Page 6 of 32
OP10.2 | Heterotropia and Strabismus — SDL Guide (Part 2)
Common Comitant Strabismus Syndromes
The three most important comitant strabismus syndromes in clinical practice are infantile esotropia, accommodative esotropia, and intermittent exotropia.
Infantile (congenital) esotropia presents within the first six months of life with a large-angle constant esotropia (typically ≥30 prism dioptres). The deviation is alternating and non-accommodative — spectacle correction of any refractive error does not resolve it. The child typically shows cross-fixation: using the right eye to look to the left (adducting) and the left eye to look to the right, which can make the abduction movement appear limited and may be mistaken for CN VI palsy. Associated features include latent nystagmus, inferior oblique overaction, and dissociated vertical deviation (DVD). Treatment is surgical (bimedial rectus recession) once the angle is stable and refractive error is optimally corrected. Amblyopia is treated first.
Accommodative esotropia typically presents at 2–3 years of age, when the child begins intense near visual tasks. The esotropia is driven by excessive accommodative convergence to overcome hypermetropia, usually +2.00 to +7.00 DS or more. In fully accommodative esotropia, complete spectacle correction of the hypermetropia abolishes the deviation — no surgery is needed, and the child must wear the glasses consistently until the accommodation-convergence linkage matures (often into the teenage years). In high-AC/A accommodative esotropia, the angle at near is much larger than at distance — bifocal glasses (executive bifocals) reduce the near accommodative effort. Partially accommodative esotropia responds to glasses but retains a residual deviation requiring surgery.
Intermittent exotropia is the commonest exodeviation in childhood. The eyes are straight most of the time (maintaining fusion) but the patient intermittently drifts outward, typically on distant fixation, daydreaming, or bright sunlight. Parents notice the exodeviation before the child does. Amblyopia is uncommon because the child predominantly fuses. Management depends on the frequency and control — patching, exercises, or surgery if the deviation is poorly controlled.
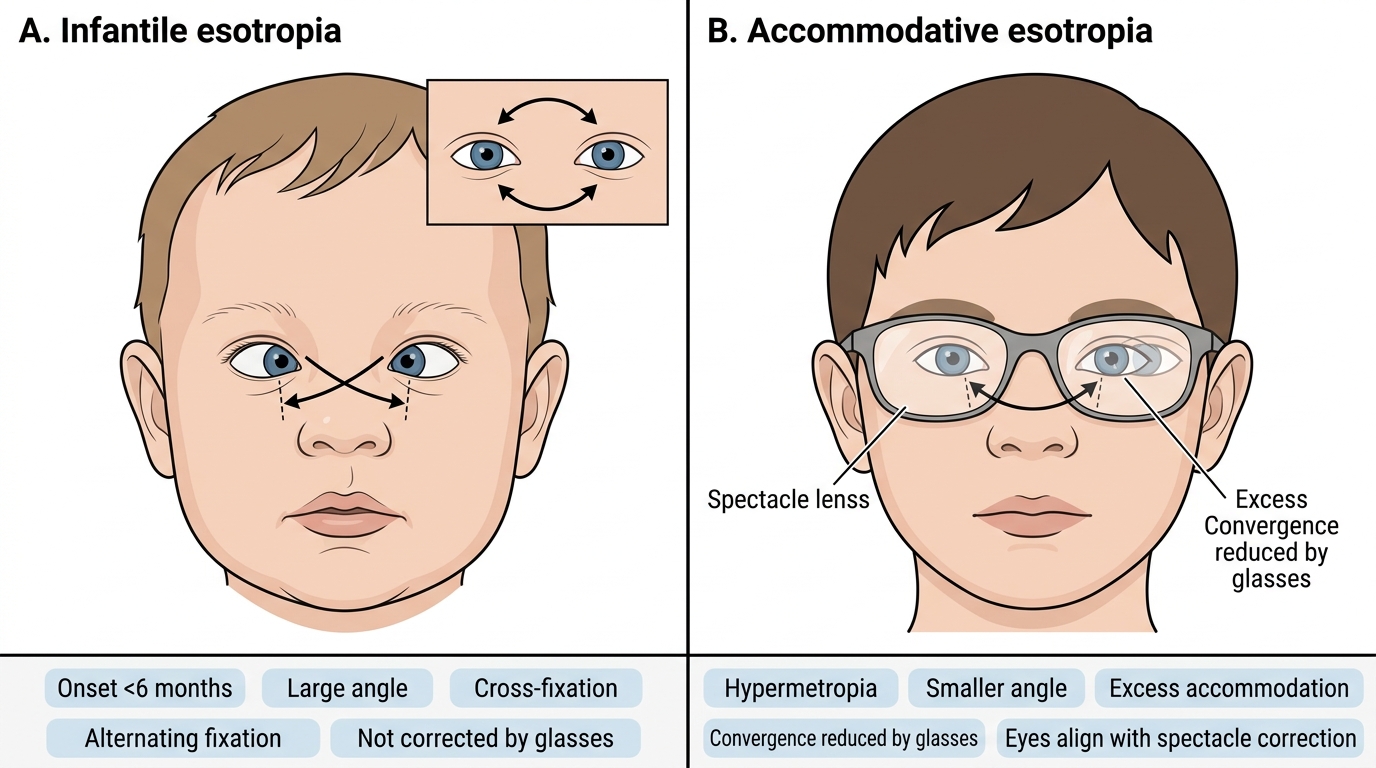
Infantile vs Accommodative Esotropia
Incomitant (Paralytic) Strabismus: CN Palsy Patterns
Incomitant strabismus is caused by failure of one or more extraocular muscles — either neurological (cranial nerve palsy) or mechanical (restriction). The key distinguishing feature from comitant strabismus is that the angle of deviation changes with gaze direction and the duction of the affected eye is limited. Diplopia is the dominant symptom in adults.
CN VI (abducens) palsy: The lateral rectus is paretic; the affected eye fails to abduct. The patient develops a convergent squint (esotropia) at distance, worse on ipsilateral gaze, with horizontal diplopia (images side by side) that increases on looking toward the paretic side. The patient adopts a face turn toward the affected side to move the eyes into the less-affected field. Causes include microvascular (diabetes, hypertension — most common in adults), raised intracranial pressure (CN VI is a false-localising sign with ICP elevation), skull base tumours, trauma, and Gradenigo's syndrome (petrous apex infection). Isolated CN VI palsy in a diabetic is the most common presentation for an MBBS viva.
CN IV (trochlear) palsy: The superior oblique is paretic; the eye shows hypertropia (upward deviation) that is worst on ipsilateral gaze and on contralateral head tilt (Parks-Bielschowsky three-step test positive). The patient develops a characteristic contralateral head tilt (tilting the head away from the affected side reduces torsional diplopia). CN IV palsy may be congenital (detected in adulthood by decompensation) or acquired (trauma — CN IV has the longest intracranial course and is the nerve most vulnerable to closed head injury).
CN III (oculomotor) palsy: The most dramatic palsy — ptosis, eye deviated down and out (lateral rectus and superior oblique are unopposed), and if the pupillomotor fibres are involved, a fixed dilated pupil. Causes: compressive (posterior communicating artery aneurysm — urgent — pupil involved), microvascular (diabetic — usually pupil-sparing), or midbrain pathology. A painful complete CN III palsy with a dilated pupil is a neurosurgical emergency.
Mechanical restriction (thyroid eye disease — tight inferior rectus causes inability to elevate; blow-out fracture — entrapped inferior rectus causes limitation of elevation) mimics inferior rectus palsy of the other eye but the forced duction test is positive (resistance to passive movement confirms mechanical restriction rather than paresis).
Examination and Investigation of Strabismus
A structured examination sequence ensures you detect both the deviation and its complications (amblyopia). The sequence recommended by Khurana and Parsons proceeds as follows:
1. Visual acuity (each eye separately): In a preverbal child, use preferential looking or Cardiff cards; in a cooperative child aged ≥3, use crowded Kay pictures or Sheridan-Gardiner optotypes. Reduced VA in the deviating eye raises suspicion of amblyopia.
2. Corneal reflexes and Hirschberg test: Objective estimate of deviation; identifies which eye is deviating and estimates the approximate angle. 1 mm decentration ≈ 7°; at the pupil margin ≈ 15°; at the iris margin ≈ 30–45°.
3. Cover/uncover test: Detects heterotropia; identifies which eye is deviating and the direction of movement (outward movement on covering the fellow eye = esotropia of the uncovered eye; inward movement = exotropia).
4. Alternate cover test: Detects total deviation (tropia + phoria); measures the full amplitude of deviation. Used with prisms (PACT) to quantify in prism dioptres.
5. Ductions and versions: Ductions confirm full extraocular movement range of each eye (rules out paralytic/restrictive strabismus). Versions expose any limitation in conjugate gaze.
6. Cycloplegic refraction: MANDATORY in any child with strabismus. Cyclopentolate 1% drops (or atropine 1% in dark-eyed children for full cycloplegia) are instilled to paralyse accommodation before the refraction — without cycloplegia, the child's accommodative effort masks the underlying hypermetropia. Significant hypermetropia driving an accommodative esotropia will be missed without cycloplegic refraction.
7. Fundus examination: Retinoscopy + fundus to exclude an organic cause for visual loss (tumour, optic nerve hypoplasia, retinal disease) that might have caused the sensory strabismus.
8. Prism cover test (quantification): Prisms are placed in front of the fixing or deviated eye (as per convention) to neutralise the corrective fixation movement — the prism power at neutralisation = the angle of strabismus in prism dioptres.