Page 5 of 30
OP2.2 | Lid and Lacrimal Procedures: Bell Phenomenon, Ptosis Evaluation, Massage and Epilation — SDL Guide
Learning Objectives
- Demonstrate and interpret Bell's phenomenon and explain its clinical significance before lid and ptosis surgery
- Perform a structured ptosis evaluation including MRD-1, levator function, and upper lid crease measurement
- Describe and demonstrate the Crigler's massage technique for congenital nasolacrimal duct obstruction
- Perform epilation of aberrant eyelashes and explain when permanent eyelash removal is indicated
- Integrate findings from ptosis evaluation to guide surgical decision-making
INSTRUCTIONS
NMC competency OP2.2 requires you to demonstrate four specific lid and lacrimal procedures under supervision. These are not just technical exercises — each procedure generates information that directly changes management. Getting a negative Bell's phenomenon before ptosis surgery can prevent a corneal disaster; getting MRD-1 and levator function wrong leads to the wrong operation. This module takes a skills-arc approach: indication → anatomy/instrument → technique → interpretation → applied clinical reasoning.
References
- AK Khurana — Comprehensive Ophthalmology, 7th ed., Ch 1 & Ch 19 (Disorders of the Lids; Strabismus and Ptosis) (textbook)
- Parsons' Diseases of the Eye, 23rd ed., Ch 1 & Ch 26 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are in the ophthalmic OPD when a mother brings in her six-month-old infant. The child's right eye is permanently watering, with intermittent mucopurulent discharge from the medial canthal area. The mother has been told to 'massage the eye' but doesn't know how. Across the room, a senior surgeon examining a 12-year-old boy with drooping of the left upper lid writes down two numbers — MRD-1 and levator function — and uses them to choose an operation. Meanwhile, a 35-year-old woman winces as each misdirected eyelash is pulled out with forceps. Four different procedures, one module. By the end, you will know not just how to perform each, but why — and what the finding means for the patient.
WHY THIS MATTERS
The four procedures in OP2.2 are tested in clinical examinations and encountered in every ophthalmic posting. Bell's phenomenon assessment determines whether ptosis surgery is safe for the cornea. Ptosis evaluation measurements (MRD-1 and levator function) are the objective basis on which surgical technique is selected — without them, a surgeon is guessing. Crigler's massage is taught to parents of infants with nasolacrimal duct obstruction and avoids the need for surgical probing in many cases. Epilation is a simple, often repeated procedure for trichiasis that prevents progressive corneal scarring. As a medical officer in a district hospital or PHC, you may encounter all four of these clinical situations and need to know what to do, or at least when to refer.
RECALL
From Year-1 Anatomy: (1) The levator palpebrae superioris (LPS) arises from the lesser wing of sphenoid, passes above the superior rectus, and inserts via the levator aponeurosis into the upper tarsus and skin (forming the upper lid crease); it is supplied by the superior division of CN III. (2) Müller's muscle (superior tarsal muscle) runs from the underside of LPS to the superior border of the tarsus; it is sympathetically innervated and contributes approximately 2 mm of lid elevation — loss in Horner syndrome produces a mild ptosis of 1–2 mm. (3) The nasolacrimal duct drains from the lacrimal sac (in the lacrimal sac fossa, between the anterior and posterior lacrimal crests) downward to open in the inferior meatus of the nasal cavity at the valve of Hasner. (4) Trichiasis = misdirected eyelashes rubbing the cornea; causes include trachoma, cicatricial entropion, and chronic blepharitis.
Clinical Indication and Relevance of These Four Procedures
Each of the four procedures in OP2.2 addresses a specific clinical problem and generates objective information that changes patient management. Understanding the indication for each procedure prevents both under-use (missing a diagnosis) and over-use (performing a procedure without clinical purpose).
Bell's phenomenon test is indicated before any lid surgery — particularly ptosis correction — to assess the protective globe rotation reflex. A positive Bell's phenomenon means the globe rotates upward and outward on attempted eye closure, protecting the corneal visual axis even if the lid cannot close completely. A negative or poor Bell's phenomenon means the cornea will be directly exposed if the ptosis is over-corrected (lid raised too high), creating a severe post-operative exposure keratopathy. It is also relevant in patients with lagophthalmos from any cause and in those being assessed for corneal exposure risk.
Ptosis evaluation (MRD-1, levator function, lid crease) is indicated in any patient presenting with drooping of the upper eyelid. In children, urgent assessment is needed to detect amblyogenic ptosis — if the drooping lid covers the visual axis, amblyopia develops rapidly. The measurements determine the severity, the likely aetiology (myogenic, aponeurotic, neurogenic, mechanical), and the choice of surgical repair. This is not an examination you can do by 'eyeballing' — objective measurements in millimetres are mandatory for surgical planning.
Lacrimal sac massage (Crigler's massage) is indicated in congenital nasolacrimal duct obstruction (CNLDO) — the commonest cause of watering eyes in infants — as the first-line non-surgical treatment. The procedure is taught to the parents to perform at home 4–6 times daily. Its purpose is to build hydrostatic pressure in the lacrimal sac and force the obstructing Hasner's membrane open at the lower end of the nasolacrimal duct. It is appropriate from birth to approximately 12 months of age, after which probing under general anaesthesia is performed if massage has failed.
Epilation is indicated for trichiasis — inward misdirection of otherwise normally situated eyelashes — when the number of affected lashes is small and permanent ablation is not yet warranted, or as a temporising measure. It is a simple outpatient procedure using epilating forceps to extract individual misdirected lashes under the slit-lamp, performed as often as required (typically every 4–6 weeks as lashes regrow). For definitive permanent removal of larger numbers of lashes, electrolysis (radiofrequency-guided needle electrolysis) or cryotherapy to the lid margin is used.
Bell's Phenomenon: Anatomy, Assessment and Clinical Significance
Bell's phenomenon is a normal physiological reflex in which the eye rotates upward and outward when the eyelids are forcibly closed. This reflex is protective — when the lids close, the cornea is carried upward behind the upper lid, so that any incomplete lid closure exposes only the inferior sclera and not the visual axis cornea. The reflex is present in approximately 80–85% of individuals; in the remaining 15–20% it is absent or equivocal (the globe does not rotate significantly on attempted closure).
The neural pathway underlying Bell's phenomenon is not fully characterised but involves brainstem circuits linking the orbicularis oculi motor nucleus (facial nerve nucleus) with the superior rectus and inferior oblique motor nuclei (oculomotor nucleus). It is distinct from voluntary upgaze and is not under voluntary control — this is why it occurs even in an unconscious or anaesthetised patient.
From a clinical examination standpoint, the grading of Bell's phenomenon is: positive — globe rotates clearly upward and outward on forcible closure (protective; normal); equivocal — partial rotation only; negative — no rotation, the cornea remains in place (high-risk for exposure). In patients with lagophthalmos (e.g., after Bell's palsy), a positive Bell's phenomenon means the cornea is protected despite incomplete lid closure, so exposure keratopathy tends to affect only the inferior cornea. A patient with lagophthalmos and negative Bell's phenomenon has fully exposed cornea on every attempted blink — this is a corneal emergency.
Ptosis Evaluation: MRD-1, Levator Function and Lid Crease Measurement
Ptosis evaluation requires a standardised set of measurements taken under consistent conditions (room illumination, patient in primary gaze, brow relaxed/neutralised). These measurements are analogous to the ECG in cardiology — objective, reproducible, and directly linked to clinical decisions. The three key measurements are MRD-1, levator function, and upper lid crease height.
Margin-reflex distance 1 (MRD-1) is measured from the corneal light reflex (produced by a pen torch held in front of the patient) to the centre of the upper lid margin in primary gaze. In a normal adult, MRD-1 is 4–5 mm. A reduced MRD-1 indicates ptosis: mild ptosis = MRD-1 of 3 mm (1–2 mm below normal); moderate = 2 mm; severe = 1 mm or less. In ptosis with amblyopia risk in children, an MRD-1 of ≤2 mm with the lid threatening the visual axis requires urgent surgery regardless of age.
Levator function (LF) measures the excursion of the upper lid from full downgaze to full upgaze, with the examiner's thumb placed firmly on the brow to block frontalis muscle contribution (otherwise frontalis mimics levator function). The normal LF is ≥15 mm. By convention: poor LF = <4 mm (indicates severe myogenic ptosis — levator muscle is fibrotic or absent; requires frontalis suspension sling surgery); fair LF = 5–11 mm (levator resection or Fasanella-Servat procedure); good LF = ≥12 mm with MRD-1 reduction suggests aponeurotic ptosis (levator aponeurosis dehiscence, the commonest cause in elderly patients — levator re-attachment surgery).
Upper lid crease height is measured from the lid margin to the lid crease (where the aponeurosis inserts into skin). The normal crease is 8–10 mm above the margin in women and 6–8 mm in men. An absent or high crease with good levator function strongly suggests aponeurotic disinsertion. Absence of a crease in a child with severe ptosis suggests congenital myogenic ptosis.
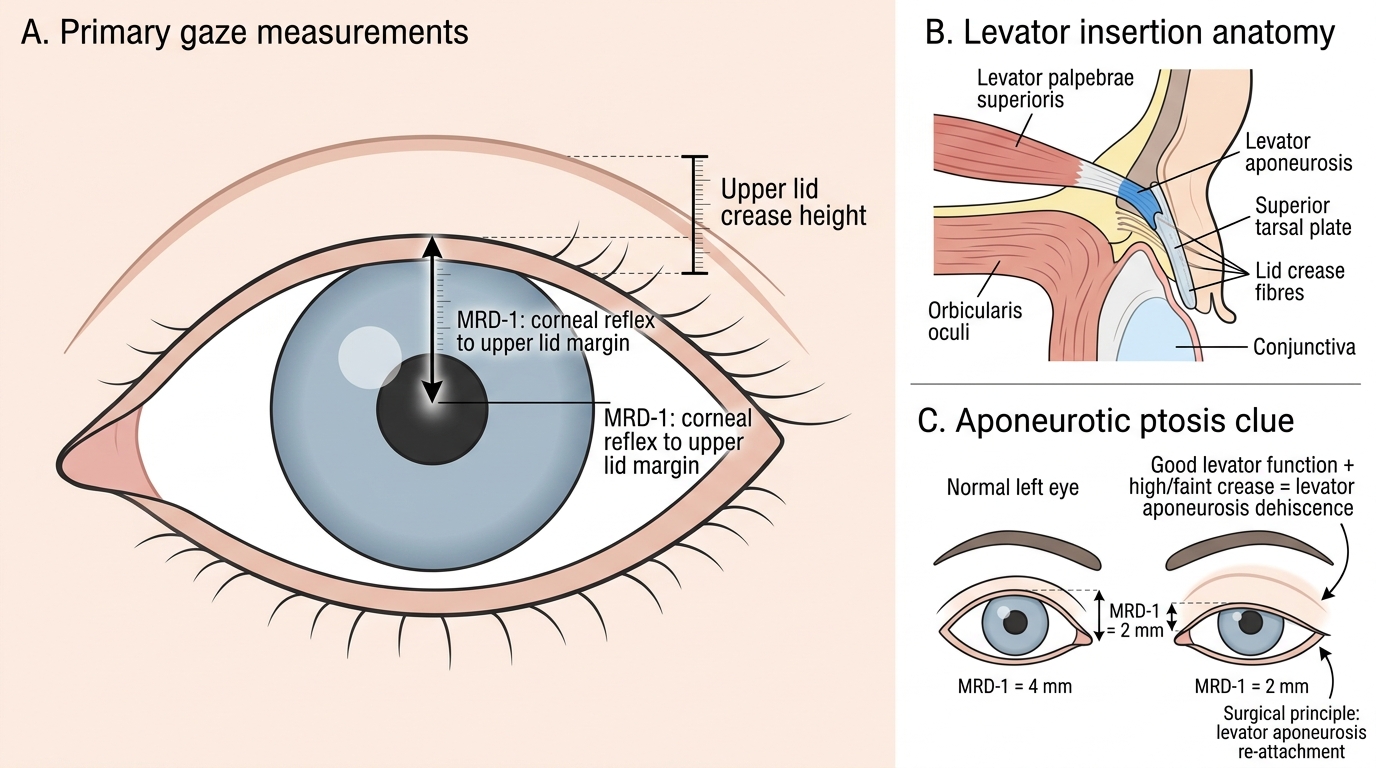
Upper Eyelid Measurements and Levator Aponeurosis Insertion
SELF-CHECK
A 45-year-old woman has drooping of the right upper eyelid. MRD-1 right = 2 mm (left = 4 mm). On levator function testing with the brow neutralised, the excursion of the right upper lid from full downgaze to full upgaze is 14 mm. The upper lid crease is high and faint. What is the most likely diagnosis and recommended surgical approach?
A. Congenital myogenic ptosis — frontalis suspension sling
B. Aponeurotic ptosis (levator dehiscence) — levator aponeurosis re-attachment
C. Neurogenic ptosis (CN III palsy) — levator resection
D. Mechanical ptosis (lid mass) — excision of mass only
Reveal Answer
Answer: B. Aponeurotic ptosis (levator dehiscence) — levator aponeurosis re-attachment
Good levator function (≥12 mm = good LF range; 14 mm is well within this) combined with a high or absent lid crease and moderate ptosis (MRD-1 = 2 mm) is the classic profile of aponeurotic ptosis — dehiscence or disinsertion of the levator aponeurosis from the tarsus. This is the commonest cause of acquired ptosis in adults. The levator muscle itself is functionally intact, so surgery is re-attachment of the aponeurosis. Frontalis sling is reserved for poor LF (<4 mm). CN III palsy also causes ptosis but with additional EOM deficits; mechanical ptosis would require a visible lid mass.