Page 4 of 27
OP3.2 | Acute Conjunctivitis: Bacterial and Viral Patterns — SDL Guide
Learning Objectives
- Describe the etiopathogenesis of acute bacterial and viral conjunctivitis
- Distinguish bacterial from viral conjunctivitis on the basis of clinical features and the papillary-versus-follicular reaction
- Identify the causes and management of hyperacute gonococcal conjunctivitis and ophthalmia neonatorum
- Outline the clinical forms of adenoviral conjunctivitis and state the basis of isolation and school-exclusion policies
INSTRUCTIONS
Acute conjunctivitis — inflammation of the conjunctiva arising over hours to days — is the most common cause of the red eye globally, and in most cases it is caused by a bacterium or a virus. Although it is generally self-limiting, some causes (notably Neisseria gonorrhoeae and adenoviral epidemic keratoconjunctivitis) are sight-threatening or highly contagious and require specific management. The ability to clinically distinguish bacterial from viral conjunctivitis — using the character of the discharge and the type of conjunctival reaction on eversion — is a core skill that determines whether you prescribe an antibiotic or give supportive care and hygiene advice.
References
- AK Khurana — Comprehensive Ophthalmology, 7th ed., Ch. 6: Diseases of Conjunctiva (textbook)
- Parsons' Diseases of the Eye, 23rd ed., Ch. 8: Diseases of the Conjunctiva (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A school nurse sends three children from the same class to your clinic on the same morning. All three have red, watery eyes with minimal discharge. Two of them report that the redness started in one eye and then spread to the other. Another child from a different family arrives simultaneously — her eyes are also red but with thick yellow discharge and her mother says her lids were stuck shut this morning. Are these four children infected with the same thing? Should you send them all back to school or exclude some of them? And does any child need a prescription? The answers depend on whether the cause is bacterial or viral — and you must decide by looking at the pattern of the discharge and the conjunctival surface.
WHY THIS MATTERS
Acute conjunctivitis is the commonest ocular diagnosis in outpatient practice across primary care, emergency departments, and ophthalmology clinics worldwide. Studies in the UK suggest that one in three GP consultations for red eye results in a prescription for topical antibiotics — but the majority of these cases are viral and antibiotics confer no benefit while promoting resistance. The NMC competency OP3.2 requires you to be able to describe the etiopathogenesis, clinical features, and treatment of both bacterial and viral conjunctivitis — because the management is fundamentally different. Failing to recognise a hyperacute gonococcal conjunctivitis can result in corneal perforation within 48 hours; failing to isolate a child with epidemic keratoconjunctivitis can trigger an outbreak affecting an entire school or hospital ward.
RECALL
The conjunctiva is a translucent mucous membrane covering the palpebral surface (inside of eyelids) and the bulbar surface (anterior sclera up to the limbus). It is richly vascularised and contains its own lymphoid tissue — the conjunctiva-associated lymphoid tissue (CALT), concentrated especially in the fornices. This lymphoid tissue mounts immune responses to antigens encountered on the conjunctival surface, generating the follicular or papillary reactions you will examine when differentiating conjunctivitis subtypes. The conjunctival epithelium produces goblet cells that secrete mucus; inflammation disrupts this layer, alters tear film, and generates the excessive discharge that is the cardinal symptom of conjunctivitis.
The Red, Sticky Eye — Clinical Presentation of Acute Conjunctivitis
Acute conjunctivitis shares a core set of clinical features regardless of aetiology, which allows you to confirm that you are dealing with conjunctivitis before narrowing to the specific cause. The three cardinal symptoms are redness (conjunctival hyperaemia — often described by patients as the eye looking 'blood-red' or 'pink'), discharge (ranging from watery to frankly purulent, depending on cause), and discomfort (typically gritty or foreign-body sensation, not true deep pain). By definition, uncomplicated conjunctivitis does NOT reduce visual acuity and does NOT cause photophobia — the presence of either should immediately prompt you to reconsider the diagnosis and look for corneal or uveal involvement.
The pattern of spread is diagnostically useful: bacterial conjunctivitis often begins unilaterally and spreads to the second eye within 1–2 days via direct hand contact and self-inoculation; viral conjunctivitis (especially adenoviral) can also be bilateral but often starts unilaterally, and the second eye gets involved later. Bilateral simultaneous onset from the very start is more typical of allergic or toxic conjunctivitis.
On general inspection, the eye shows:
- Conjunctival hyperaemia — most prominent in the fornices and peripheral bulbar conjunctiva (conjunctival injection), sparing the perilimbal area (no ciliary flush).
- Discharge — accumulates in the inner canthus; may glue the lids together at night, causing the classic complaint of 'eyes stuck shut in the morning' in bacterial disease.
- Chemosis — oedema of the bulbar conjunctiva, causing a gelatinous elevation of the conjunctival surface; more pronounced in gonococcal and severe viral disease.
- In viral forms: preauricular lymph node enlargement is a reliable sign — feel for a tender node just anterior to the tragus of the ear.
Conjunctival Anatomy and the Papillary vs Follicular Reaction
The single most important clinical sign for distinguishing bacterial from viral conjunctivitis is the type of conjunctival reaction visible on eversion of the upper eyelid. This requires the examiner to evert the upper lid using a cotton bud or the thumb, exposing the palpebral conjunctival surface, and inspect it under a torch light or slit-lamp. There are two distinct patterns:
Papillary reaction: Papillae are small, flat-topped elevations of the conjunctival surface, each containing a central vascular core that gives them a red dot appearance. The vascular core is fed from below and the epithelium folds over it, creating the characteristic central vessel. Papillae form when inflammatory cells (PMNs, eosinophils) infiltrate the subepithelial stroma around this vascular scaffold. Giant papillae (>1 mm) — 'cobblestone' appearance — are pathognomonic of vernal keratoconjunctivitis on the upper palpebral conjunctiva. A papillary reaction indicates bacterial or allergic stimulation of the conjunctiva.
Follicular reaction: Follicles are dome-shaped, avascular lymphoid aggregates in the subepithelial layer. They have no central vascular core — instead, blood vessels course around the periphery of the follicle ('cap vessels'), giving them a pale, translucent centre with surrounding vessels, like a miniature lymph node. Follicles represent lymphocyte proliferation in response to viral or chlamydial antigens. A follicular reaction on the palpebral conjunctiva indicates viral or chlamydial conjunctivitis.
Memory aid: 'F for Follicle, F for Follicular (viral)' — follicles are round, avascular, and fluffy; papillae are flat-topped, vascular, and present in bacterial/allergic disease.
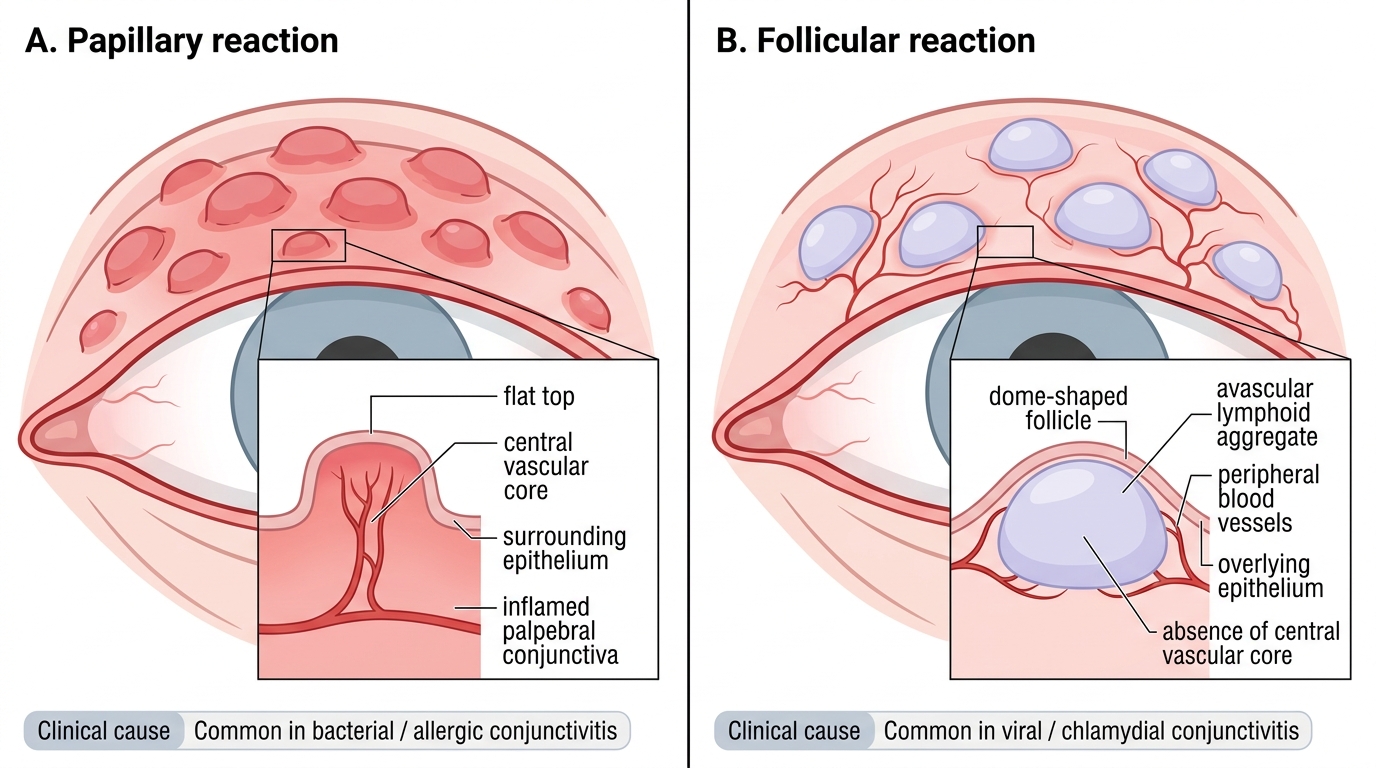
Papillary vs Follicular Conjunctival Reaction
SELF-CHECK
On everting the upper eyelid of a patient with acute red eye, you see dome-shaped pale elevations with blood vessels coursing around their periphery but no central vascular core. This reaction pattern is called:
A. Papillary reaction — indicating bacterial conjunctivitis
B. Follicular reaction — indicating viral or chlamydial conjunctivitis
C. Giant papillary reaction — indicating vernal keratoconjunctivitis
D. Chemosis — indicating allergic response
Reveal Answer
Answer: B. Follicular reaction — indicating viral or chlamydial conjunctivitis
Follicles are dome-shaped, avascular lymphoid aggregates — they have no central vascular core; blood vessels run around the periphery. This pattern is produced by lymphocyte proliferation in response to viral or chlamydial antigens. Papillae, by contrast, have a central vascular core and a flat top, and indicate bacterial or allergic stimulation. The follicular-vs-papillary distinction is the key clinical sign for aetiology in acute conjunctivitis.
Examining the Conjunctiva and Diagnosing the Cause
A systematic clinical examination of acute conjunctivitis proceeds in a fixed sequence that ensures no discriminating feature is missed. The examination should be performed in a well-lit room using a torch; a slit-lamp adds precision but is not required for the basic assessment.
Step 1 — Visual acuity: Test both eyes. Any reduction in VA in a 'red eye' diagnosis is a red flag for corneal or uveal involvement — reassess the diagnosis.
Step 2 — Inspect the discharge: Look at the inner canthus and lids. Characterise as: watery/serous (viral or allergic), mucopurulent (yellow, thick — bacterial), purulent/profuse (gonococcal or severe bacterial), or ropy/stringy (allergic/vernal).
Step 3 — Inspect the bulbar conjunctiva: Note the pattern of redness — conjunctival injection (prominent peripherally) or ciliary flush (perilimbal). In conjunctivitis, you should see only conjunctival injection. Any perilimbal flush suggests corneal or uveal pathology.
Step 4 — Evert the upper eyelid: Ask the patient to look down. Place a cotton bud at the upper tarsal border. Fold the lid upward over the bud. Inspect the palpebral conjunctiva for follicles (viral), papillae (bacterial/allergic), or giant papillae (vernal).
Step 5 — Inspect the cornea: Use oblique illumination. Any haziness, ulcer, or staining (with fluorescein under cobalt-blue light) indicates keratitis — a completely different diagnosis requiring urgent specialist referral.
Step 6 — Palpate the preauricular node: Tenderness of the preauricular lymph node (just anterior to the tragus) strongly favours viral aetiology, especially adenoviral conjunctivitis. It is absent in bacterial disease.
Step 7 — Examine fellow eye: Bilateral symmetric involvement supports viral or allergic cause; sequential unilateral spread suggests infectious (bacterial or viral) spread.
IMPORTANT: If the discharge is profuse and purulent and you cannot wipe it away — it immediately reforms — suspect hyperacute (gonococcal) conjunctivitis and treat as an emergency.