Page 16 of 30
OP2.5 | Cavernous Sinus Thrombosis: Ocular Features and Management — SDL Guide (Part 2)
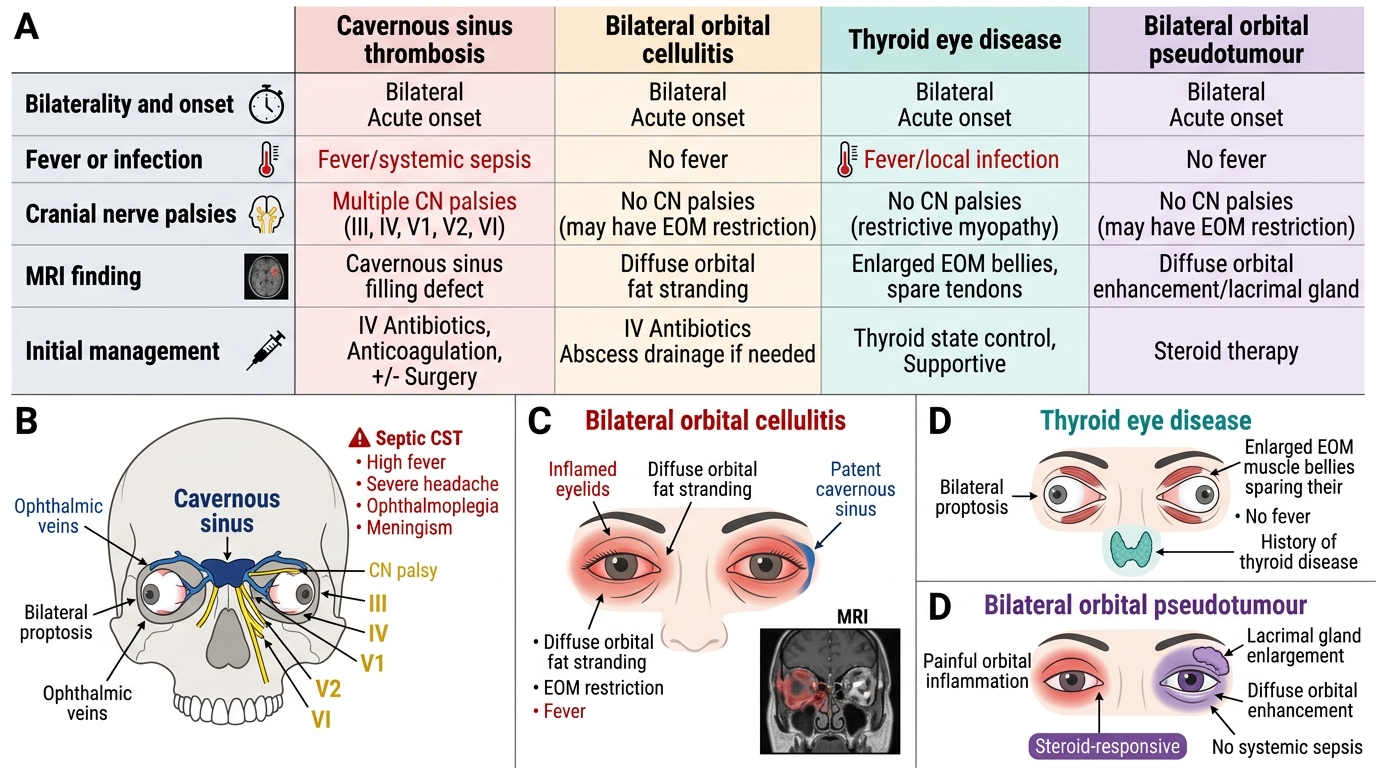
Diagnosis: Distinguishing CST from Other Causes of Bilateral Orbital Involvement
The diagnosis of CST is clinical, supported by imaging and laboratory findings. The key diagnostic challenge is distinguishing CST from bilateral orbital cellulitis, bilateral TED, and other causes of bilateral proptosis — because the management is fundamentally different.
Clinical diagnostic features that CONFIRM CST over orbital disease: (1) Bilateral proptosis and ophthalmoplegia that developed in rapid sequence (hours), especially if one eye was initially normal; (2) meningism (neck stiffness, photophobia, Kernig's sign); (3) multiple cranial nerve palsies in the same eye or bilaterally (CN VI + III + IV + V1 in one examination session); (4) ICA involvement signs — contralateral hemiparesis from septic thrombosis of the ICA or its branches.
Investigations: CT brain and orbits with contrast: the CT shows proptosis, enlarged EOMs, orbital fat haziness, and — critically — filling defects in the cavernous sinus (non-enhancement of the sinus after contrast, or expansion of the sinus with loss of the normal concave lateral wall) on axial cuts. MRI with gadolinium and MR venography is more sensitive for CST: filling defect, expansion, and heterogeneous signal in the cavernous sinus; also detects intracranial complications (subdural empyema, cerebral abscess, cortical venous thrombosis). Blood investigations: FBC (leucocytosis), raised CRP/ESR, blood cultures (often positive), coagulation studies, D-dimer (elevated in thrombosis); lumbar puncture if meningism is present (contraindicated if CT shows raised ICP with mass effect or tonsillar herniation).
Bilateral Proptosis: Key Differentials
Differential diagnosis: Bilateral orbital cellulitis (bilateral simultaneous onset without meningism, fever plus EOM restriction but usually less extensive CN palsies, no cavernous sinus filling defect on MRI); TED (bilateral, no fever, no CN palsies beyond EOM restriction from muscle fibrosis, known thyroid disease); bilateral orbital pseudotumour (bilateral, painful, steroid-responsive, no systemic sepsis); mucormycosis (immunocompromised, black eschar, can involve cavernous sinus directly via sphenoid).
SELF-CHECK
An 18-year-old woman developed a dental abscess three weeks ago and was prescribed oral amoxicillin. She now presents with bilateral eye swelling, cannot move either eye, temperature 40°C, severe headache, and neck stiffness. MRI shows filling defects in both cavernous sinuses and bilateral proptosis. The blood culture grows Streptococcus milleri. What is the correct initial antibiotic regimen?
A. Oral co-amoxiclav 625 mg TDS — the same antibiotic family as her initial treatment but at higher dose
B. IV ceftriaxone 2 g BD (plus metronidazole for dental source anaerobes) — broad-spectrum IV treatment for septic CST
C. IV vancomycin alone — for MRSA cover
D. IV methylprednisolone — to reduce cavernous sinus inflammation
Reveal Answer
Answer: B. IV ceftriaxone 2 g BD (plus metronidazole for dental source anaerobes) — broad-spectrum IV treatment for septic CST
Septic CST from a dental source requires immediate broad-spectrum IV antibiotics to cover streptococci, staphylococci, and oral anaerobes. IV ceftriaxone (2 g BD) plus IV metronidazole (500 mg TDS) is appropriate for this dental-source CST — ceftriaxone covers streptococcal and many gram-negative organisms with good CNS penetration; metronidazole covers oral anaerobes. Oral antibiotics are entirely inappropriate for a condition with 20–30% mortality. Vancomycin alone would miss the gram-negative and anaerobic component. IV steroids would be harmful in active septic thrombosis without prior aggressive antibiotics.
Management: IV Antibiotics, Anticoagulation and Supportive Care
Management of septic CST is a multidisciplinary emergency involving ophthalmology, neurology, neurosurgery, otolaryngology, and intensive care. The principles are: aggressive IV antibiotics to eradicate the infection, anticoagulation to prevent clot propagation (controversial), management of the primary infection source, supportive care, and monitoring for complications.
IV antibiotics: Should be started immediately, without waiting for culture results. The initial regimen must cover Staphylococcus aureus (including MRSA if suspected — community-acquired or hospital setting), Streptococcus species, gram-negative organisms, and anaerobes (especially if dental or sinus source). Recommended regimens: (1) IV ceftriaxone 2 g BD (excellent CNS penetration) + IV metronidazole 500 mg TDS (anaerobes) — first-line for most cases. (2) Add IV vancomycin 15–20 mg/kg BD if MRSA is suspected or confirmed on culture. (3) IV piperacillin-tazobactam or meropenem if gram-negative or polymicrobial infection is suspected. Duration: minimum 3–4 weeks of IV antibiotics, followed by oral antibiotics to complete 6 weeks total.
Anticoagulation: The evidence base is limited (no RCTs). Rationale for anticoagulation: the thrombus propagates via the intercavernous and superior/inferior petrosal sinuses; heparin anticoagulation may limit progression and reduce the risk of cortical vein thrombosis and stroke. Rationale against: risk of haemorrhage into septic foci; risk of spreading infected clot. Current practice: anticoagulation is offered (low molecular weight heparin transitioning to warfarin or DOAC) in patients without active haemorrhage, guided by the treating physician and neurologist jointly. The decision is clinical and individualised; the ophthalmologist should document the ocular examination findings that supported the diagnosis and alert the team to any new visual deterioration.
Source control: Drainage of any accessible primary infection — dental abscess (emergency dental extraction or incision and drainage), orbital abscess (surgical drainage per Chandler criteria), sphenoid sinusitis (endoscopic drainage), mastoid abscess (mastoidectomy). Functional endoscopic sinus surgery (FESS) for sinusitis-related CST. Elimination of the primary source prevents ongoing bacteraemia seeding the thrombus.
Supportive care: IV fluids for sepsis; ICU monitoring if hemodynamically unstable; anticonvulsants if seizures occur; management of raised intracranial pressure (head elevation, mannitol if cerebral oedema); eye care — lubricant drops every hour, ointment at night, moisture chamber glasses, and tarsorrhaphy if corneal exposure develops; ophthalmology monitoring of VA and pupils twice daily.
Complications and Long-Term Sequelae
Even with optimal management, CST carries a mortality of approximately 20–30% and a high rate of permanent morbidity. Understanding the complication profile is important both for monitoring and for counselling the family.
Ophthalmic complications: (1) Permanent cranial nerve palsies — despite treatment, CN VI, III, or IV palsies may persist for months or permanently, producing strabismus, ptosis, or chronic diplopia requiring eventual strabismus or lid surgery. (2) Blindness from optic nerve involvement — compression by oedema, central retinal artery or vein occlusion, or papilloedema-related optic atrophy; the risk of permanent visual loss is 5–20% in survivors. (3) Corneal scarring from exposure keratopathy if lagophthalmos is untreated.
Neurological complications: (1) Meningitis — from direct spread to the subarachnoid space; CSF pleocytosis on LP. (2) Cerebral abscess — septic emboli from the cavernous sinus reaching the cerebral vasculature; presents with focal neurological deficits. (3) Cortical venous sinus thrombosis — spread to the superior sagittal sinus or sigmoid sinus; may cause venous infarcts, haemorrhage, or seizures. (4) Stroke — arterial stroke from ICA involvement (arteritis or septic emboli from the ICA within the sinus). (5) Pituitary infarction — the pituitary gland is enclosed by the cavernous sinus; thrombosis and inflammation can compromise pituitary blood supply.
Systemic complications: septicaemia, septic emboli to lungs (septic pulmonary emboli), endocarditis, DIC.
Prognosis: In the pre-antibiotic era, CST was nearly universally fatal. With modern IV antibiotics, mortality is 20–30%. Factors associated with worse prognosis: delayed diagnosis, immunocompromised state (diabetics, haematological malignancy), ICA involvement (stroke risk), bilateral cerebral involvement.
SELF-CHECK
A patient recovering from septic CST is noted to have left esotropia (left eye deviated medially, cannot abduct past midline) that has persisted for 3 months despite completed antibiotic treatment. Which cranial nerve was most likely affected, and what long-term ophthalmic management might be required?
A. CN III palsy — left ptosis surgery and inferior rectus recession
B. CN VI palsy — left lateral rectus palsy producing esotropia; may require strabismus surgery (medial rectus recession ± lateral rectus resection) if persistent
C. CN IV palsy — left superior oblique palsy requiring inferior oblique weakening
D. CN II palsy — optic nerve damage requiring no specific treatment
Reveal Answer
Answer: B. CN VI palsy — left lateral rectus palsy producing esotropia; may require strabismus surgery (medial rectus recession ± lateral rectus resection) if persistent
CN VI (abducens nerve) palsy produces lateral rectus palsy — the affected eye deviates medially at rest (esotropia) and cannot abduct (look outward) past the midline. CN VI is the first and most commonly permanently damaged nerve in CST because of its position in the sinus lumen. After recovery from the acute illness, persistent esotropia from CN VI palsy is managed with prism spectacles initially (to correct the diplopia); if it does not resolve within 6 months (spontaneous nerve recovery), strabismus surgery (medial rectus recession with or without lateral rectus resection) is performed. CN III palsy produces a 'down-and-out' deviation with ptosis and mydriasis, not esotropia.
CLINICAL PEARL
The pathognomonic sign of cavernous sinus thrombosis is bilateral involvement — bilateral proptosis, bilateral ophthalmoplegia, bilateral periorbital oedema. No other cause of proptosis and ophthalmoplegia simultaneously affects both orbits this rapidly except CST. When you see a patient with bilateral 'orbital signs' appearing in rapid succession (one eye, then the other within hours), think CST until proven otherwise and act immediately. The second essential teaching: CN VI palsy appears first in CST because CN VI runs through the venous lumen of the cavernous sinus — this anatomical fact also explains why CN VI is the most commonly permanently damaged nerve. An isolated CN VI palsy in a febrile patient with headache should always raise suspicion for CST even before bilateral signs develop.
Self-Assessment: Cavernous Sinus Thrombosis
Self-assessment for cavernous sinus thrombosis must integrate the anatomy of the cavernous sinus and its venous connections, the clinical syndrome that results when this sinus becomes infected and thrombosed, the investigations that confirm the diagnosis and exclude mimics, and the management protocol — including the controversial role of anticoagulation in a septic thrombosis setting. CST is rare but high-stakes: misdiagnosis as orbital cellulitis or preseptal cellulitis leads to inadequate treatment, and the bilateral spread — which is pathognomonic of cavernous sinus involvement — can occur rapidly once the contralateral cavernous sinus is reached via the intercavernous sinus. The mortality of untreated CST historically exceeded 50%; with modern IV antibiotics it falls to around 10-20%, but blindness from ophthalmic vein occlusion and neurological deficits from cranial nerve damage remain significant sequelae.
- A 25-year-old man presents with a rapidly progressive right proptosis and ophthalmoplegia following a skin furuncle on the right alar of the nose. Within 24 hours, similar but milder signs appear on the left side, and he becomes febrile and confused. What is the diagnosis and what is the primary imaging investigation of choice?
- Which cranial nerves pass through the cavernous sinus and which pass in the lateral wall? Name the clinical signs produced by their involvement in CST.
- Explain the anatomical route by which a nasal furuncle leads to cavernous sinus thrombosis.
- What antibiotic regimen is used in septic cavernous sinus thrombosis, and what is the evidence base and controversy regarding anticoagulation?
- Name four sequelae of cavernous sinus thrombosis in a patient who survives.
Expected answers: (1) Cavernous sinus thrombosis; MRI brain with gadolinium and MR venography (or CT with contrast as first-line if MRI unavailable). (2) CN III (oculomotor), CN IV (trochlear), CN V1 and V2 (ophthalmic and maxillary divisions of trigeminal) run in the lateral wall of the sinus; CN VI (abducens) runs freely in the sinus lumen, exposed to venous blood, making it the first cranial nerve to be affected in CST. Signs: III palsy (ptosis, mydriasis, loss of upgaze/downgaze/adduction), IV palsy (loss of infraduction in adduction), VI palsy (lateral rectus, most commonly affected), V1 sensory loss (forehead, corneal reflex), proptosis (ophthalmic vein obstruction). (3) Nasal furuncle → facial vein → angular vein → ophthalmic vein (valveless) → cavernous sinus. (4) IV broad-spectrum antibiotics targeting Staphylococcus aureus (including MRSA if healthcare-associated): vancomycin + piperacillin-tazobactam + metronidazole; anticoagulation with IV heparin is used in many centres to limit thrombus propagation but evidence is from case series, not RCTs; benefit in septic thrombosis remains debated. (5) Blindness (ophthalmic vein occlusion → central retinal vein → retinal ischaemia), persistent cranial nerve palsies, pituitary insufficiency (pituitary gland supplied by cavernous sinus), meningitis/brain abscess, septicaemia and septic emboli.