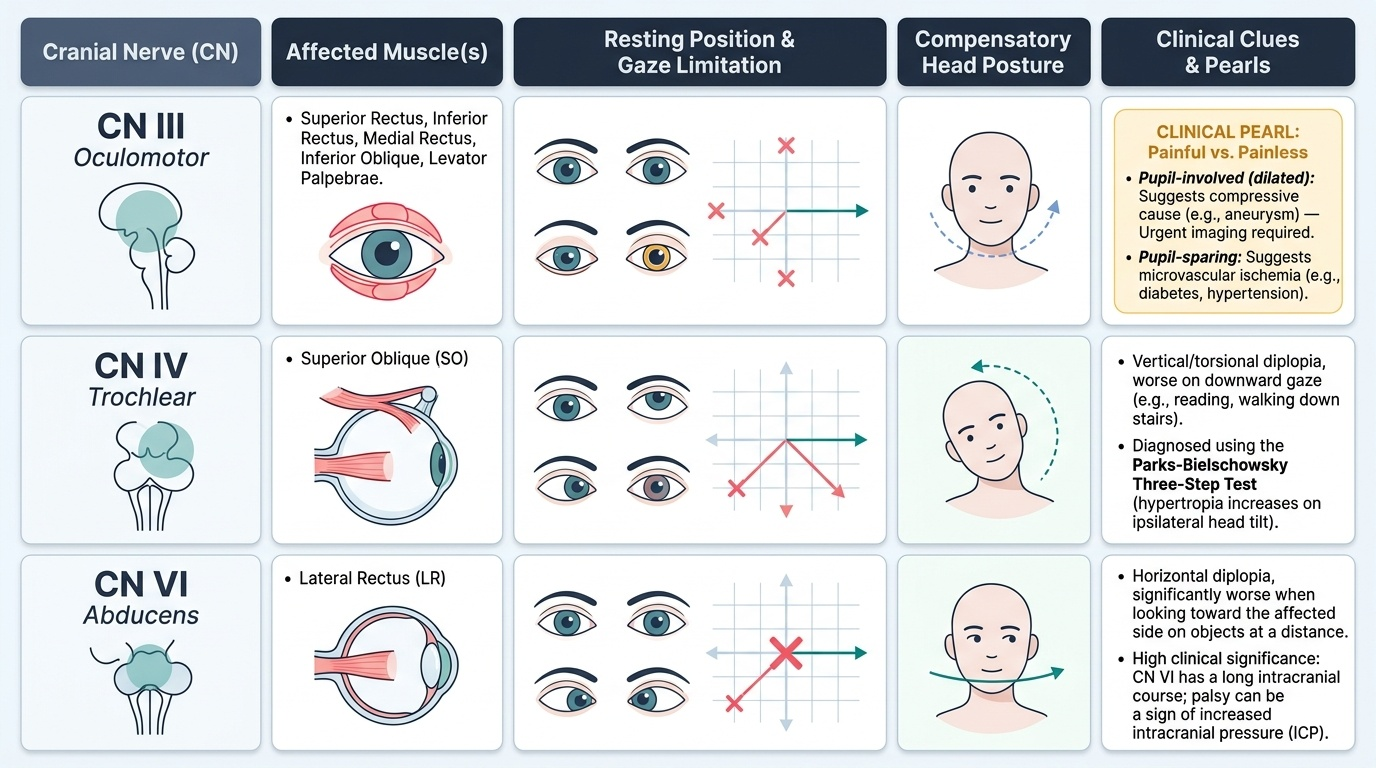
Characteristic patterns by cranial nerve:
- CN VI (Abducens) palsy: Limitation of abduction of the affected eye; esotropia at distance (lateral rectus is the abductor). Horizontal diplopia, worse on gaze towards the affected side. Compensatory face-turn toward the affected side.
- CN IV (Trochlear) palsy: Limitation of depression in adduction (inferior oblique overaction pattern). Hypertropia of the affected eye worse on ipsilateral gaze and contralateral head tilt. The patient develops a contralateral head tilt (Parks-Bielschowsky three-step test identifies CN IV palsy).
- CN III (Oculomotor) palsy: Ptosis, dilated fixed pupil (if complete), eye in "down and out" position (lateral rectus and superior oblique unopposed). Limitation of adduction, elevation, and depression. If pupil-sparing, consider microvascular ischaemia (diabetes, hypertension) rather than compressive cause.
CLINICAL PEARL
The 'painful versus painless' pupil-involved CN III palsy rule: A complete CN III palsy with a DILATED FIXED PUPIL and pain should be treated as a posterior communicating artery (PCoA) aneurysm until proven otherwise — urgent CT-angiography or MR-angiography is mandatory. This is because the pupillomotor fibres run on the OUTER surface of CN III where they are compressed first by an expanding aneurysm. Diabetic microvascular CN III palsy, by contrast, tends to be PUPIL-SPARING (central ischaemia affects the motor fibres first while the peripheral pupillomotor fibres are relatively spared). This rule is not absolute — 10–20% of compressive CN III palsies can be pupil-sparing — but it governs the initial triage decision. Do not be reassured by a pupil-sparing presentation if pain is prominent.
Applied Practice: Common Clinical Scenarios
Applying systematic EOM examination to a clinical case consolidates all the preceding steps. Consider three commonly tested presentations:
Scenario 1 — CN VI palsy (as in the hook case): A diabetic man, 52 years, wakes with horizontal diplopia. Examination: Hirschberg centred bilaterally on the primary position. Versions: the right eye fails to abduct fully; in right gaze, the right eye lags behind. Cover test: esotropia present at distance, worse on right gaze. Ductions (right eye alone): abduction limitation confirmed. Ductions (left eye alone): full movement in all directions. Interpretation: right CN VI palsy, most likely microvascular (age, diabetes). No pupil abnormality, no pain: reassure and monitor, blood sugar control. Refer if not resolving in 3 months or if progressive.
Scenario 2 — CN III palsy: A 65-year-old hypertensive woman presents with right ptosis, diplopia. On elevation of the lid: right eye is deviated down and out, pupil fixed dilated 7 mm, unable to adduct or elevate the right eye. Ductions confirm absence of elevation, adduction, and depression, with abduction preserved. Cover test: large exotropia and hypotropia right eye. Interpretation: complete right CN III palsy. Pupil involvement in a patient of this age: URGENT imaging to exclude PCoA aneurysm despite mild hypertension history.
Scenario 3 — Concomitant esotropia (childhood): A 4-year-old child is brought with a constant inward turn of the right eye for 6 months. Hirschberg: right corneal reflex displaced nasally (temporal reflex ≈ pupil margin = ~15°). Cover/uncover: right eye moves outward (from in to straight) on covering left eye — right esotropia confirmed. Versions: FULL range of movement in all positions, equal deviation in all gazes (comitant). Ductions: full, confirming no paresis. Interpretation: comitant right esotropia — assess for accommodative component (cycloplegic refraction), amblyopia (visual acuity each eye), and refer to strabismologist.
SELF-CHECK
During the cover/uncover test with the patient fixating a distant target, the RIGHT eye is covered. The LEFT eye moves from a lateral (outward) position to take up fixation. What is the diagnosis?
A. Left esotropia (manifest inward deviation of the left eye)
B. Left exotropia (manifest outward deviation of the left eye)
C. Right esophoria (latent inward deviation of the right eye)
D. Right exophoria (latent outward deviation of the right eye)
Reveal Answer
Answer: B. Left exotropia (manifest outward deviation of the left eye)
When the right eye is covered, the LEFT eye moves from a lateral (outward) position to take up fixation — this means the left eye was resting in an outward (exo) position before the cover was applied. This is a MANIFEST exodeviation of the left eye — left exotropia. The movement is from temporal (out) to straight when fusion is disrupted by covering, confirming a pre-existing outward manifest deviation.
Self-Assessment: Testing Your EOM Examination Skills
Before you proceed to your clinical EOM examination posting, take a moment to consolidate the chain of reasoning that links anatomy to technique to interpretation. The extraocular movement examination is not a sequence of isolated tests — each component builds on the last. Ductions establish individual muscle action and detect restriction or paresis in isolation; versions expose yoke imbalances under binocular conditions; the cover test classifies the deviation as manifest or latent and identifies which eye is deviating; the Hirschberg test provides an objective angle estimate independent of patient cooperation; and interpretation of the combined findings leads to localisation of the lesion to a specific muscle and its nerve supply. A student who performs each test correctly but interprets them in isolation will miss the pattern. A CN IV palsy, for example, is identified by: hypertropia of the affected eye on versions (worst in ipsilateral gaze), a positive Parks-Bielschowsky three-step test, limited depression in adduction on ductions, and a compensatory contralateral head tilt on clinical observation — no single test alone delivers the diagnosis. Practice the full sequence until the choreography is automatic.
Checklist self-check:
1. Can you name all six extraocular muscles and their cranial nerve supply without looking?
2. Can you describe the difference between a duction and a version?
3. Can you explain why the cover/uncover test identifies a tropia but the alternate cover test identifies phoria + tropia?
4. Can you estimate angle of strabismus from a Hirschberg test if the reflex is at the pupil margin vs the iris margin?
5. Can you describe the gaze position in which you would look for CN IV palsy?
For an OSCE scenario, the examiner will typically ask you to examine EOM on a model patient or a cooperative volunteer and then present a clinical photograph or vignette. Common vignette formats: a photograph of a child with pseudo-strabismus (angle kappa — large positive angle), a CN VI palsy limitation, and an accommodative esotropia. Practice drawing the characteristic eye diagrams for each CN palsy.
Self-check knowledge questions are provided in the micro-quiz blocks interspersed in this SDL. Review your answers and use any incorrect ones to re-read the relevant section before your clinical posting.
SELF-CHECK
A 3-year-old child is brought for assessment because a family member thinks the child's eyes 'look like they are drifting outward.' The corneal light reflex is located at the temporal margin of the pupil symmetrically in both eyes. The alternate cover test shows NO corrective movement in either eye, and versions are full. What is the most likely explanation?
A. Bilateral exotropia
B. Pseudostrabismus due to positive angle kappa
C. Convergence excess esotropia
D. CN VI bilateral palsy
Reveal Answer
Answer: B. Pseudostrabismus due to positive angle kappa
Positive angle kappa (visual axis nasal to pupillary axis) causes the corneal light reflex to appear displaced TEMPORALLY relative to the pupil centre in a straight eye, giving the appearance of outward deviation — this is pseudo-exotropia. The negative alternate cover test (no corrective movement) confirms the eyes are actually orthophoric. This is a common normal variant in children and does not require treatment. In true exotropia, the alternate cover test would reveal a corrective inward movement of the covered eye on uncovering. Always confirm apparent strabismus with the cover test.