Page 9 of 30
OP2.3 | Thyroid Eye Disease — SDL Guide
Learning Objectives
- Describe the aetiology and pathophysiology of thyroid eye disease (TED) including the role of TSH receptor antibodies
- Identify the characteristic ocular signs of TED on systematic examination
- Apply the Clinical Activity Score (CAS) and EUGOGO classification to grade disease activity and severity
- Outline the management of TED across severity categories including selenium, IV methylprednisolone, orbital decompression, and rehabilitative surgery
- Recognise and describe the emergency management of sight-threatening TED (compressive optic neuropathy)
INSTRUCTIONS
Thyroid eye disease is the most common cause of unilateral and bilateral proptosis in adults worldwide. It is a systemic autoimmune condition affecting the orbit, and its management requires close collaboration between the ophthalmologist and endocrinologist. This module covers the complete competency OP2.3 — aetiology, clinical presentation, complications, and management — with special attention to the distinction between active and inactive disease, which determines treatment choice. The OP known-trap: do not confuse TED proptosis with orbital cellulitis (OP2.4) or orbital tumour (OP2.6, OP2.7) — this module includes the key differentiating features.
References
- AK Khurana — Comprehensive Ophthalmology, 7th ed., Ch 1 (Thyroid Eye Disease) (textbook)
- Parsons' Diseases of the Eye, 23rd ed., Ch 1 & Ch 16 (Orbital Disease) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 38-year-old woman comes to the ophthalmic OPD referred by her endocrinologist. She was diagnosed with Graves' hyperthyroidism eight months ago and has been on carbimazole. Over the last three months she has noticed that her eyes 'look bigger' and feel gritty, especially in the morning. Her husband says her eyes look like they are 'staring all the time.' On examination you note bilateral upper lid retraction with a visible sliver of sclera above the corneal limbus in primary gaze, bilateral proptosis (Hertel 22 mm right, 20 mm left), and conjunctival injection with chemosis. Her visual acuity is 6/6 bilaterally and colour vision is normal. She tells you she smokes 15 cigarettes a day. You now have to stage her disease, decide whether it is active or inactive, and choose between observation, medical treatment, or referral for orbital surgery. Thyroid eye disease is a diagnosis that requires you to think across organ systems — and act at the right moment.
WHY THIS MATTERS
Thyroid eye disease is the most common cause of adult proptosis in clinical practice. India has a high prevalence of thyroid disorders, and TED is regularly encountered by physicians and ophthalmologists alike. Understanding TED is critical for several reasons: first, the ocular disease can be sight-threatening (from corneal exposure or compressive optic neuropathy) and requires urgent recognition. Second, the severity and activity of TED determine management — applying the wrong treatment at the wrong phase (e.g., operating during the active inflammatory phase) worsens outcomes. Third, systemic factors — particularly smoking and radioiodine therapy — directly worsen TED and are within your influence to address. NMC OP2.3 covers aetiology, clinical presentation, complications, and management.
RECALL
From Year-1 Anatomy: (1) The orbit is a bony pyramid with its apex directed posteriorly toward the optic canal; the orbital volume is approximately 30 mL and is bounded by seven bones. (2) The orbital apex contains the optic canal (optic nerve + ophthalmic artery) and the superior orbital fissure; the annulus of Zinn (common tendinous ring) is the origin of the four rectus muscles and encircles the optic canal — swollen rectus muscles at the apex compress the optic nerve through this tight space. (3) The orbit is lined by periorbita; the pre- and post-septal spaces (relevant to distinguishing TED from orbital cellulitis). (4) From Year-1 Physiology: TSH (thyroid-stimulating hormone) acts on the TSH receptor on thyroid follicular cells; in Graves disease, TRAb (TSH receptor antibodies) constitutively stimulate this receptor. These same TSH receptors are present on orbital fibroblasts — the basis of TED.
Clinical Presentation: Proptosis, Lid Retraction and Red Eye in a Thyroid Patient
Thyroid eye disease presents with a constellation of orbital and periorbital signs that, once recognised, are characteristic. The key is that TED can affect patients who are hyperthyroid, euthyroid, or even hypothyroid — the correlation between thyroid function and eye disease activity is imperfect, and approximately 10% of TED occurs in patients without clinical hyperthyroidism. TED is significantly more common in women (4:1 female-to-male ratio) and in smokers. The onset of TED typically occurs within 18 months of the onset of Graves hyperthyroidism, but disease activity and severity can evolve independently of thyroid hormone levels — this dissociation is why the ophthalmologist and endocrinologist must manage TED collaboratively. Smoking doubles the risk of TED and significantly worsens severity and the response to immunosuppression; smoking cessation is therefore part of the treatment plan, not merely a lifestyle recommendation.
Provided image
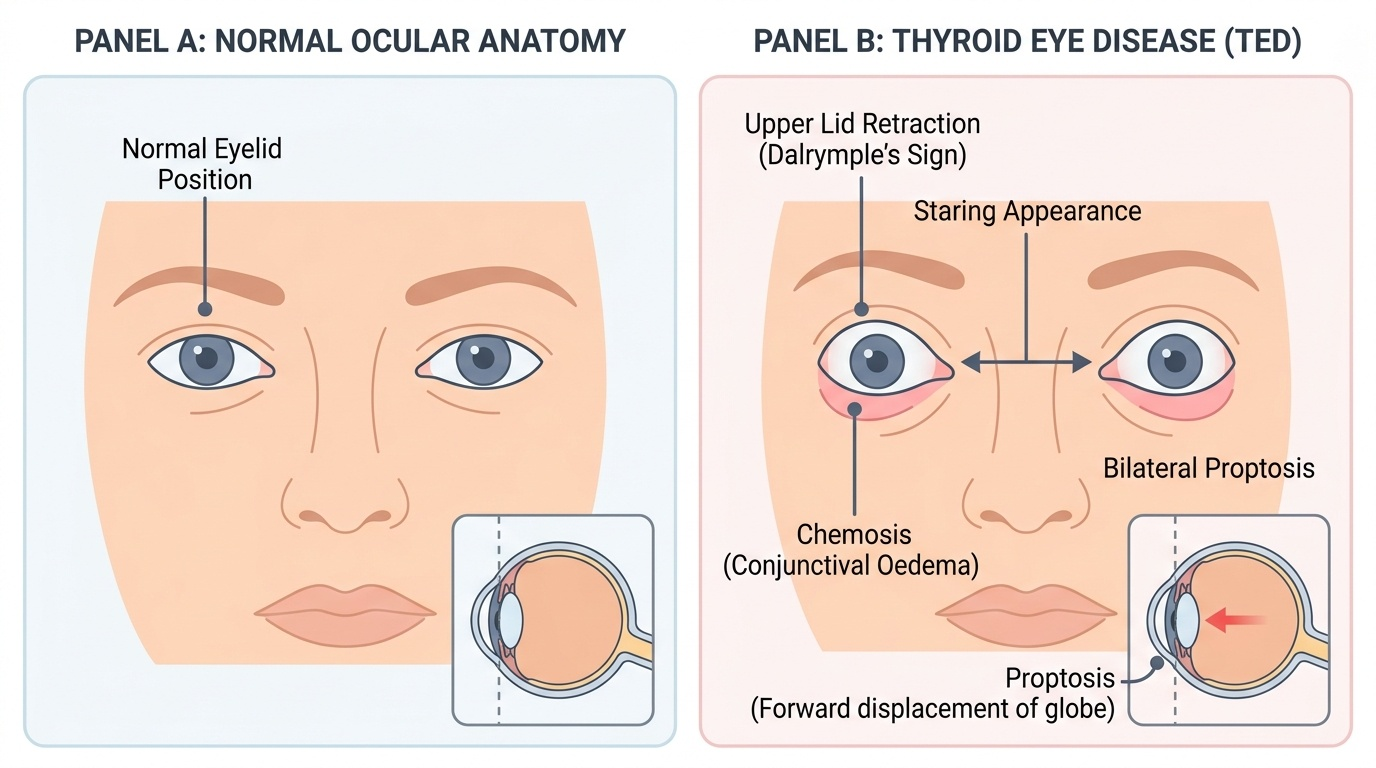
The classical presenting features are:
- Proptosis (exophthalmos): forward displacement of the globe; bilateral in most cases (though often asymmetric); the patient or their family notes the eyes 'look bigger' or 'stick out'
- Upper lid retraction: the upper lid is elevated such that the white sclera (limbus-to-lid gap) is visible above the superior corneal limbus in primary gaze — this is Dalrymple's sign; it gives the characteristic 'staring' or 'frightened' appearance
- Lagophthalmos on attempted closure: due to proptosis pushing the globe forward and lid retraction, the lids cannot fully appose the globe on closure
- Lid lag: the upper lid lags behind the descending globe on downgaze — von Graefe's sign
- Periorbital oedema: puffiness of the lids due to venous congestion and inflammatory oedema
- Chemosis (conjunctival oedema): the conjunctiva balloons forward, appearing as a pale gelatinous fold at the limbus
- Restricted extraocular movements: most commonly inferior rectus fibrosis limits upgaze (patient cannot look up fully) and medial rectus fibrosis limits abduction; double vision (diplopia) is a common symptom
- Corneal exposure: inferior punctate epithelial erosions from inadequate lid closure
- Optic nerve compression (most serious): reduced visual acuity, colour desaturation, relative afferent pupillary defect (RAPD) — occurs due to apical crowding by enlarged rectus muscles
Pathophysiology: Autoimmune Orbital Fibroblast Activation
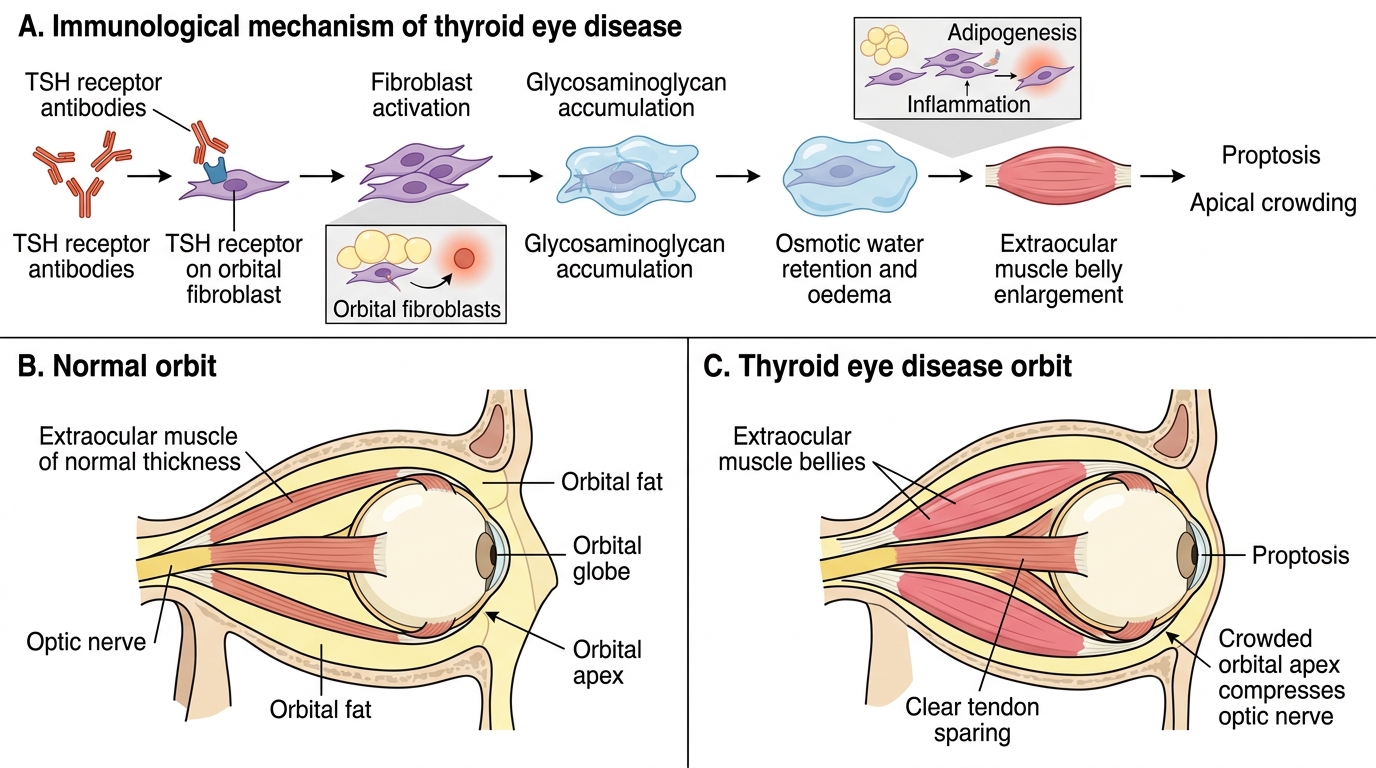
The pathophysiology of TED is an autoimmune process driven by TSH receptor antibodies (TRAb). In Graves' disease, TRAb are produced by activated B lymphocytes and stimulate the TSH receptor on thyroid follicular cells to cause hyperthyroidism. The same TSH receptor is expressed on orbital fibroblasts and preadipocytes within the orbit — when TRAb bind these orbital cells, they stimulate differentiation and proliferation, leading to the three cardinal tissue changes that produce the clinical features of TED.
The three orbital tissue changes are: (1) Glycosaminoglycan accumulation: orbital fibroblasts produce large quantities of hyaluronic acid and chondroitin sulphate, hydrophilic glycosaminoglycans that retain water and cause orbital oedema and expansion — this is the primary cause of proptosis in the early, active (inflammatory) phase of TED. (2) Extraocular muscle enlargement: the EOM belly (muscle body) enlarges from infiltration by lymphocytes, mast cells, and fibroblast-derived glycosaminoglycans; importantly, in TED, the muscle belly is enlarged but the tendon is SPARED — this finding on CT/MRI distinguishes TED from orbital myositis (where both muscle and tendon enlarge). (3) Orbital fat expansion: preadipocyte differentiation into mature adipocytes causes an increase in orbital fat volume, contributing to proptosis and filling the retrobulbar space.
As the disease becomes chronic (inactive phase), the inflammatory infiltrate is replaced by fibrosis and fat, leading to fixed restriction of EOM movements and stable but permanent proptosis. The most dangerous consequence of EOM enlargement is apical crowding at the orbital apex, where swollen muscle bellies compress the optic nerve within the tight confines of the annulus of Zinn and optic canal, causing compressive optic neuropathy even in the absence of extreme proptosis.
Pathophysiology of Thyroid Eye Disease
Ocular Examination: Signs, Grading Systems and Investigation
A systematic ophthalmic examination of a patient with known or suspected TED proceeds in a defined sequence, because each component contributes either to establishing the diagnosis, grading activity, or detecting complications. The clinical examination and scoring are the tools that guide whether to treat or observe, and when to escalate to surgical intervention.

Provided image
Systematic examination sequence: visual acuity (both eyes — critical, as reduced acuity is the earliest warning of optic neuropathy), colour vision (colour desaturation on Ishihara plates is an early sign of optic nerve compression — impaired before VA drops), pupil reactions including RAPD (swinging flashlight test), Hertel exophthalmometry (proptosis in mm), lid position measurements (margin-reflex distance, upper lid crease, lid retraction in mm), assessment of lagophthalmos (ask patient to close eyes slowly and gently — note any gap), EOM assessment (restricted movements, diplopia in the nine positions of gaze), corneal examination (slit-lamp — inferior punctate erosions from exposure), intraocular pressure (IOP may increase on upgaze in TED from IR fibrosis putting pressure on the globe), optic disc assessment (pallor in chronic compressive neuropathy), and visual fields (Humphrey field analyzer for subtle optic nerve defects).
Clinical Activity Score (CAS): The CAS distinguishes active (inflammatory, potentially responsive to immunosuppression) from inactive (fibrotic, not responsive to steroids) disease. It scores 1 point for each of the following 7 features: (1) spontaneous retrobulbar pain at rest; (2) pain on attempted up or side gaze; (3) erythema of the eyelids; (4) oedema of the eyelids; (5) erythema of the conjunctiva; (6) chemosis; (7) oedema of the caruncle or plica semilunaris. CAS ≥3/7 = active disease; CAS <3/7 = inactive. Active disease responds to IV methylprednisolone; inactive disease does not respond and requires rehabilitative surgery.
Hertel exophthalmometry: measures proptosis using a frame that rests on the lateral orbital rims; a mirror system reads the proptosis of each eye separately. Normal upper limits: approximately <21 mm in Caucasians, <20 mm in Asians. An asymmetry of >2 mm between the two eyes is clinically significant even if individual values are within normal limits.
Imaging: CT orbits (axial + coronal, without contrast) is the investigation of choice: it shows enlarged EOM belly with spared tendons (pathognomonic for TED), increased orbital fat, and apical crowding. MRI is used when optic neuropathy is suspected (superior soft-tissue resolution at the apex). Thyroid function tests (TSH, free T4), TRAb, and thyroid ultrasound are ordered in collaboration with the endocrinologist.
SELF-CHECK
A patient with known Graves' disease presents with bilateral proptosis. On examination: visual acuity 6/6 bilaterally, normal colour vision, no RAPD, CAS = 5/7 (spontaneous retrobulbar pain, eyelid oedema, conjunctival erythema, chemosis, caruncle oedema). Hertel: 24 mm right, 22 mm left. What is the correct EUGOGO severity category and what is the first-line treatment?
A. Mild TED — selenium 200 mcg/day for 6 months
B. Moderate-severe active TED — IV methylprednisolone
C. Sight-threatening TED — urgent orbital decompression surgery
D. Inactive TED — rehabilitative surgery (lid, squint, orbital)
Reveal Answer
Answer: B. Moderate-severe active TED — IV methylprednisolone
CAS ≥3/7 (here CAS = 5/7) indicates active inflammatory disease. Vision is preserved (VA 6/6, normal colour vision, no RAPD), so this is not sight-threatening. The degree of proptosis (24/22 mm) and significant inflammatory signs (chemosis, oedema, pain) indicate moderate-severe TED by EUGOGO criteria. The first-line treatment for moderate-severe active TED is IV methylprednisolone (IVMP), which is preferred over oral steroids (better efficacy, fewer systemic side effects per EUGOGO randomised trial data). Selenium is for mild active TED. Rehabilitative surgery is for stable inactive disease.