Page 23 of 30
OP2.7-8 | Orbital Tumours: Classification, Presentation, Workup and Referral — SDL Guide (Part 2)
Pathophysiology: How Orbital Tumours Produce Their Effects
The pathophysiology of orbital tumour effects is largely an exercise in orbital anatomy applied to tumour biology. The orbit is a rigid bony space — unlike the skull, it cannot expand to accommodate a growing mass. Any increase in orbital volume must therefore be displaced anteriorly, pushing the globe forward (proptosis) or, in very small compartments like the optic canal, compressing neural and vascular structures directly.
Volume and compartment effects:
The key determinant of proptosis direction is the tumour's relationship to the muscle cone. Intraconal lesions (within the cone) expand equally in all directions and push the globe straight forward — axial proptosis. Extraconal lesions (outside the cone) are constrained by the bone on one side and push the globe in the direction of least resistance, away from the lesion — eccentric proptosis. This is the anatomical basis of the clinical rule that the direction of eccentric displacement points away from the tumour.
Compressive optic neuropathy:
The optic nerve at the orbital apex is the most vulnerable neural structure. When an intraconal lesion (or a large diffuse lesion) expands at the apex, it compresses the nerve sheath, reducing axoplasmic flow and damaging the parvocellular fibres (which subserve colour vision) before the achromatic channels. The clinical consequence — colour desaturation preceding visual acuity loss — is the single most important monitoring point in any patient with orbital disease. Once compressive optic neuropathy establishes, intervention must be immediate.
Bony changes as diagnostic clues:
The rate of bony change distinguishes benign from malignant behaviour. A slow-growing benign tumour (cavernous haemangioma, pleomorphic adenoma, mucocele) remodels bone — smoothly expanding the bony cavity without cortical destruction, producing a well-defined scalloped margin on CT. A malignant tumour (rhabdomyosarcoma, adenoid cystic carcinoma, metastasis) erodes and destroys bone — producing irregular, moth-eaten bony margins with cortical breakthrough on CT. This CT distinction is one of the most reliable pre-biopsy indicators of malignant behaviour.
Vascular tumour effects:
Vascular orbital lesions have distinctive pathophysiological behaviours based on their haemodynamic properties. Capillary haemangiomas enlarge with increased venous pressure (crying, Valsalva) because their thin-walled capillaries fill with blood when venous outflow is impeded. Cavernous haemangiomas are low-flow lesions with a thick pseudocapsule; they are non-compressible and non-pulsatile. Orbital varices are venous malformations that dramatically engorge with Valsalva (a clinical test: proptosis that markedly increases when the patient strains or bends down = orbital varix). Arteriovenous fistulas (carotid-cavernous fistula) produce pulsatile proptosis with a bruit.
Neural tumour mechanisms:
Optic nerve glioma expands within the nerve itself (fusiform enlargement), directly impairing axonal conduction. Optic nerve sheath meningioma grows around the nerve, compressing it from outside; the nerve remains structurally intact for longer but functionally impaired. Optociliary shunt vessels form at the disc as collaterals to relieve chronic venous obstruction from the surrounding meningioma — they are pathognomonic of chronic optic nerve sheath compression.
Investigations for Orbital Tumours
Investigations for an orbital tumour serve three purposes: to characterise the lesion (imaging), to establish whether the disease is systemic (laboratory and staging), and to achieve tissue diagnosis (biopsy). The choice of investigation is guided by the clinical assessment.
Orbital imaging:
CT orbit and MRI orbit are complementary, not interchangeable. Their relative strengths determine which is chosen first — and choosing the wrong modality first can delay diagnosis by days or provide misleading information. For example, a calcified lesion (optic nerve sheath meningioma, cavernous haemangioma with phleboliths) is identified immediately on CT but may appear only as a non-specific mass on MRI if the characteristic calcification pattern is not appreciated. Conversely, optic nerve infiltration, perineural spread, and intracranial extension are far better characterised on gadolinium-enhanced MRI than on CT. The key rule: when bony detail matters (malignancy with erosion, sinus mucocele, foreign body) — start with CT; when soft tissue characterisation matters (optic nerve lesion, orbital apex, intracranial extension, distinguishing haemangioma from lymphoma) — start with MRI or add it early:
CT orbit (axial and coronal slices):
- Best for bony detail — detects bony erosion (malignant) vs remodelling (benign), sinus mucocele extension, and foreign bodies.
- Detects calcification: phleboliths in cavernous haemangioma; 'tram-track' calcification along the optic nerve in meningioma; eggshell calcification in dermoid.
- Shows the muscle cone boundaries and relationship of the mass to the extraocular muscles.
- Fast; best for acute trauma or uncooperative patients.
- Limitation: poor soft-tissue contrast within the orbit; radiation dose.
MRI orbit (with fat suppression and gadolinium):
- Best for soft-tissue characterisation and optic nerve detail.
- Key T2 signal patterns: high T2 = fluid-containing (lymphangioma, mucocele, lymphoma); moderately high T2 = cavernous haemangioma, dermoid; low T2 = meningioma, dense/cellular lesion.
- Dynamic gadolinium MRI: Progressive fill-in enhancement = cavernous haemangioma (pathognomonic if characteristic). Circumferential 'tram-track' enhancement around the optic nerve = optic nerve sheath meningioma. Early homogeneous enhancement = rhabdomyosarcoma, lymphoma.
- Fusiform expansion of the optic nerve with T2 bright signal = optic nerve glioma.
- No radiation; superior for intracranial extension assessment.
Laboratory investigations:
- TFTs + TRAb: Mandatory in any adult with unexplained proptosis to exclude thyroid eye disease (the great mimic of bilateral orbital disease).
- Full blood count, LDH, serum protein electrophoresis, serum β2-microglobulin: For suspected orbital lymphoma.
- Breast/prostate/kidney tumour markers + CXR/CT chest: If orbital metastasis is suspected.
- Urine catecholamines (VMA, HVA) + MIBG scan: For suspected neuroblastoma in a child.
Systemic staging:
- PET-CT + CT chest/abdomen/pelvis: For lymphoma staging (Ann Arbor system) — orbital lymphoma is Ann Arbor Stage IE if isolated.
- Bone marrow biopsy: Required for lymphoma staging.
Tissue biopsy — the critical decision:
- Incisional biopsy is INDICATED for: rhabdomyosarcoma (urgent), lymphoma (to confirm and subtype), orbital metastasis (to confirm and identify primary), any mass where malignancy cannot be excluded by imaging alone.
- Incisional biopsy is CONTRAINDICATED for: suspected lacrimal gland pleomorphic adenoma. Biopsy seeds tumour cells along the incision track and in the orbit, converting a curable tumour (100% cure rate with en bloc excision) into a locally recurrent and eventually malignant lesion. The correct procedure is total en bloc excision without opening the capsule.
- Excisional biopsy (complete removal) is appropriate for well-encapsulated benign lesions such as cavernous haemangioma and dermoid cyst.
⚑ AI image — pending faculty review (auto-QA score 4/10; best of 3 attempts)
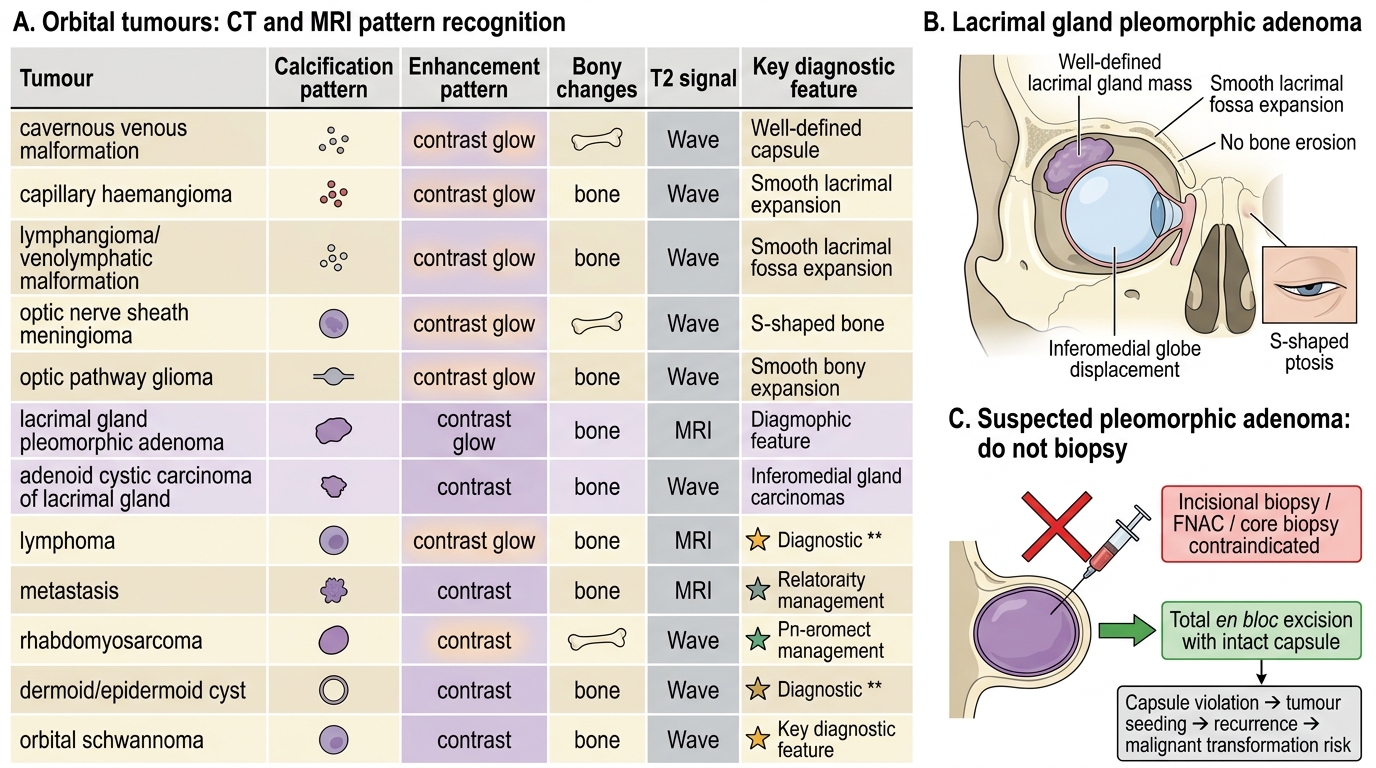
Orbital Tumours: CT-MRI Clues and Pleomorphic Adenoma Management
SELF-CHECK
A 48-year-old woman has a 2-year history of painless, slowly progressive inferomedial displacement of her right globe with S-shaped ptosis. CT orbit shows a well-defined mass in the superolateral orbit that has smoothly expanded the lacrimal fossa without bone erosion. She is referred to you for a 'diagnostic biopsy'. What is the correct management?
A. Proceed with incisional biopsy under local anaesthesia
B. Fine-needle aspiration cytology of the mass
C. Total en bloc excision of the mass with intact capsule, without incisional biopsy
D. CT-guided core needle biopsy
Reveal Answer
Answer: C. Total en bloc excision of the mass with intact capsule, without incisional biopsy
This is the classic presentation of lacrimal gland pleomorphic adenoma — painless, years of duration, S-shaped ptosis, inferomedial globe displacement, well-defined mass with bone remodelling (not erosion) in the lacrimal fossa. Incisional biopsy, fine-needle aspiration, and core needle biopsy are ALL contraindicated for suspected pleomorphic adenoma. Any violation of the capsule seeds tumour cells in the orbit, converting a disease curable by simple en bloc excision (100% cure rate) into a locally aggressive, recurrent, and eventually malignant (carcinoma ex pleomorphic adenoma) lesion. Total en bloc excision with intact capsule through a lateral orbitotomy is the correct first and definitive treatment.
Diagnosis and Differential Diagnosis
Constructing an accurate differential diagnosis for an orbital tumour requires recognising that age is the single most powerful discriminator — the probability distribution of orbital tumours is radically different in a two-year-old versus a sixty-year-old, and applying an adult differential to a child (or vice versa) leads to diagnostic error. Time course is the second axis: a tumour that has been present and stable for three years is almost certainly benign (cavernous haemangioma, dermoid cyst, pleomorphic adenoma); one that has grown visibly over four weeks demands urgent biopsy to exclude rhabdomyosarcoma in children and lymphoma or adenoid cystic carcinoma in adults. Pain is the third discriminator: most benign orbital tumours are painless; lacrimal gland adenoid cystic carcinoma is characteristically painful because of perineural invasion, and lymphoma is painless but produces salmon-coloured chemosis. Applying these three axes in sequence converts a long list of tumour names into three or four prioritised diagnoses.
The differential diagnosis of an orbital tumour is constructed systematically, using patient age as the primary filter, then applying time course, pain, direction of proptosis, and imaging findings to narrow the list.
Step 1: Age filter
If the patient is a child (<16 years):
- Rapidly progressive (<4 weeks): Rhabdomyosarcoma (urgent biopsy), acute haemorrhage into lymphangioma (rapid onset, chocolate-brown fluid if aspirated), orbital cellulitis with abscess (fever, EOM restriction — note: rhabdomyosarcoma can mimic cellulitis).
- Slowly progressive (months): Capillary haemangioma (infancy, Valsalva enlargement, soft, compressible), dermoid cyst (suture line, firm, non-tender), optic nerve glioma (axial, RAPD, visual field loss, NF-1 stigmata).
If the patient is an adult (>40 years):
- Axial, painless, very slow (years): Cavernous haemangioma, optic nerve meningioma (but with early vision loss disproportionate to proptosis + optociliary shunts).
- Superolateral, painless, slow: Lacrimal gland pleomorphic adenoma — DO NOT biopsy.
- Superolateral, painful, with bone erosion: Lacrimal gland adenoid cystic carcinoma — biopsy required, surgical oncology referral.
- Bilateral, soft, salmon-coloured subconjunctival mass: Orbital lymphoma (MALT) — systemic staging mandatory.
- Rapid onset, known primary malignancy: Orbital metastasis. Note scirrhous breast → enophthalmos.
Step 2: Lacrimal gland differential — the most clinically important decision point
Distinguishing pleomorphic adenoma from adenoid cystic carcinoma before any surgical intervention is critical:
| Feature | Pleomorphic adenoma | Adenoid cystic carcinoma |
|---|---|---|
| Duration | Years (>12 months typical) | Months |
| Pain | Absent | Present (perineural invasion) |
| Bone change | Remodelling (smooth expansion) | Erosion (irregular destruction) |
| CT margin | Well-defined, lobulated | Irregular, infiltrative |
| Prognosis | Curable with en bloc excision | Poor (5-year survival ~21%) |
| Biopsy | Contraindicated | Required for diagnosis |
Step 3: Rhabdomyosarcoma vs orbital cellulitis in a child — do not miss this distinction
Both present with acute periorbital swelling and proptosis in a child. The key differentiators: rhabdomyosarcoma typically lacks fever (though low-grade fever may occur), lacks the progressive EOM restriction of cellulitis, and shows a solid mass on CT rather than the rim-enhancing abscess of orbital cellulitis. If there is clinical doubt, urgent CT and ophthalmology/ENT review are mandatory — a missed rhabdomyosarcoma treated as cellulitis is a diagnostic catastrophe.
CLINICAL PEARL
Three biopsy rules for orbital tumours that every clinician must know:
- Never perform incisional biopsy on a suspected lacrimal gland pleomorphic adenoma. The capsule is the barrier between cure and catastrophe — breaching it seeds tumour cells in the orbit and transforms a 100%-curable disease into an incurable local recurrence with malignant transformation risk. The correct approach is total en bloc excision.
- Rhabdomyosarcoma requires urgent biopsy, not observation. Any child with rapidly progressive proptosis and a solid extraconal mass on CT must have an urgent incisional biopsy under general anaesthetic within 24–48 hours. Delayed diagnosis allows haematogenous and lymphatic spread. Localised orbital rhabdomyosarcoma has >90% 5-year survival with VAC chemotherapy; metastatic disease has <30% survival.
- Orbital lymphoma always requires systemic staging. Even an apparently isolated 'salmon-patch' subconjunctival MALT lymphoma may have systemic disease — bone marrow biopsy and PET-CT staging are mandatory before treatment decisions. Managing a systemically active lymphoma with orbital radiotherapy alone would miss the systemic disease.