Page 2 of 32
OP10.1 | Extraocular Movement Examination: Uniocular and Binocular Technique — SDL Guide (Part 2)
Binocular Testing — Versions and Vergences
Versions are conjugate binocular movements in which both eyes move in the same direction simultaneously under binocular viewing conditions. Version testing is the natural complement to duction testing: whereas ductions isolate individual muscle action, versions assess the coordinated function of yoke muscle pairs and expose the dynamic interaction between the two eyes during conjugate gaze. The power of version testing lies in the fact that Hering's law demands equal and simultaneous innervation to yoke muscles — so when a yoke pair is mismatched in strength (as occurs with a paretic muscle), one eye will lag while the other leads, a discrepancy that becomes dramatically visible when both eyes are open and moving together. Version testing also reveals overactions: in a long-standing CN VI palsy, the contralateral medial rectus may develop a secondary overaction as it receives supra-normal innervation (by Hering's law) when the paretic lateral rectus requires extra innervation to reach a given gaze position. This overaction pattern is only visible on version testing, not on duction testing of the medial rectus alone. Versions should always be tested in all nine positions of gaze using a smooth, slow-moving target, with the examiner watching both eyes simultaneously and noting which eye leads, lags, or shows a nystagmoid jerk at the extremes of gaze. The standard test is the nine positions of gaze (also called the H-pattern or cardinal positions of gaze test): primary position (straight ahead), right gaze (dextroversion), left gaze (laevoversion), up-right, up-left, down-right, down-left, elevation in primary position, and depression in primary position.
Technique for versions:
1. Both eyes open; no occlusion.
2. Examiner holds the target at 33 cm and moves it through all nine positions, pausing briefly in each position to observe both eyes simultaneously.
3. Note: symmetry of movement; any lag, limitation, or overaction of a single eye in any position; any nystagmus.
4. Compare each muscle's action to its yoke muscle in the fellow eye (e.g. right lateral rectus and left medial rectus are yoke muscles for dextroversion).
Vergences are disconjugate movements — the eyes move in opposite directions to maintain single binocular vision as the target moves in depth. Convergence testing is clinically important: ask the patient to follow a finger brought from 40 cm to 5–7 cm towards the bridge of the nose and note the near point of convergence (NPC). Normal NPC is ≤10 cm from the bridge of the nose; a receded NPC (>10 cm) suggests convergence insufficiency. Divergence is tested by observing the eyes as the target moves away.
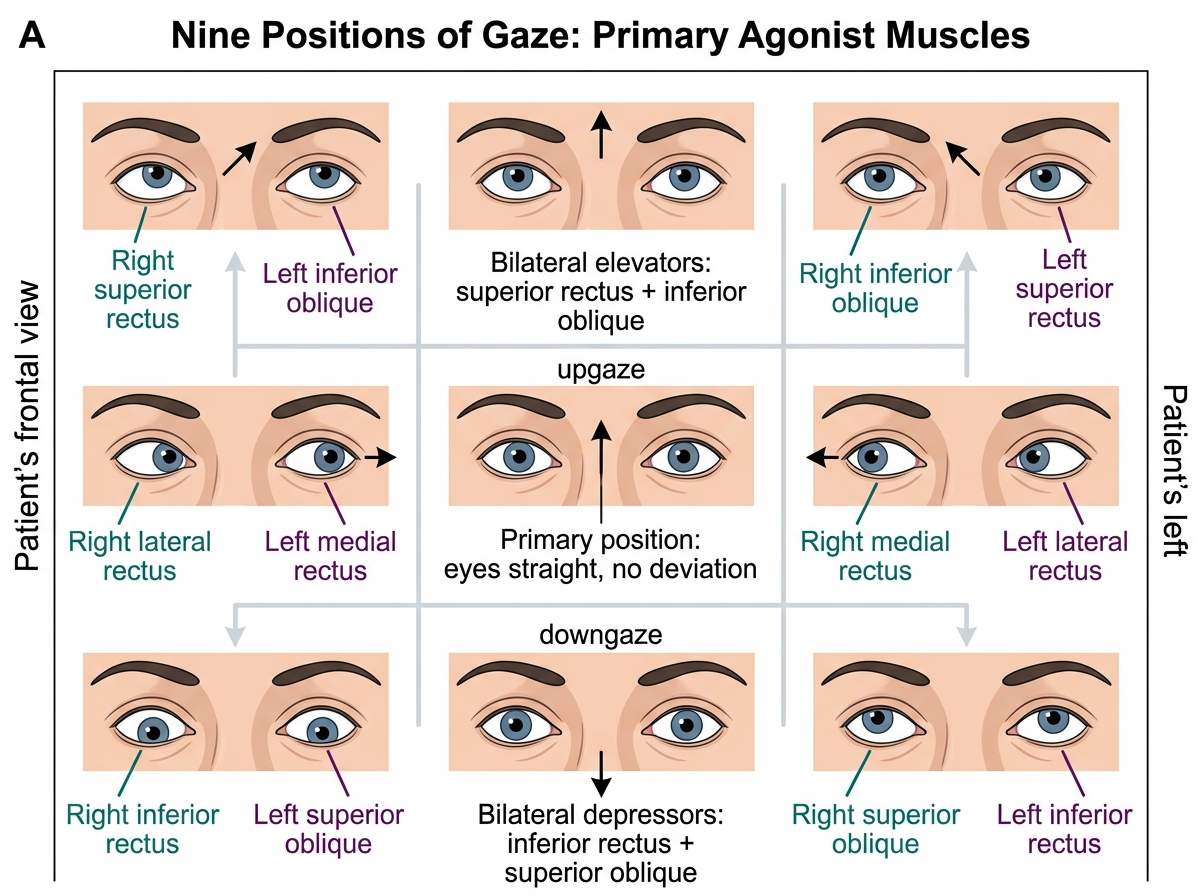
Nine Positions of Gaze and Primary Agonist Muscles
Cover/Uncover and Alternate Cover Tests
The cover tests are the cornerstone of clinical strabismus assessment and the most important part of the EOM examination for any patient suspected of having a deviation. They work by exploiting a fundamental principle: the human visual system uses binocular fusion — the cortical drive to keep both foveas aligned on the same object — to maintain single binocular vision. When you cover one eye you remove the binocular fusion stimulus for that eye, breaking the alignment lock. If a manifest deviation (heterotropia) is present, the uncovered eye moves to take up fixation when the better eye is covered. If only a latent tendency (heterophoria) exists — held in check by the fusion reflex during binocular viewing — the alternating cover test dissociates fusion completely and reveals that tendency as a corrective fixation movement. The cover tests are also the definitive way to distinguish true strabismus from pseudostrabismus: a child with prominent epicanthal folds may appear esotropic, but the cover test will show no corrective movement if the eyes are actually straight. You must understand what you are testing before you pick up the occluder.
Cover/uncover test (CT): Detects a manifest deviation (heterotropia / tropia) — a constant, non-fusional misalignment present even during binocular viewing.
- Ask the patient to fixate on a distant target (6 m) or a near target (33 cm) with both eyes open.
- Cover the RIGHT eye and watch the LEFT eye for a movement. If the left eye moves to take up fixation (a corrective movement), a manifest deviation was present in the left eye. The direction of movement identifies the type: movement inward (from temporal to nasal) = exotropia (the left eye was turned out); movement outward = esotropia.
- Remove the cover from the right eye and watch the right eye: if it moves to regain fixation, it was deviated (manifest deviation of the right eye).
- Repeat covering the left eye and watching the right.
Alternate cover test (ACT): Detects the total deviation (manifest + latent, i.e. heterotropia + heterophoria) by dissociating binocular fusion completely. Cover is moved rapidly from eye to eye (allowing 1–2 seconds under cover) without allowing binocular viewing at any point. When the cover is removed from an eye, watch for the corrective fixation movement. The ACT will reveal a larger deviation than the cover/uncover test if a phoria component exists. The prism alternate cover test (PACT) quantifies the deviation in prism dioptres by neutralising the movement with a prism.
Key distinction: The CT tells you if a tropia is present and which eye is involved. The ACT measures the maximum (total) deviation. Together they classify the deviation as phoria (latent, controlled by fusion) or tropia (manifest, not controlled by fusion).
Recording convention: esophoria/esotropia = "E" or "ET/EP"; exophoria/exotropia = "X" or "XT/XP"; vertical = hyperphoria/hypertropia.
Hirschberg Corneal Reflex and Krimsky Test
The Hirschberg corneal reflex test provides a rapid, objective estimate of the angle of strabismus without requiring patient cooperation, making it indispensable in the examination of infants, toddlers, intellectually disabled patients, or any patient who cannot reliably follow a target for version and duction testing. The test is rooted in basic optics: the cornea acts as a convex mirror and reflects an image of a light source. When the patient's visual axis is aligned with the light source, this corneal light reflex (CLR) falls at a consistent anatomical landmark on the cornea — slightly nasal to the pupil centre in most normal eyes (the nasal offset is due to angle kappa). When the eye is deviated — turned in or out — the visual axis no longer points at the light, and the reflection falls on a different part of the cornea. The direction and distance of this displacement from the pupil centre identifies the direction and magnitude of the deviation. The test therefore converts an angular measurement (angle of strabismus in degrees or prism dioptres) into a spatial measurement (millimetres of reflex displacement from the pupil centre) that can be estimated at the bedside with no equipment other than a pen torch. Because it does not require fusion or fixation by the deviating eye, it is the single most useful test when other strabismus tests are impossible.
Technique:
1. Shine a pen torch from approximately 33 cm, equidistant from both eyes, along the line of sight.
2. Ask the patient (or have the parent hold the infant's head still) to look at the light.
3. Observe the position of the corneal light reflex in each eye simultaneously.
4. In the orthophoric (straight) eye, the reflex sits at or just slightly nasal to the centre of the pupil (pseudo-strabismus allowance for positive angle kappa).
5. Decentration of the reflex indicates deviation: nasal displacement of the reflex = exotropia (eye turned out); temporal displacement = esotropia (eye turned in).
6. Quantification: 1 mm of decentration ≈ 7° (≈ 15 prism dioptres) of deviation (per Khurana). A reflex at the pupil margin ≈ 15° deviation; at the iris margin ≈ 30–45° deviation.
The Krimsky test refines the Hirschberg by placing prisms in front of the fixing eye (base-out for esotropia, base-in for exotropia) until the corneal reflex is centred in the deviated eye, giving a prismatic measure of the deviation.
Angle kappa: The visual axis and the pupillary axis do not perfectly coincide. A positive angle kappa (visual axis nasal to pupillary axis) causes the CLR to appear slightly temporal in a straight eye — mimicking exotropia (pseudo-exotropia). A negative angle kappa mimics esotropia. Awareness of angle kappa prevents over-diagnosis of strabismus on the Hirschberg test alone.
SELF-CHECK
A child's corneal light reflex falls at the temporal margin of the iris in the right eye when tested with Hirschberg's test. The left eye reflex is centred. What is the approximate angle of deviation, and which type of strabismus does this suggest?
A. 15° esotropia
B. 30–45° esotropia
C. 15° exotropia
D. 30–45° exotropia
Reveal Answer
Answer: D. 30–45° exotropia
Temporal displacement of the corneal reflex in the right eye means the right eye is turned inward (toward the nose) relative to the light — this is esotropia. A reflex at the iris margin corresponds to approximately 30–45° of deviation (iris margin ≈ 2–3 mm decentration × 15°/mm). Temporal reflex = esotropia. The answer is 30–45° esotropia.