Page 10 of 30
OP2.3 | Thyroid Eye Disease — SDL Guide (Part 2)
Classification and Diagnosis: EUGOGO Severity and NO SPECS
Two classification systems are used in TED and students must be familiar with both: the EUGOGO (European Group on Graves' Orbitopathy) severity classification and the older NO SPECS mnemonic (still used for clinical description and examinations in many centres). These two systems serve different purposes in practice: EUGOGO guides treatment decisions by stratifying severity into mild, moderate-to-severe, and sight-threatening categories with defined therapeutic thresholds, while NO SPECS provides a structured descriptive vocabulary for documenting the clinical findings at the bedside. Knowing both systems is essential because EUGOGO is the framework used in modern clinical trials and referral criteria, whereas NO SPECS terminology appears in older textbooks, many Indian university examinations, and case-based discussions. The sight-threatening category in EUGOGO requires immediate intervention — dysthyroid optic neuropathy (DON) and corneal breakdown are ophthalmological emergencies.
EUGOGO severity classification is based on the impact of disease on quality of life and threat to vision:
- Mild TED: minor lid retraction (<2 mm), mild soft tissue involvement, proptosis <3 mm above normal, transient or no diplopia, corneal exposure that responds to lubricants. Patient distress is present but QoL impact is limited.
- Moderate-severe TED: ≥2 mm lid retraction, moderate-severe soft tissue involvement, proptosis ≥3 mm above normal, intermittent or constant diplopia, significant corneal exposure. High QoL impact but no immediate visual threat.
- Sight-threatening TED: compressive optic neuropathy (reduced VA, colour desaturation, RAPD, field defect) OR corneal breakdown (ulceration unresponsive to lubrication). This is an emergency requiring immediate intervention.
Crucially, activity (CAS) and severity (EUGOGO) are independent axes: a patient can have severe inactive TED (fibrotic, fixed proptosis, stable EOM restriction — not amenable to steroids) or mild active TED (minimal proptosis but CAS=4/7 — should be treated with steroids to prevent progression).
NO SPECS mnemonic (Werner classification):
- No signs or symptoms
- Only signs (lid retraction, Dalrymple's, von Graefe's)
- Soft tissue involvement (oedema, chemosis, injection)
- Proptosis (measured by Hertel)
- Extraocular muscle involvement (restricted movements, diplopia)
- Cornea involvement (exposure keratopathy, ulceration)
- Sight loss (optic nerve compression — visual acuity, fields, colour vision, RAPD)
Differential diagnosis of TED proptosis: The key differentials are orbital cellulitis (fever, rapid onset, painful, restricted EOM, CT shows fat-stranding not muscle enlargement — OP2.4), orbital tumours (unilateral, irregular mass, CT/MRI shows lesion — OP2.7), orbital pseudotumour/idiopathic orbital inflammation (painful, steroid-responsive, but tendon involvement on imaging distinguishes from TED), and carotid-cavernous fistula (pulsatile proptosis, bruit, dilated episcleral vessels).
SELF-CHECK
On CT orbits of a patient with Graves' disease and bilateral proptosis, the radiologist reports 'bilateral enlargement of the inferior and medial rectus muscles with tendon sparing.' What is the significance of tendon sparing in this context?
A. It suggests orbital myositis rather than thyroid eye disease
B. It is pathognomonic of thyroid eye disease — muscle belly enlargement with tendon sparing distinguishes TED from orbital myositis
C. Tendon sparing is irrelevant; TED diagnosis is made on clinical grounds alone
D. It indicates the chronic inactive phase of TED; active TED shows tendon involvement
Reveal Answer
Answer: B. It is pathognomonic of thyroid eye disease — muscle belly enlargement with tendon sparing distinguishes TED from orbital myositis
In thyroid eye disease, the glycosaminoglycan accumulation and inflammatory infiltration affect the extraocular muscle belly but spare the tendon insertions — this 'tendon sparing' pattern on CT/MRI is pathognomonic of TED. In orbital myositis (idiopathic orbital inflammation), both the muscle belly and the tendon are enlarged — this 'tendon-to-tendon' enlargement on imaging is the distinguishing feature. Tendon sparing is a constant feature of TED regardless of disease phase and is used to distinguish it from the major differential diagnosis of orbital myositis.
Management: Systemic, Orbital and Surgical Treatment
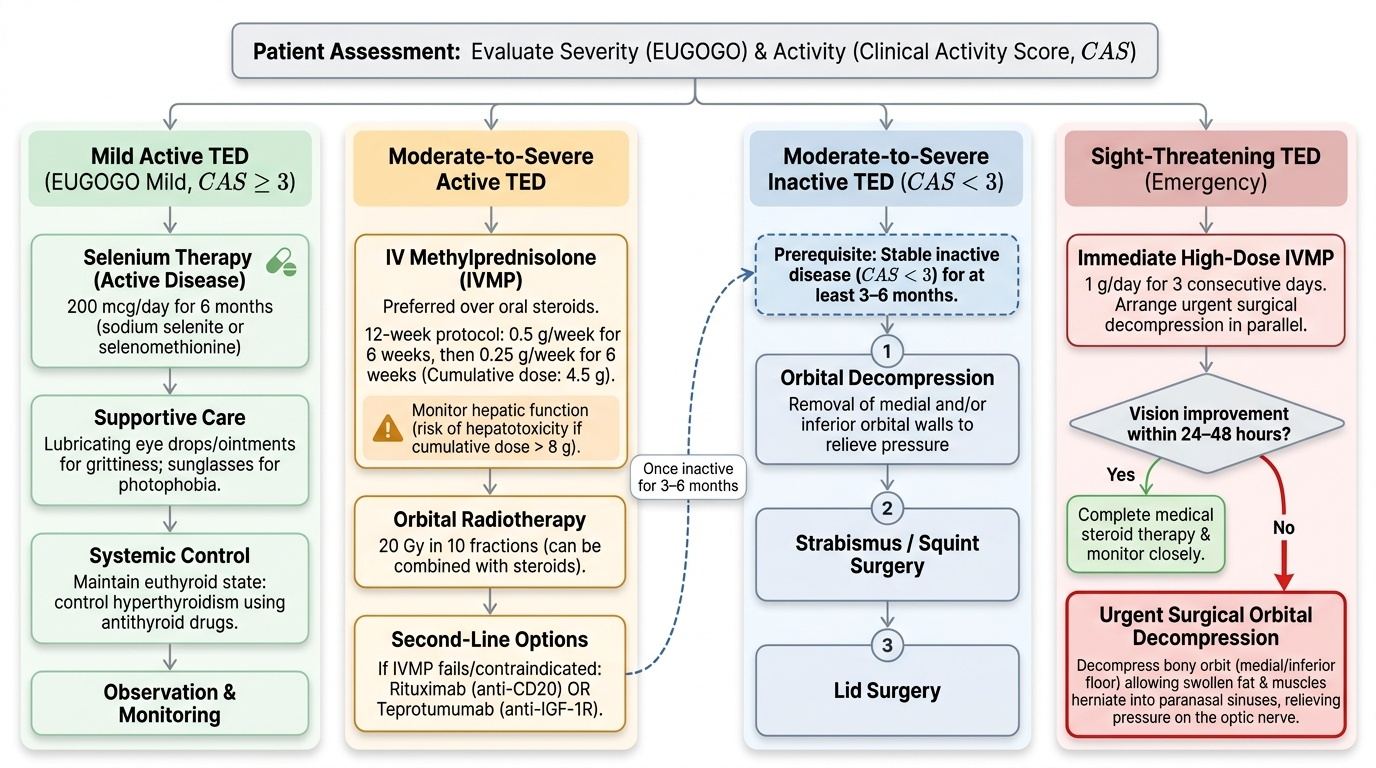
Management of TED is guided by disease activity (CAS) and severity (EUGOGO). The overarching principle is: treat active inflammatory disease with immunosuppression first, and perform rehabilitative surgery only when the disease has been inactive for at least 3–6 months. Operating during the active phase causes unpredictable outcomes because the tissue is still changing. The sequence for rehabilitative surgery (if needed) is: (1) orbital decompression → (2) strabismus/squint surgery → (3) lid surgery — in that order, because each step affects the one that follows.
Provided image
Mild active TED (CAS ≥3, EUGOGO mild): Selenium 200 mcg/day for 6 months (sodium selenite or selenomethionine). Selenium is an antioxidant that reduces the inflammatory burden in orbital fibroblasts; EUGOGO Grade A recommendation, shown to reduce CAS, reduce soft tissue signs, and delay progression to moderate-severe disease. Lubricating eye drops and ointment for gritty symptoms. Sunglasses for photophobia. Euthyroid state is important — control hyperthyroidism with antithyroid drugs.
Moderate-severe active TED (CAS ≥3, EUGOGO moderate-severe): IV methylprednisolone (IVMP) is first-line. Preferred over oral prednisolone because of better efficacy and fewer systemic side effects (EUGOGO randomised trial evidence). Standard EUGOGO protocol: 12 weekly IV infusions of methylprednisolone totalling 4.5 g (e.g., 0.5 g × 6 weeks then 0.25 g × 6 weeks). Hepatic function must be monitored (steroid hepatotoxicity risk — cumulative dose >8 g increases risk). Orbital radiotherapy (20 Gy in 10 fractions) can be combined with steroids for moderate-severe active disease. If steroids fail or are contraindicated, second-line options include rituximab (anti-CD20) or teprotumumab (anti-IGF-1R antibody — FDA-approved for TED).
Sight-threatening TED: Immediately high-dose IVMP (1 g/day for 3 days) while arranging urgent surgical orbital decompression. Compressive optic neuropathy is a surgical emergency. Orbital decompression removes one or more orbital walls (typically medial and/or inferior, or floor) to decompress the bony orbit and allow the swollen orbital fat and muscles to herniate into the paranasal sinuses — this relieves pressure on the optic nerve. If vision does not recover within 24–48 hours of IVMP, decompression should not wait.
Inactive TED (CAS <3): Steroids are ineffective. Management is rehabilitative surgery in the sequence: orbital decompression (if proptosis severe enough to cause corneal exposure or significant cosmetic disability) → strabismus surgery (to correct double vision from fibrotic EOM restriction) → lid surgery (to correct upper lid retraction and lower lid retraction). Each stage must be completed and stable before the next is performed.
Smoking: is the single most important modifiable risk factor for TED. Smokers have 7.7× higher risk of TED than non-smokers. Smoking also reduces the efficacy of orbital radiotherapy. Smoking cessation is mandatory counselling in every TED clinic visit. Radioiodine (RAI) therapy: RAI for Graves' hyperthyroidism can worsen TED (particularly in smokers, pre-existing TED, and high TRAb levels). EUGOGO recommends covering RAI treatment with oral prednisolone 0.3–0.5 mg/kg for 3 months in patients at risk.
Complications and Sight-Threatening Features
Two complications of TED are sight-threatening and constitute ophthalmic emergencies that must be recognised immediately and treated aggressively. Neither condition should be allowed to progress while waiting for an outpatient appointment.
Compressive optic neuropathy (CON): Caused by enlarged rectus muscle bellies crowding the orbital apex and compressing the optic nerve within the tight annulus of Zinn and optic canal. Paradoxically, CON can occur without severe proptosis — the apical crowding is the mechanism, not the proptosis itself, and a patient with minimal proptosis but massively enlarged inferior and medial recti can develop CON. Clinical features: reduced visual acuity (may be subtle initially — compare with pinhole), impaired colour vision (reduced red-green discrimination on Ishihara plates — often the first symptom patients report as 'colours look washed out'), RAPD (relative afferent pupillary defect — a bright torch swung between eyes shows a paradoxical pupil dilation on the affected side because the afferent signal is reduced), and visual field defects (central scotoma or inferior altitudinal defect on Humphrey fields). CT shows apical crowding. Management: immediate high-dose IVMP; if no improvement in 24–48 hours, surgical decompression of the orbital apex.
Corneal breakdown: Severe lagophthalmos from proptosis and lid retraction exposes the cornea, especially inferiorly. The tear film evaporates, epithelium erodes (exposure keratopathy), and if untreated, ulceration develops with risk of perforation and secondary infection. Management: lubricating drops every hour, lubricating ointment at night, moisture chamber glasses, taping the lids at night, and urgent lateral tarsorrhaphy if corneal ulceration is present. Lubricants alone are insufficient for a corneal ulcer — the lid must be closed, either surgically (tarsorrhaphy) or after decompression reduces proptosis.
Both complications require urgent ophthalmology referral and, in the case of CON, immediate intervention without waiting for the endocrinologist's assessment. Vision lost from compressive optic neuropathy may not recover if treatment is delayed beyond 72 hours.
SELF-CHECK
A 52-year-old woman with known TED presents urgently with a three-day history of deteriorating right vision. Examination: right VA = 6/36 (was 6/6 six months ago), Ishihara colour plates 6/17 right (reduced) vs 17/17 left, right RAPD positive, right proptosis 26 mm (Hertel). CAS = 6/7. CT shows enlargement of bilateral inferior and medial rectus muscles with apical crowding on the right. What is the IMMEDIATE treatment?
A. Start selenium 200 mcg/day and review in 6 weeks
B. High-dose IV methylprednisolone 1 g/day for 3 days and urgent surgical orbital decompression if no improvement in 24–48 hours
C. Initiate oral prednisolone 1 mg/kg/day and refer to endocrinologist
D. Arrange elective orbital decompression after stabilising thyroid function
Reveal Answer
Answer: B. High-dose IV methylprednisolone 1 g/day for 3 days and urgent surgical orbital decompression if no improvement in 24–48 hours
This patient has compressive optic neuropathy (CON): reduced VA, impaired colour vision (Ishihara 6/17), positive RAPD, and CT showing apical crowding. This is sight-threatening TED — an emergency. Immediate high-dose IVMP (1 g/day for 3 consecutive days) is given while surgical decompression is arranged. If vision does not improve within 24–48 hours of IVMP, urgent orbital decompression is performed. Selenium is for mild active TED only. Oral steroids are slower and less effective than IV. Waiting for elective surgery or endocrinology review in this setting is inappropriate — every hour of delayed treatment risks permanent visual loss.
CLINICAL PEARL
The most important safety rule in TED management: always check colour vision in every TED patient at every visit. Compressive optic neuropathy causes colour desaturation before visual acuity drops — the patient will often report that colours look 'washed out' or 'less bright' on the affected side before they notice any blurring. Asking 'Do red colours look as bright in your right eye as your left?' takes ten seconds and can detect early optic neuropathy before irreversible damage occurs. A second essential pearl: the CAS and EUGOGO severity are orthogonal — grade both independently at every encounter. A patient who was moderate-severe and active (on IVMP) should be re-graded after treatment; when CAS drops <3 and the disease is inactive, switch to rehabilitative surgery planning, not more steroids.
Self-Assessment: Thyroid Eye Disease
Self-assessment for thyroid eye disease integrates the four domains covered in this module: recognising the clinical presentation, understanding the autoimmune pathophysiology that drives orbital fibroblast activation and glycosaminoglycan deposition, applying the EUGOGO and NO SPECS classification systems to determine severity, and selecting appropriate management — systemic immunosuppression, orbital radiotherapy, surgical decompression, or simply careful monitoring with lubricants. The most examination-relevant scenarios involve correctly identifying sight-threatening TED (dysthyroid optic neuropathy or corneal breakdown) as a medical emergency requiring urgent systemic steroids, distinguishing active from inactive disease using the Clinical Activity Score, and knowing the sequencing of surgical interventions: decompression before squint surgery, squint surgery before lid surgery. Systemic disease control — maintaining euthyroidism — is the essential background condition for all other interventions to succeed.
- A 45-year-old woman with known Graves' disease presents with lid retraction of 3 mm, proptosis of 5 mm above normal, constant diplopia in primary gaze, and a corneal ulcer that has not responded to lubricants. What is her EUGOGO category and what is the immediate treatment?
- What does CAS stand for, and what score threshold defines "active" TED requiring immunosuppression?
- Explain the mechanism by which cigarette smoking worsens TED severity and reduces response to immunosuppression.
- A patient with TED requires decompression, strabismus surgery, and lid retraction correction. In what order must these be performed and why?
- What is the NO SPECS class for the following: marked proptosis with complete limitation of eye movements, worsening colour vision, but no corneal exposure or optic neuropathy yet on formal testing?
Expected answers: (1) Sight-threatening TED (corneal exposure with ulcer); IV methylprednisolone 1 g/day for 3 days, urgent orbital decompression if steroids fail, corneal protection with moisture chamber and topical antibiotics. (2) Clinical Activity Score — each of 7 signs scores 1 point; CAS ≥ 3/7 = active disease; ≥ 4/10 in recurrences. (3) Smoking promotes orbital fibroblast activation, increases adipogenesis and hyaluronic acid synthesis; it also increases anti-TSHR antibodies and reduces efficacy of IV steroids and orbital radiotherapy by approximately 50%. (4) Orbital decompression first (changes eye position and muscle balance) → strabismus surgery second (may further alter lid position) → lid retraction correction last. (5) NO SPECS Class 4 (motility restriction); the patient also has Class 2 (soft tissue involvement) and Class 3 (proptosis) — all three classes are present. Class 5 (corneal) is not yet reached; worsening colour vision raises concern for Class 6 (optic nerve) and mandates urgent formal assessment even if not confirmed on formal testing yet.