Page 5 of 32
OP10.2 | Heterotropia and Strabismus — SDL Guide
Learning Objectives
- Classify strabismus by direction, laterality, comitance, onset, and accommodative status
- Distinguish comitant from incomitant strabismus on clinical grounds
- Describe the clinical features of infantile esotropia, accommodative esotropia, and intermittent exotropia
- Explain why untreated childhood strabismus leads to amblyopia and what determines the critical period
- Interpret cover test and Hirschberg findings in the context of strabismus diagnosis
- Enumerate the indications for referral of a patient with strabismus
INSTRUCTIONS
Strabismus — the misalignment of the visual axes — is one of the commonest eye problems seen in paediatric ophthalmology clinics and is an important cause of preventable visual impairment (amblyopia) in children. Understanding its classification helps you make the right diagnosis, recognise when strabismus signals neurological disease, and know when and where to refer. This module covers the classification, diagnosis, and management principles of strabismus from the MBBS perspective.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. New Age International, 2019. Ch. 17 (Strabismus) (textbook)
- Parsons JH (revised by Ramanjit Sihota, Radhika Tandon). Diseases of the Eye, 23rd ed. Elsevier, 2022. Ch. 24 (Squint) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A mother brings her 3-year-old son to the outpatient clinic. She has noticed that his right eye turns inward, especially when he is tired or looking at near objects. Her family physician had told her it was 'just a phase' and would resolve on its own. Now, six months later, you notice that the child preferentially uses his left eye — the right eye drifts inward and the child does not seem bothered by it. You perform a cover test and confirm right esotropia. Your senior colleague says, 'We need to get his refractive error checked — and amblyopia treatment must start now, before the critical period closes.' What does this mean, and what are the next steps?
WHY THIS MATTERS
Strabismus affects approximately 2–4% of children worldwide and is the leading cause of amblyopia (lazy eye) — a condition that permanently reduces vision in one eye if not treated before the critical period of visual development (approximately 7–8 years). Beyond childhood, new-onset strabismus in an adult signals neurological disease until proven otherwise. As a general practitioner or district hospital doctor, you will often be the first contact for parents worried about a child's squint — the ability to distinguish true from pseudostrabismus, recognise amblyopia risk, and refer appropriately is a core MBBS competency.
RECALL
From your ophthalmology posting and the EOM examination SDL, recall that the six extraocular muscles (four recti and two obliques) per eye maintain ocular alignment through balanced tone and the fusion reflex — the brain's drive to maintain single binocular vision by keeping the foveas of both eyes aligned on the same target. Fusion requires good vision in both eyes and an intact sensory and motor pathway. If fusion is impaired, the eyes may drift. From your earlier learning, recall that the cover/uncover test detects a manifest deviation (heterotropia/tropia) and the alternate cover test detects total deviation (tropia + phoria). The Hirschberg corneal reflex test gives an objective estimate without requiring patient cooperation — essential when examining toddlers.
Presentation: How Strabismus Comes to Attention
Strabismus comes to clinical attention through several different routes, and recognising each is important. The most common presentation in children is parental concern about a visible eye turn — one eye appearing to drift inward, outward, or upward, especially when the child is tired, ill, or concentrating on a near object. Parents often notice the deviation in photographs, where the corneal reflex asymmetry is easily visible. A less-obvious presentation is amblyopia — the child with suppression has no symptoms of diplopia, but the reduced vision in the deviated eye may be detected incidentally during a pre-school visual screening or school eye test. Vision screening programmes aim to catch amblyopia at the pre-school stage (3–5 years), when treatment is most effective.
In adults, the onset of diplopia (double vision) is the dominant presentation — this is because suppression of one image (as occurs in children) does not develop readily after the critical period of visual development. Any adult with new-onset diplopia requires a systematic evaluation to exclude neurological, vascular, or orbital causes. An abnormal head posture — head tilt, face turn, or chin elevation/depression — may develop as the patient unconsciously finds a gaze position where the diplopia is minimised or abolished (the null zone); this is seen in CN IV palsy (contralateral head tilt) and nystagmus. Finally, strabismus may be detected incidentally during a routine ophthalmic examination or general medical check-up.
Anatomy and Pathophysiology of Strabismus
Understanding why strabismus occurs requires integrating anatomy, sensory physiology, and the concept of the critical period of visual development. Under normal circumstances, the brain uses binocular fusion to merge slightly different images from each eye into a single, three-dimensional percept. Fusion depends on good visual acuity in both eyes, coordinated extraocular muscle balance, and an intact cortical fusion centre. When any of these components fail — whether because of refractive error, corneal opacity, cataract, or muscle imbalance — the visual axes may diverge and strabismus results.
In comitant childhood strabismus, the primary disturbance is usually an imbalance in the accommodation-convergence reflex. Accommodation (focusing the crystalline lens for near objects) is linked neurally to convergence: when a child accommodates to see a near target clearly, the eyes also converge. In a hypermetropic (long-sighted) child, the extra effort to accommodate (to overcome the refractive error) drives excessive convergence, and the eyes drift inward — this is the mechanism of accommodative esotropia. The AC/A ratio (accommodative convergence to accommodation ratio) quantifies this: a high AC/A ratio means a large convergent response per unit of accommodation, predisposing to esotropia.
Critically, in children under approximately 7–8 years of age, the visual cortex is still plastic — capable of reorganising in response to visual input. If one eye is chronically suppressed or deprived of clear images (as occurs when a child uses only the straight eye and suppresses the deviated eye's image to avoid diplopia), the cortical connections for the suppressed eye weaken, resulting in amblyopia — a persistent reduction in visual acuity that cannot be corrected by spectacles alone, because the problem lies in the cortex, not the optics. Amblyopia is reversible if treatment begins within the critical period, but becomes progressively harder to reverse after age 7–8 and essentially fixed by age 10–12.
The AC/A ratio is clinically important because an elevated AC/A ratio underlies high-AC/A accommodative esotropia, which responds to miotic drops (reducing accommodative effort) or bifocal glasses in addition to full correction of hypermetropia.
Classification of Strabismus: Comitant vs Incomitant
A systematic classification of strabismus is essential before any discussion of management, because the classification directly determines the diagnostic pathway, the investigation strategy, and the treatment plan. Without a clear classification framework, it is easy to order the wrong investigations (for example, performing cycloplegic refraction but omitting ductions) or to recommend the wrong treatment (prescribing spectacles for a non-accommodative esotropia, or — more dangerously — planning surgery before amblyopia therapy). The five-axis classification described below provides a complete clinical description of any squint from first principles, ensuring that no critical feature is omitted. In an OSCE or viva, presenting a strabismus case along these five axes signals that you have a logical, systematic approach rather than pattern-matching to a memorised list. Each axis is clinically actionable — the direction tells you whether to use base-in or base-out prism; the comitance axis tells you whether to investigate for a neurological cause; the accommodative status axis tells you whether spectacles will resolve the deviation. Strabismus is classified along five axes, each with clinical implications:
Provided image
- Direction of deviation: Esotropia (inward/convergent), exotropia (outward/divergent), hypertropia (upward), hypotropia (downward), cyclotropia (torsional). The direction combined with comitance determines the diagnostic pathway.
- Laterality: Unilateral strabismus (the same eye always deviates — the non-dominant eye); alternating strabismus (either eye may deviate, depending on fixation — the patient alternates between eyes). Alternating strabismus carries less amblyopia risk because both eyes alternate fixation, preventing persistent suppression of either eye.
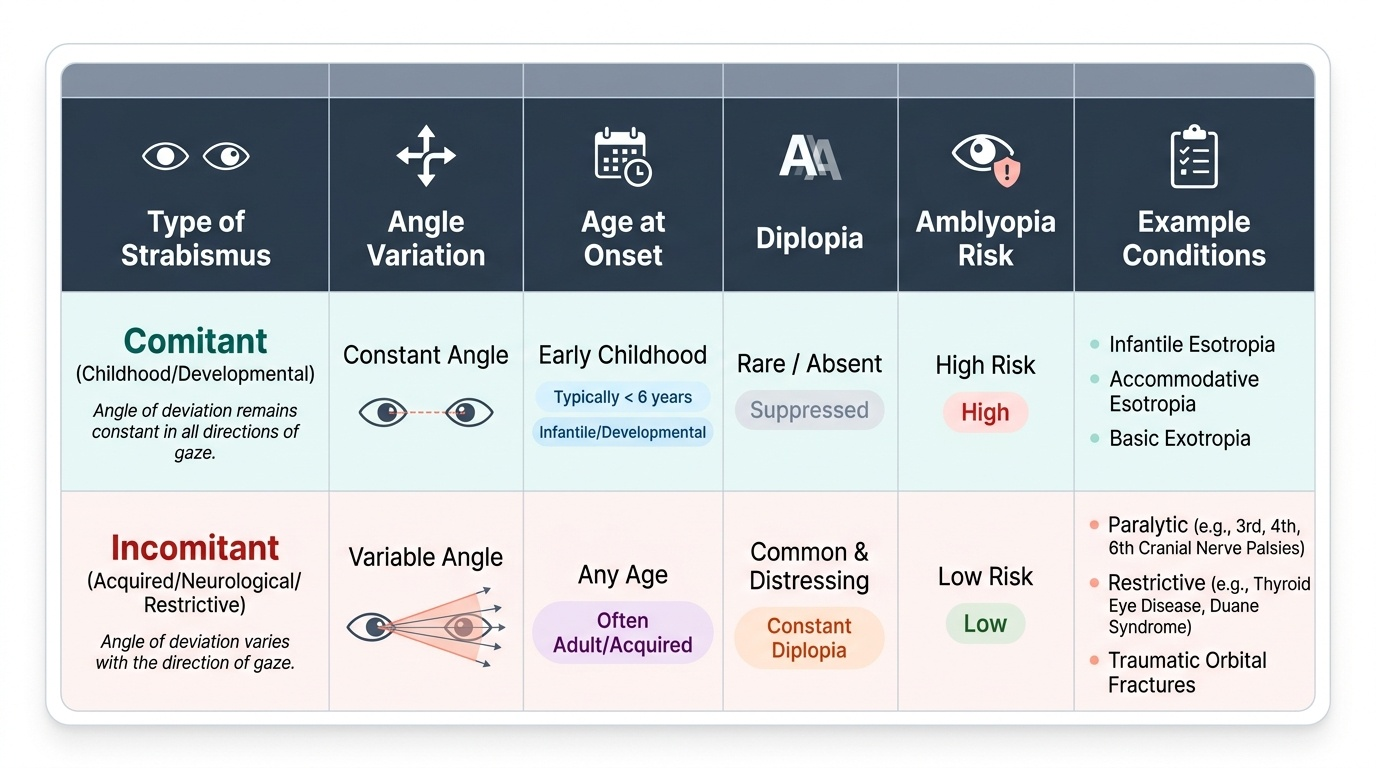
3. Comitance (the most clinically important axis):
- Comitant (concomitant) strabismus: The angle of deviation is EQUAL in all positions of gaze. The deviation does not increase or decrease when looking in any particular direction. This type is almost always of childhood onset and is caused by an imbalance in binocular control rather than a problem with individual muscles or their nerves. Importantly, the eye movement range of each eye individually (ductions) is FULL — there is no muscle weakness or restriction. Suppression and amblyopia are common because the deviated eye's image is chronically ignored. Diplopia is typically ABSENT in children due to suppression.
- Incomitant (paralytic/restrictive) strabismus: The angle of deviation VARIES with the direction of gaze — it is greatest in the field of action of the paretic muscle or in the direction of restriction. This type is typical of acquired CN palsies, orbital muscle restriction (thyroid eye disease, blow-out fracture), or myasthenia gravis. Ductions of the affected eye are LIMITED (unlike comitant strabismus). Diplopia is typically PRESENT because suppression has not developed (adult-onset).
- Onset: Congenital (onset <6 months — actually a misnomer; apparent from birth but possibly not true at birth) vs acquired. Congenital esotropia has a large angle (≥30 prism dioptres), is alternating, and is not accommodative.
- Accommodative status: Accommodative strabismus (fully corrected by spectacles for the refractive error — usually hypermetropia) vs non-accommodative. Partly accommodative strabismus is corrected partially but not fully by spectacles.
SELF-CHECK
A 5-year-old child has a constant right esotropia. Ductions of the right eye are full in all directions. The alternate cover test shows equal angle deviation in primary gaze, right gaze, and left gaze. There is no diplopia. What type of strabismus is this?
A. Incomitant paralytic esotropia — right CN VI palsy
B. Comitant esotropia — likely accommodative type
C. Incomitant restrictive esotropia — orbital blow-out fracture
D. Pseudostrabismus — angle kappa
Reveal Answer
Answer: B. Comitant esotropia — likely accommodative type
Full ductions, equal angle in all gazes, childhood onset, and absence of diplopia are the hallmarks of COMITANT strabismus. CN VI palsy (paralytic) would show limited abduction of the right eye on duction testing and increased angle on right gaze. In a 5-year-old with an esotropia and full ductions, the priority is cycloplegic refraction to determine if there is significant hypermetropia driving an accommodative component.