Page 15 of 30
OP2.5 | Cavernous Sinus Thrombosis: Ocular Features and Management — SDL Guide
Learning Objectives
- Describe the anatomy of the cavernous sinus and identify its cranial nerve and vascular contents
- Explain the venous pathways by which infection reaches the cavernous sinus from orbital, facial, dental, and ENT sources
- Identify the characteristic ocular findings on examination in cavernous sinus thrombosis
- Distinguish cavernous sinus thrombosis from bilateral orbital cellulitis and other causes of bilateral proptosis and ophthalmoplegia
- Outline the management of septic cavernous sinus thrombosis including antibiotic choice, anticoagulation, and indications for surgical intervention
- Describe the complications and prognosis of cavernous sinus thrombosis
INSTRUCTIONS
Cavernous sinus thrombosis is the most severe complication of orbital and facial infections — a condition with 20–30% mortality even in the antibiotic era. It is Chandler Stage V of orbital cellulitis and marks the transition from an orbital emergency to a neurological emergency. The bilateral ophthalmoplegia, bilateral proptosis, and meningism syndrome in a febrile patient is one of the most dramatic presentations in clinical medicine. This module equips you to recognise CST immediately, understand its anatomy, and initiate life-saving treatment.
References
- AK Khurana — Comprehensive Ophthalmology, 7th ed., Ch 16 (Orbital Disease & CST) (textbook)
- Parsons' Diseases of the Eye, 23rd ed., Ch 16 (The Orbit) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 16-year-old student is admitted to the medicine ward with a four-day history of worsening headache, high fever, and now double vision. Two weeks ago he squeezed a painful boil on his upper lip. On examination: temperature 39.8°C, he looks toxic and confused; bilateral proptosis (both eyes are pushed forward), both eyes are nearly fixed in position — he cannot move either eye in any direction; his neck is stiff; there is bilateral periorbital oedema and chemosis; fundoscopy shows bilateral papilloedema. This patient has cavernous sinus thrombosis. The bacteria from his facial boil travelled through the valveless veins of the face into the cavernous sinus. Understanding the anatomy of that pathway — and what is inside the cavernous sinus — is the key to understanding every feature of this devastating presentation.
WHY THIS MATTERS
Cavernous sinus thrombosis is uncommon but carries high mortality (20–30%) and significant morbidity even with treatment. It is encountered in district hospitals and tertiary centres, most often as a complication of facial or orbital infections. In India, where facial furuncles and dental infections are prevalent and access to early care is variable, CST is more commonly seen than in high-income countries. NMC OP2.5 requires you to describe the ocular examination findings and management — but understanding the condition requires starting with the anatomy. This module also consolidates the orbital cellulitis content from OP2.4, since CST is Chandler Stage V.
RECALL
From Year-1 Anatomy: (1) The cavernous sinus is a paired, irregular venous lake at the base of the skull, lateral to the sella turcica and pituitary gland, on either side of the body of the sphenoid bone. (2) It receives drainage from the superior ophthalmic vein, inferior ophthalmic vein, superficial middle cerebral vein, and sphenoidal emissary veins. (3) It drains posteriorly via the superior and inferior petrosal sinuses into the sigmoid sinus and internal jugular vein. (4) From OP2.4: the ophthalmic veins are valveless — they can carry infected thrombus retrogradely from the orbit to the cavernous sinus. (5) The 'danger triangle' of the face (nose, upper lip, nasolabial fold) drains via the facial vein, which communicates with the ophthalmic vein — infected thrombus from a squeezed facial boil can track all the way to the cavernous sinus.
Clinical Presentation: Bilateral Proptosis and Ophthalmoplegia with Systemic Toxicity
Cavernous sinus thrombosis presents as an acute, life-threatening syndrome combining orbital, cranial nerve, and systemic sepsis features. The clinical hallmark that distinguishes CST from all other orbital pathologies — including orbital cellulitis — is bilateral involvement: proptosis, ophthalmoplegia, and periorbital signs that cross the midline. This bilaterality occurs because the two cavernous sinuses are connected by the anterior and posterior intercavernous sinuses; once infected thrombus reaches one sinus, it can propagate to the other, producing bilateral cranial nerve palsies and bilateral proptosis simultaneously or in rapid sequence.
The clinical presentation unfolds in a typical sequence: (1) a primary infection (facial boil, dental abscess, orbital cellulitis, sinusitis, otitis media) is present or has recently resolved; (2) high-grade fever, rigors, and toxicity develop; (3) the patient develops a headache that is severe and retro-orbital; (4) unilateral periorbital oedema, proptosis, and ophthalmoplegia appear; (5) within hours to days, the CONTRALATERAL eye becomes involved (bilateral proptosis, bilateral ophthalmoplegia — the pathognomonic sign); (6) meningism (neck stiffness, photophobia, Kernig's sign) develops from meningeal irritation; (7) papilloedema from raised intracranial pressure and retinal venous congestion; (8) altered consciousness if cerebral involvement or septic emboli occur.
Key symptoms reported by the patient or family:
- Severe headache (often described as the worst of their life)
- Diplopia (double vision) — from multiple cranial nerve palsies
- Visual blurring or loss — from corneal exposure, papilloedema, or retinal venous congestion
- Neck stiffness and photophobia — meningeal involvement
- Confusion or reduced consciousness — septic encephalopathy or cerebral vein involvement
Cavernous Sinus Contents and Venous Connections
Anatomy of the Cavernous Sinus and Venous Pathways of Spread
A thorough understanding of cavernous sinus anatomy is essential because the anatomy directly predicts which neurological signs will appear, in which order, and how the infection reached the sinus. The cavernous sinus is not a simple vessel — it is a complex venous lake whose relationships with cranial nerves and the internal carotid artery determine the clinical syndrome.
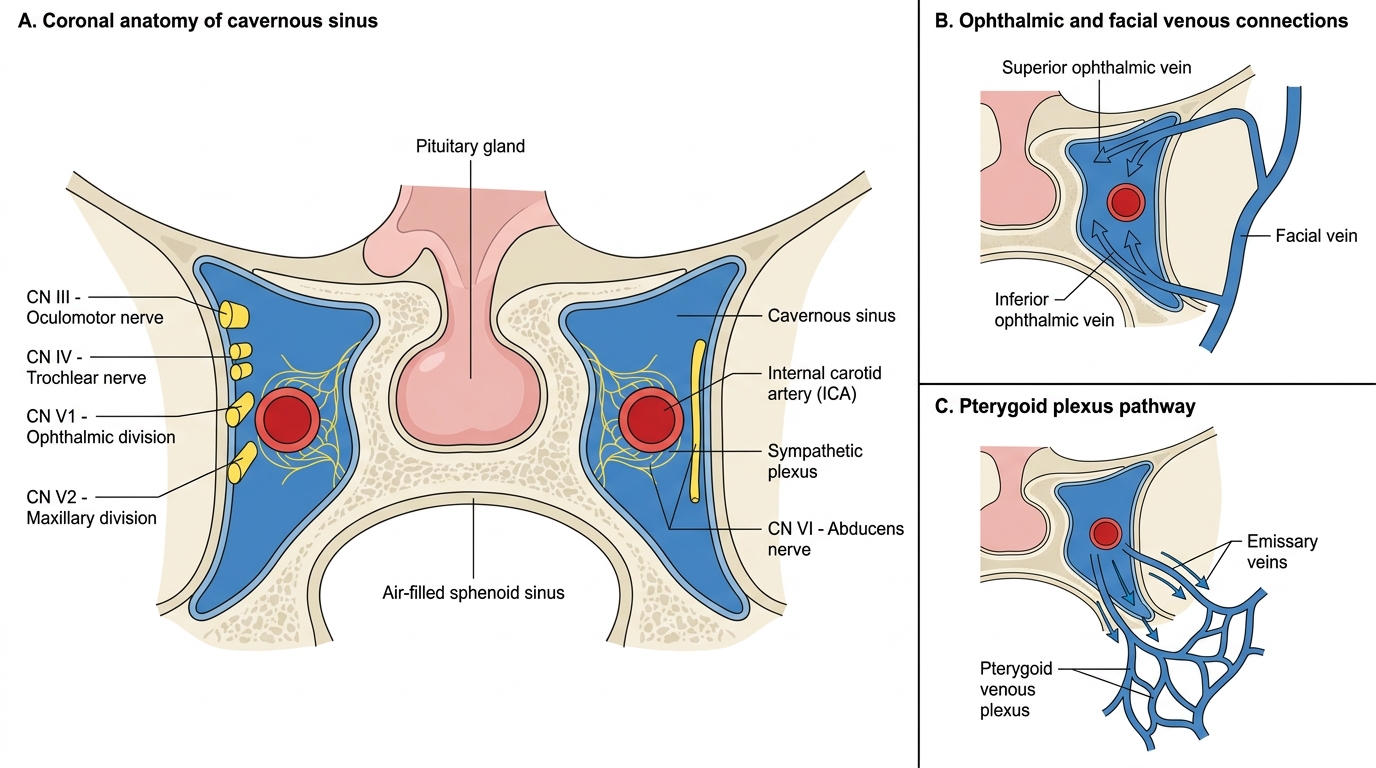
Contents of the cavernous sinus: The lateral wall of the cavernous sinus, from superior to inferior, contains: CN III (oculomotor nerve — upper division to superior rectus and levator; lower division to medial rectus, inferior rectus, inferior oblique, and pupillary constrictor), CN IV (trochlear — supplies superior oblique), CN V1 (ophthalmic division — sensory to forehead, upper lid, cornea), CN V2 (maxillary division — sensory to cheek, lower lid, upper teeth). Running through the body of the sinus itself (not in the wall but in the lumen, exposed to the venous blood) are CN VI (abducens nerve — supplies lateral rectus) and the internal carotid artery (ICA) with its surrounding sympathetic plexus.
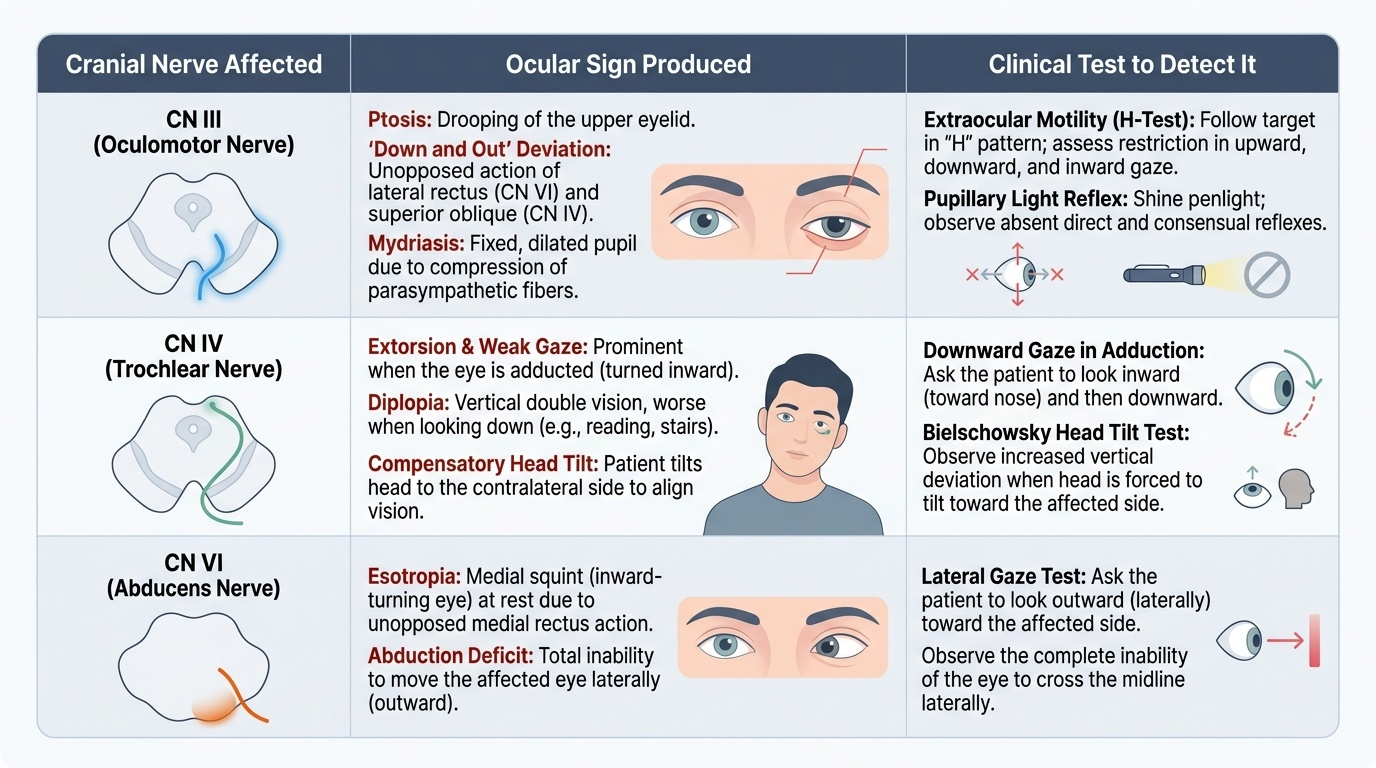
Because CN VI runs through the lumen — in direct contact with the venous blood — it is the most vulnerable nerve and is the first cranial nerve to be affected in CST, producing a lateral rectus palsy (failure of abduction, producing an esotropia or medial squint on attempted lateral gaze). CN III palsy produces ptosis, a fixed dilated pupil (mydriasis), and deviation of the eye downward and outward ('down and out'). CN IV palsy produces vertical diplopia. V1 and V2 involvement produces periorbital hyperaesthesia or anaesthesia. Sympathetic plexus involvement around the ICA may produce Horner syndrome (ptosis, miosis, anhidrosis).
Venous pathways of infection spread: (1) Orbital route (most common): superior and inferior ophthalmic veins (valveless) carry infected thrombus from the orbital cellulitis retrograde into the cavernous sinus. This is Chandler Stage V. (2) Facial route ('danger triangle'): the angular vein and facial vein in the upper lip-nose region communicate with the ophthalmic veins; infected thrombus from squeezing a facial furuncle propagates to the cavernous sinus via this route. The 'danger triangle' of the face — bounded by the corners of the mouth and the nose — is a classic clinical teaching: never squeeze a boil in this area. (3) Dental route: upper molar teeth drain to the pterygoid plexus, which connects to the cavernous sinus; dental abscesses can produce CST. (4) Otogenic route: infection from the mastoid or middle ear spreads via the inferior petrosal sinus. (5) Sphenoidal sinusitis: the sphenoid sinus has a direct relationship with the cavernous sinus roof — sphenoid sinusitis is a classic and often under-recognised cause of CST.
SELF-CHECK
In a patient with early septic cavernous sinus thrombosis, which cranial nerve palsy is expected to appear FIRST and what is its anatomical basis?
A. CN III palsy — because it is the largest cranial nerve in the sinus and most vulnerable to compression
B. CN VI palsy — because it runs through the lumen of the cavernous sinus in direct contact with the venous blood, making it most exposed to thrombosis and raised pressure
C. CN V1 palsy — because V1 runs in the superior part of the lateral wall, nearest to the ophthalmic vein drainage
D. CN IV palsy — because the trochlear nerve is the thinnest and most easily compressed
Reveal Answer
Answer: B. CN VI palsy — because it runs through the lumen of the cavernous sinus in direct contact with the venous blood, making it most exposed to thrombosis and raised pressure
CN VI (abducens nerve) runs through the body of the cavernous sinus lumen itself — not in the lateral wall like CN III, IV, V1, and V2 — placing it in direct contact with the infected venous blood and making it most vulnerable to thrombosis and pressure effects. CN VI palsy (lateral rectus palsy) therefore typically presents first in CST, causing an inability to abduct the affected eye. CN III is in the superior lateral wall; its palsy (ptosis, mydriasis, 'down and out' deviation) appears later as inflammation spreads.
Ocular Examination Findings in CST
The ocular examination in CST must be both systematic and rapid — the clinical findings serve both diagnostic and monitoring purposes. The key is that virtually every structure innervated by the contents of the cavernous sinus is affected, and the combination of bilateral involvement with systemic sepsis is diagnostic.
Provided image
Visual acuity: may be reduced from corneal exposure (lagophthalmos from proptosis + ophthalmoplegia), from raised intracranial pressure affecting the optic nerve (papilloedema leading to obscurations), or from central retinal vein occlusion (CRVO) due to venous congestion. VA should be checked in both eyes, both with spectacle correction and pinhole.
Pupil reactions: CN III palsy affects the pupilloconstrictor fibres (they travel in the outer aspect of CN III and are compressed early) — producing a fixed, dilated pupil (mydriasis) with absent direct and consensual light reflexes on the affected side. Bilateral pupil involvement may occur in advanced bilateral CST. A Horner syndrome (miosis + partial ptosis + anhidrosis) on one side may occur from ICA sympathetic plexus involvement.
Proptosis and chemosis: Forward displacement of both globes with severe conjunctival chemosis, periorbital oedema; the chemosis is typically more pronounced than in orbital cellulitis alone because raised intraorbital and intracranial pressure impairs venous drainage from the conjunctival surface.
Extraocular movements: Multiple cranial nerve palsies produce a complex ophthalmoplegia. In early CST, CN VI palsy is isolated — the eye cannot abduct, producing an esotropia (medial squint). As the disease progresses, CN III palsy adds ptosis and a 'down and out' deviation; CN IV palsy adds vertical diplopia. Complete ophthalmoplegia (the eye is fixed in all positions) occurs in severe CST when all three nerves are affected simultaneously.
Sensory findings: CN V1 involvement produces reduced corneal sensation (check with a wisp of cotton wool, comparing both eyes) and periorbital hyperaesthesia; CN V2 involvement produces cheek numbness. These sensory changes are important exam findings.
Fundoscopy: Bilateral papilloedema from raised intracranial pressure; dilated, tortuous retinal veins from venous congestion; CRVO in severe cases.
Systemic examination: neck stiffness (Kernig's sign), altered consciousness, fever — must be documented alongside the ocular findings.