Page 22 of 30
OP2.7-8 | Orbital Tumours: Classification, Presentation, Workup and Referral — SDL Guide
Learning Objectives
- Classify orbital tumours by origin (primary, secondary, metastatic), biological behaviour (benign, malignant), patient age, and tissue of origin
- Describe the clinical presentation of major orbital tumours including capillary haemangioma, dermoid, rhabdomyosarcoma, cavernous haemangioma, optic nerve glioma, optic nerve sheath meningioma, lacrimal gland tumours, orbital lymphoma, and metastases
- Select appropriate investigations for an orbital tumour, including CT and MRI orbit with their specific indications, and systemic workup for lymphoma and metastatic disease
- Explain why incisional biopsy is contraindicated for suspected lacrimal gland pleomorphic adenoma
- Outline the management of major orbital tumours and enumerate the red flag features that indicate urgent referral
INSTRUCTIONS
The orbit contains structures from almost every tissue type — vascular, neural, epithelial, lymphoid, and connective — and tumours can arise in any of them. A systematic classification framework is therefore the clinician's most important tool: it converts an overwhelming list of names into a logical structure that guides clinical assessment, imaging choices, and management decisions. This module takes you through the major orbital tumours systematically, with emphasis on the clinical and imaging features that distinguish them and the management decisions — particularly biopsy choices and referral thresholds — that determine patient outcomes.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. Chapter on Diseases of the Orbit (textbook)
- Parsons' Diseases of the Eye, 23rd ed. Chapter on Orbital Tumours (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Case 1: A 40-year-old woman presents with three years of slowly progressive protrusion of the left eye. There is no pain, no diplopia, and her vision is normal. On examination, the proptosis is axial and non-pulsatile. CT orbit shows a well-defined, ovoid, high-attenuation lesion within the muscle cone with no bony destruction. Case 2: A 6-year-old boy presents with a 2-week history of rapidly progressive proptosis and downward displacement of the right eye, periorbital bruising, and mild pain. He is afebrile. His parents recall a small swelling above the right eye three months ago. CT orbit shows a heterogeneous mass in the superior extraconal space with early bony remodelling. These two patients have entirely different diseases with entirely different urgencies. What distinguishes them, and what does each case require next?
WHY THIS MATTERS
Orbital tumours challenge the clinician at every step: recognition (proptosis is the common entry sign, but its character varies), diagnosis (imaging is essential but must be interpreted correctly), and management (an incision made in the wrong place can seed a benign tumour and convert it to a locally destructive recurrence; an urgent biopsy delayed in a child with rhabdomyosarcoma can cost a life). OP2.7 requires you to classify and describe the presentation of various orbital tumour types; OP2.8 requires you to describe the investigations, management, and indications for referral. Taken together, these competencies equip you to triage an orbital mass correctly in any clinical setting — the outpatient clinic, the emergency department, or the district general hospital.
RECALL
Before proceeding, revisit these foundations from earlier modules:
1. Orbital anatomy (Year-1 Anatomy): The orbit is a bony pyramid of approximately 30 mL volume. The extraocular muscle cone divides it into the intraconal compartment (containing the optic nerve and central orbital fat) and the extraconal compartment (between the muscle cone and the bony walls). Intraconal masses produce axial proptosis; extraconal masses produce eccentric (directional) displacement. The lacrimal gland occupies the superolateral fossa (lacrimal fossa) in the frontal bone.
2. Proptosis evaluation (OP2.6 SDL): Hertel measurement (normal ≤20 mm; asymmetry >2 mm = significant); direction of displacement; reducibility; pulsation; colour vision and visual acuity for compressive optic neuropathy screening.
3. Key differentials already covered: Thyroid eye disease (commonest adult bilateral proptosis, OP2.3); orbital cellulitis (acute proptosis + fever + EOM restriction, OP2.4); cavernous sinus thrombosis (bilateral + systemic signs, OP2.5). This module focuses on true neoplastic orbital disease.
4. Bony anatomy and imaging: CT distinguishes bony erosion (aggressive/malignant) from bony remodelling (pressure effect of slow-growing benign tumour). MRI better characterises soft tissue and optic nerve.
A Lump Behind the Eye: Recognising Orbital Tumours
An orbital tumour is any neoplastic or tumour-like mass arising within the orbit or extending into it from adjacent structures. The clinical presentation is dominated by the consequences of a space-occupying lesion in a rigid bony compartment — but the presenting symptom depends critically on the tumour's location, rate of growth, and biological behaviour.
The most common presenting symptom is proptosis — forward displacement of the globe that the patient or a relative notices. However, several features of the proptosis provide immediate diagnostic information, because orbital tumours are not a homogeneous group — they range from benign hamartomas of childhood (capillary haemangioma) to aggressive malignancies (rhabdomyosarcoma, lacrimal gland adenoid cystic carcinoma) with fundamentally and clinically different urgency of workup and treatment:
- Time course: Slow and painless over months to years suggests a benign lesion (cavernous haemangioma, lacrimal gland pleomorphic adenoma, optic nerve meningioma). Rapid progression over days to weeks, especially in a child, raises the possibility of rhabdomyosarcoma or acute haemorrhage into a lymphangioma. In adults, rapid onset may indicate orbital metastasis, lymphoma, or inflammatory orbital pseudotumour.
- Direction: Axial proptosis (no lateral displacement) indicates an intraconal mass. Eccentric proptosis (globe displaced inferiorly, medially, or laterally) indicates the location of the extraconal mass opposite the direction of displacement.
- Pain: Most benign orbital tumours are painless. Pain is a red flag suggesting malignancy with periosteal invasion, acute inflammatory change, or adenoid cystic carcinoma of the lacrimal gland (characterised by perineural spread and severe pain).
- Diplopia: Extraocular muscle restriction from mass effect, infiltration, or mechanical tethering.
- Visual loss: Compressive optic neuropathy (axial intraconal lesion), optic nerve infiltration (glioma, meningioma), or exposure keratopathy.
The hook cases — the 40-year-old woman with three years of painless axial proptosis and the 6-year-old boy with 2 weeks of rapid eccentric proptosis — represent the two ends of the spectrum. The woman's history and CT are classic for cavernous haemangioma (well-defined intraconal mass, no bony destruction, slow growth). The boy's presentation — rapidly progressive proptosis in a child, eccentric, with bone remodelling — is rhabdomyosarcoma until proved otherwise, a paediatric oncological emergency.
Clinical Presentation by Tumour Type
Each major orbital tumour has a characteristic clinical signature — a combination of age, time course, location, and associated features that, taken together, often allows a clinical diagnosis before imaging. The following descriptions use this clinical signature approach.
Capillary haemangioma: Presents in the first months of life; the commonest orbital vascular tumour of infancy. The lesion is a bright red, lobulated, compressible mass, superficial (in the lid or anterior orbit) or deep. Its critical features are: it enlarges with crying or Valsalva manoeuvre (because increased venous pressure engorges its thin-walled capillaries), and it spontaneously involutes by age 7–10 years. Treatment is indicated only if the lesion threatens vision by causing amblyopia (anisometropic from induced astigmatism, or deprivation from obscuring the visual axis). First-line treatment when required: oral propranolol (β-blocker, causes vasoconstriction and reduced VEGF expression in the haemangioma endothelium).
Dermoid cyst: A congenital choristoma occurring along cranial suture lines — most commonly the frontozygomatic suture (superolateral orbit, most common site) and frontolacrimal suture (superomedial). It presents in childhood as a firm, non-tender, smooth swelling that may not be noticed until school age. It does not transilluminate. The critical clinical hazard is rupture — spontaneous or traumatic — which releases keratin and sebum into the orbit, causing an intense granulomatous inflammatory reaction mimicking orbital cellulitis. Management: elective surgical excision before rupture.
Rhabdomyosarcoma: The commonest primary orbital malignancy in children, typically presenting in the first decade of life. It is a rapidly progressive extraconal mass, most commonly in the superior orbit, causing downward and forward globe displacement with periorbital oedema and sometimes bruising that can mimic trauma or orbital cellulitis. The embryonal subtype is most common in the orbit. Absence of fever does not exclude it. This is the orbital tumour in a child that must NEVER be delayed — a biopsy is required urgently under general anaesthetic.
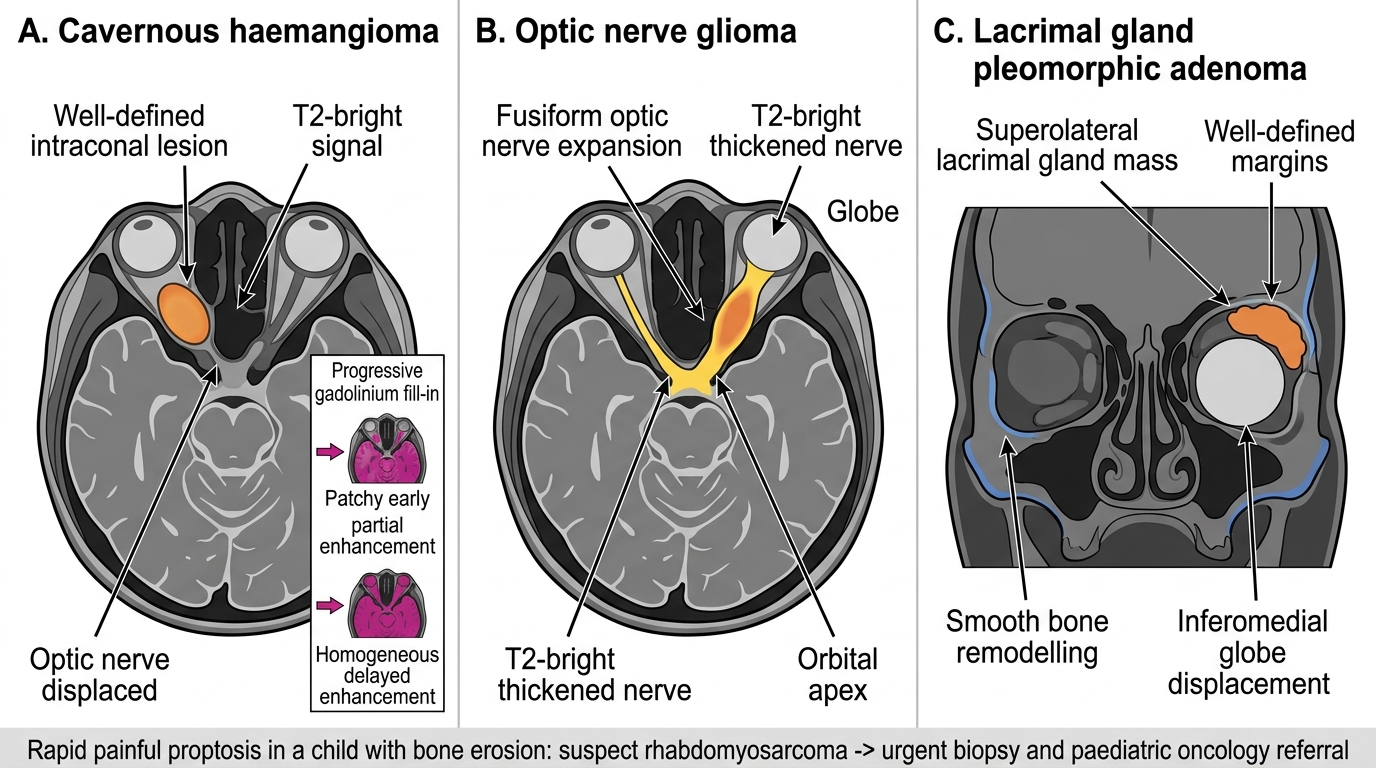
Cavernous haemangioma: The commonest benign orbital tumour in adults. It is a slow-growing, well-encapsulated, intraconal mass, most commonly in the right orbit for reasons that are unexplained. The presenting symptom is axial proptosis progressing over years with no pain. The patient's visual acuity is typically preserved until the mass compresses the optic nerve at the orbital apex. On imaging, MRI shows a T1-isointense, T2-bright, well-defined lesion with characteristic progressive fill-in enhancement on dynamic gadolinium imaging — the most diagnostically useful MRI feature.
Optic nerve glioma: A pilocytic astrocytoma of the optic nerve, predominantly in childhood; approximately 30–50% of childhood orbital optic nerve gliomas are associated with neurofibromatosis type 1 (NF-1). Presents with axial proptosis, relative afferent pupillary defect (RAPD), and visual loss — the combination of axial proptosis and visual field defect strongly suggests an optic nerve lesion. MRI shows fusiform T2-bright expansion of the optic nerve with no sharp nerve-tumour boundary.
Optic nerve sheath meningioma: Arises from the meningeal arachnoid cells sheathing the optic nerve; predominantly in adult women in the 4th–5th decade. Its hallmark presentation is visual loss disproportionate to the degree of proptosis — the meningioma compresses the nerve as it grows, causing progressive optic atrophy before proptosis becomes marked. Optociliary shunt vessels — retinociliary collateral veins visible on fundoscopy at the disc margin — are pathognomonic of chronic optic nerve sheath compression. CT shows 'tram-track' calcification along the nerve; MRI shows circumferential 'tram-track' enhancement around the nerve with gadolinium.
Lacrimal gland tumours: The lacrimal gland in the superolateral orbit produces two clinically distinct presentations:
- Pleomorphic adenoma (benign mixed tumour): Slow-growing (months to years), painless, smooth, non-tender; produces characteristic S-shaped ptosis (the upper lid curves downward at its lateral aspect) and inferomedial globe displacement. CT shows a well-defined mass expanding (remodelling, not eroding) the lacrimal fossa. Incisional biopsy is contraindicated — it seeds the tumour into the orbit and transforms a curable tumour into an incurable, recurrent, eventually malignant lesion. Management: planned total en bloc excision with intact capsule.
- Adenoid cystic carcinoma (malignant lacrimal gland tumour): Presents with onset over months, pain (due to perineural invasion — the pathological hallmark of this tumour), irregular border, and bone erosion on imaging. It is the commonest malignant lacrimal gland tumour and carries a poor prognosis because of its propensity for perineural spread to the cavernous sinus and skull base.
Orbital lymphoma: Almost always B-cell non-Hodgkin lymphoma — the commonest type is extranodal MALT lymphoma (mucosa-associated lymphoid tissue), which is low-grade and may present as a unilateral or bilateral 'salmon-pink' subconjunctival mass that is soft and moulded to the globe. Orbital lymphoma can present in isolation or as part of systemic lymphoma. Systemic staging is always required.
Orbital metastases: Haematogenous spread from a distant primary. Breast is the commonest source in women — notably, scirrhous (fibrotic) breast metastases cause enophthalmos (sunken eye) rather than proptosis, because the fibrotic process actually contracts the orbit. Lung is the commonest source in men. Prostate and kidney are less common in adults. In children, neuroblastoma (adrenal primary) classically metastasises to the orbit, producing bilateral periorbital bruising ('panda eyes' or 'raccoon eyes').
MRI Comparison of Common Orbital Masses
SELF-CHECK
An 8-year-old girl is brought in with 3 weeks of progressive downward and forward proptosis of the left eye. There is periorbital erythema but no fever and no mucopurulent discharge. CT orbit shows an irregular, heterogeneous mass in the superior extraconal space with early erosion of the roof of the orbit. What is the single most urgent management step?
A. Admit for intravenous antibiotics and review in 48 hours
B. MRI orbit and neurosurgery referral next week
C. Urgent incisional biopsy under general anaesthetic and paediatric oncology referral
D. Start oral propranolol and review in 1 month
Reveal Answer
Answer: C. Urgent incisional biopsy under general anaesthetic and paediatric oncology referral
This presentation is rhabdomyosarcoma until proved otherwise — rapidly progressive extraconal proptosis in a child with bone erosion on CT. Rhabdomyosarcoma is the commonest primary orbital malignancy in children. The urgency is because it is a rapidly invasive malignant tumour that responds well to chemotherapy (VAC protocol) + radiotherapy if treated early. Orbital cellulitis typically presents with fever, chemosis, and EOM restriction, but rhabdomyosarcoma can mimic inflammation. Antibiotics alone risk missing the diagnosis. MRI and neurosurgery review 'next week' delays a diagnosis where days matter. Propranolol is for capillary haemangioma (a benign infantile vascular lesion, not this presentation).
Classification of Orbital Tumours
Understanding orbital tumour classification is not a memory exercise — it is the cognitive scaffolding that allows a clinician to generate a differential diagnosis from first principles at the bedside, before CT results are available. The orbit is embryologically complex, incorporating mesenchymal, ectodermal, neural crest, and vascular tissue; each tissue type gives rise to a distinct family of tumours with characteristic clinical behaviour, imaging appearances, and management. Children and adults have fundamentally different orbital tumour spectrums: in children, the most common primary orbital tumour is the capillary haemangioma (benign, involutes spontaneously) but the most feared is rhabdomyosarcoma (rapidly fatal if untreated); in adults, lymphoma and lacrimal gland carcinoma predominate among primary tumours, while metastasis from breast, lung, and prostate is the most common malignant cause overall.
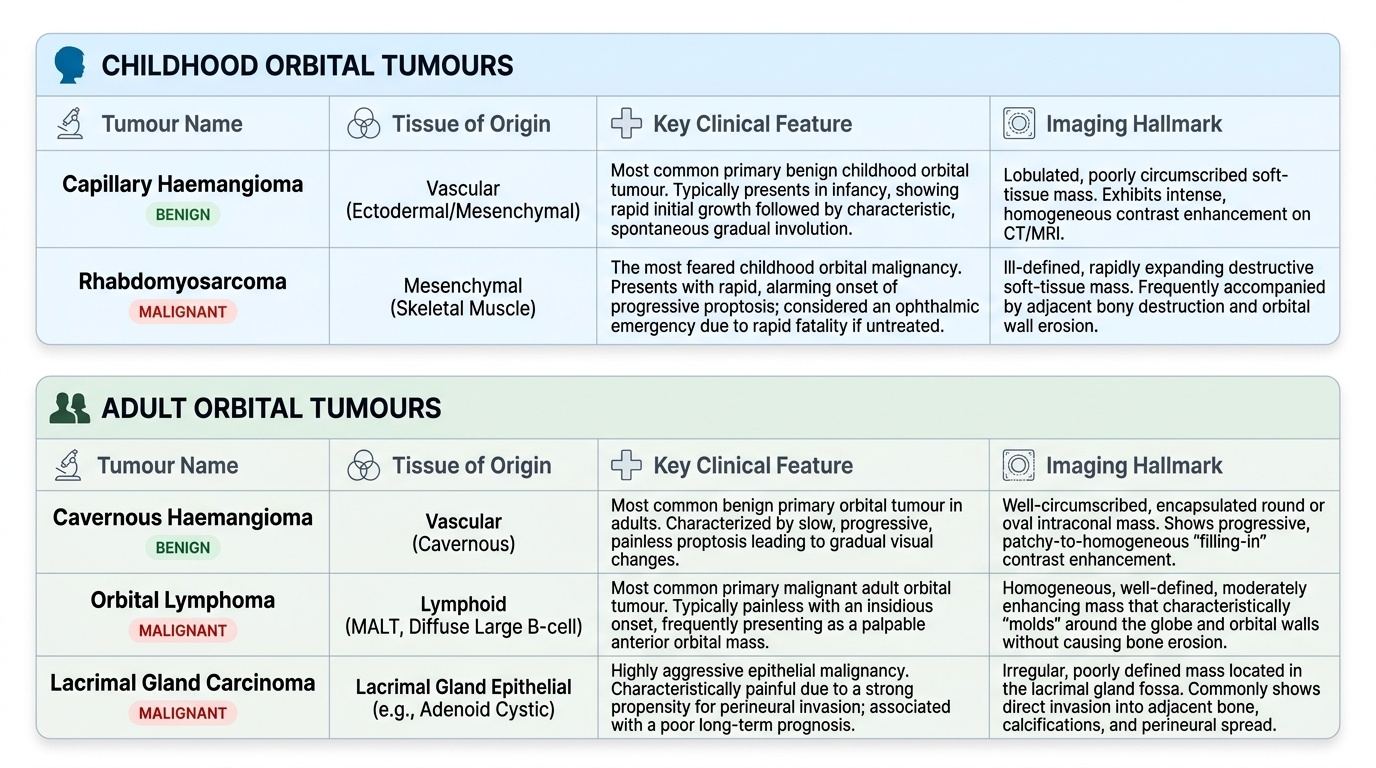
Provided image
A systematic four-axis classification transforms the daunting list of orbital tumour names into a logical structure that guides clinical decision-making.
Axis 1: Origin
- Primary orbital tumours: Arise from tissues native to the orbit. Include the full range of histological types — vascular (capillary haemangioma, cavernous haemangioma, lymphangioma, orbital varices), neural (optic nerve glioma, optic nerve sheath meningioma, schwannoma, neurofibroma), lacrimal gland (pleomorphic adenoma, adenoid cystic carcinoma, other epithelial tumours), lymphoid (orbital lymphoma — MALT, diffuse large B-cell), and mesenchymal (rhabdomyosarcoma, fibrous histiocytoma).
- Secondary orbital tumours (direct extension): Arise outside the orbit and extend into it through bony walls. Sources: sinuses (frontal, ethmoid, maxillary — squamous cell carcinoma, mucocele, adenocarcinoma); eyelids (sebaceous gland carcinoma, squamous cell carcinoma); globe (uveal melanoma through sclera, retinoblastoma).
- Metastatic tumours: Reach the orbit by haematogenous spread. Breast (most common overall, and specifically the commonest source in women), lung (most common in men), prostate, kidney, neuroblastoma (children).
Axis 2: Biological behaviour
- Benign: Well-circumscribed, non-invasive, no bony erosion, remodel rather than destroy bone, slow growth, no distant metastasis. Examples: cavernous haemangioma, dermoid, lacrimal gland pleomorphic adenoma, optic nerve glioma (pilocytic astrocytoma in children = benign histologically).
- Malignant: Infiltrative, bone-eroding, fast-growing, metastatic potential. Examples: rhabdomyosarcoma, adenoid cystic carcinoma, diffuse large B-cell lymphoma, metastases.
Axis 3: Patient age
- Childhood orbital tumours: Capillary haemangioma (infancy), dermoid cyst (childhood), rhabdomyosarcoma (first decade — malignant, urgent), optic nerve glioma (first two decades, NF-1), lymphangioma (childhood), neuroblastoma metastasis (first decade, bilateral periorbital bruising).
- Adult orbital tumours: Cavernous haemangioma (4th–5th decade), lacrimal gland tumours (4th–6th decade), optic nerve sheath meningioma (4th–5th decade, predominately women), orbital lymphoma (5th–7th decade), metastases (5th–7th decade), thyroid eye disease (note: not in this classification as it is not a tumour, but must always be in the adult bilateral proptosis differential).
Axis 4: Tissue of origin — tissue-based grouping
| Tissue type | Benign | Malignant |
|---|---|---|
| Vascular | Capillary haemangioma, cavernous haemangioma, orbital varices | Haemangiopericytoma |
| Neural | Optic nerve glioma (childhood), schwannoma, neurofibroma | Optic nerve sheath meningioma (locally aggressive), malignant peripheral nerve sheath tumour |
| Lacrimal gland | Pleomorphic adenoma | Adenoid cystic carcinoma, mucoepidermoid carcinoma |
| Lymphoid | Benign reactive lymphoid hyperplasia | MALT lymphoma, diffuse large B-cell lymphoma |
| Mesenchymal | Dermoid cyst, fibrous dysplasia | Rhabdomyosarcoma |
| Secondary / metastatic | — | Sinus carcinoma extension, breast/lung/prostate metastases, neuroblastoma (children) |