Page 5 of 27
OP3.2 | Acute Conjunctivitis: Bacterial and Viral Patterns — SDL Guide (Part 2)
Bacterial Conjunctivitis: Causes, Features, and Treatment
Bacterial conjunctivitis is characterised by mucopurulent discharge, papillary reaction on the palpebral conjunctiva, and the absence of a preauricular node. The spectrum of causative organisms determines the severity and dictates the management strategy. Understanding the causative agent is particularly important because common organisms cause a self-limiting disease manageable with topical antibiotics, while Neisseria gonorrhoeae causes a hyperacute emergency requiring systemic treatment. This understanding also prevents the common error of treating all mucopurulent conjunctivitis as equivalent — the clinical approach to Staphylococcal lid disease differs fundamentally from that to gonococcal conjunctivitis, not only in drug choice but in urgency: one can be managed in the community over a week, the other requires same-day systemic antibiotics to prevent corneal perforation. The management algorithm for neonatal conjunctivitis depends critically on the time of onset after birth, which serves as a reliable surrogate for the causative organism. A clinician who understands the organism-specific reasoning behind each treatment choice will never default to 'topical chloramphenicol for any red sticky eye.'
Provided image
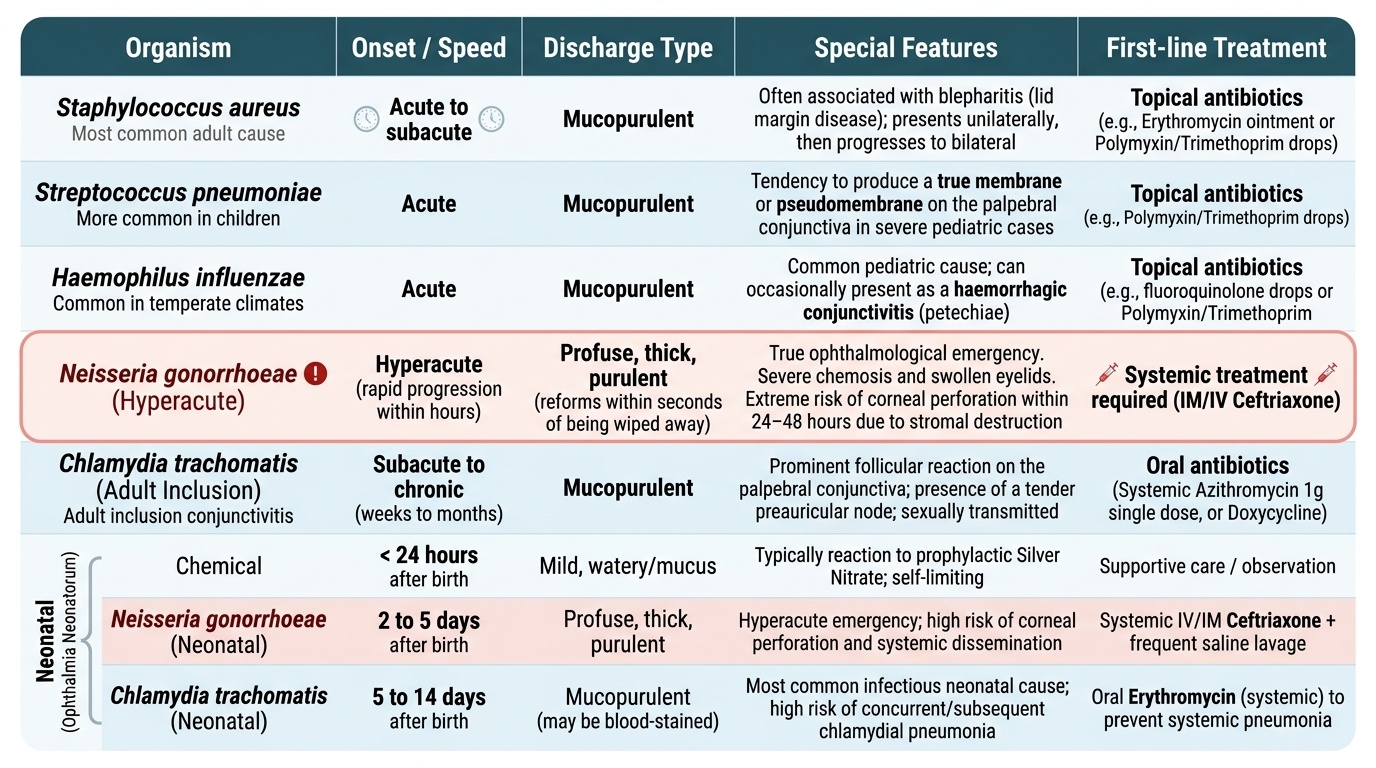
Common bacterial causes in adults (non-hyperacute):
- Staphylococcus aureus — most common cause of bacterial conjunctivitis in adults; presents as an acute to subacute unilateral then bilateral mucopurulent conjunctivitis; often associated with blepharitis (lid margin disease).
- Streptococcus pneumoniae — more common in children; tends to produce a membrane or pseudomembrane on the palpebral conjunctiva in severe cases.
- Haemophilus influenzae — common cause of bacterial conjunctivitis in children, particularly in temperate climates; can cause a haemorrhagic conjunctivitis.
Hyperacute bacterial conjunctivitis — Neisseria gonorrhoeae:
Gonococcal conjunctivitis is a true ophthalmological emergency. The discharge is profuse, thick, and frankly purulent — it reforms within seconds of being wiped away. The conjunctiva is intensely hyperaemic, with severe chemosis, and the eyelids are markedly swollen. Without urgent systemic treatment (IM or IV ceftriaxone), the gonococcal lipopolysaccharide (LPS) destroys the corneal stroma, leading to corneal perforation within 24–48 hours — a blinding complication. Topical antibiotics alone are INSUFFICIENT for gonococcal disease. The patient must also be investigated for genital co-infection and sexual contacts traced.
Ophthalmia neonatorum (neonatal conjunctivitis):
Neonatal conjunctivitis presents within the first 4 weeks of life and is acquired during passage through an infected birth canal. The timing of onset provides the critical clue to aetiology:
- Day 1–3: Chemical conjunctivitis (from silver nitrate prophylaxis — now largely replaced) OR Neisseria gonorrhoeae (if onset <5 days, always consider gonococcal first).
- Day 5–14: Chlamydia trachomatis serotypes D-K (inclusion conjunctivitis) — the most common cause of neonatal conjunctivitis in many settings; causes a follicular/papillary mixed reaction with mucopurulent discharge; treated with systemic erythromycin (topical alone is insufficient as it does not treat concomitant chlamydial nasopharyngeal infection in the neonate).
- Any neonate with purulent conjunctivitis at any age should have cultures taken immediately.
WHO recommends prophylaxis with 1% tetracycline ointment or 0.5% erythromycin eye ointment at birth in endemic areas.
Treatment of non-gonococcal bacterial conjunctivitis:
Most cases are self-limiting in 7–10 days even without treatment. Topical antibiotics reduce the duration by 1–2 days and decrease infectivity:
- First-line: topical chloramphenicol (0.5% drops or 1% ointment) or topical ciprofloxacin (0.3%) — both 4× daily for 7 days.
- In contact-lens wearers, avoid chloramphenicol; use fluoroquinolones (ciprofloxacin or ofloxacin).
- Hygiene measures: clean hands, do not share towels, discard contaminated contact lenses.
SELF-CHECK
A 5-day-old neonate is brought to the paediatric clinic with bilateral mucopurulent eye discharge since birth. Gram stain of the discharge shows Gram-negative intracellular diplococci. The correct management is:
A. Topical chloramphenicol eye drops for 7 days
B. Systemic ceftriaxone plus topical saline irrigation
C. Topical erythromycin ointment alone
D. Topical ciprofloxacin drops for 5 days
Reveal Answer
Answer: B. Systemic ceftriaxone plus topical saline irrigation
Gram-negative intracellular diplococci on conjunctival smear in a neonate = Neisseria gonorrhoeae — a sight-threatening emergency. Treatment requires systemic ceftriaxone (single IM dose, weight-based) because topical antibiotics alone cannot achieve adequate concentrations to prevent corneal perforation. Frequent saline irrigation removes the purulent exudate and reduces the gonococcal load. Topical antibiotics are used as an adjunct but never as monotherapy. If untreated, corneal perforation can occur within 24-48 hours.
Viral Conjunctivitis: Adenoviral EKC and Acute Haemorrhagic Conjunctivitis
Viral conjunctivitis is the most common cause of infectious conjunctivitis globally, with adenovirus accounting for the vast majority of cases. Unlike bacterial conjunctivitis, viral disease is almost entirely self-limiting — antibiotics play no role — but certain forms are so contagious that they require strict infection control measures including school and workplace exclusion. The clinical stakes are therefore not in the severity of the individual illness but in the public health consequences of mismanagement: a nurse with EKC who continues working on an ophthalmic ward can trigger an outbreak affecting dozens of patients. Understanding the virological distinctions between pharyngoconjunctival fever and epidemic keratoconjunctivitis — in particular the serotype-specific risk of subepithelial corneal infiltrates in EKC — is essential for giving the patient accurate prognostic information and the clinic accurate infection control advice. The specific timing of subepithelial infiltrate development in EKC (second week of illness) is a commonly tested factual point and a clinically critical one, because patients who are not warned return with blurred vision that they attribute incorrectly to a new diagnosis.
Provided image
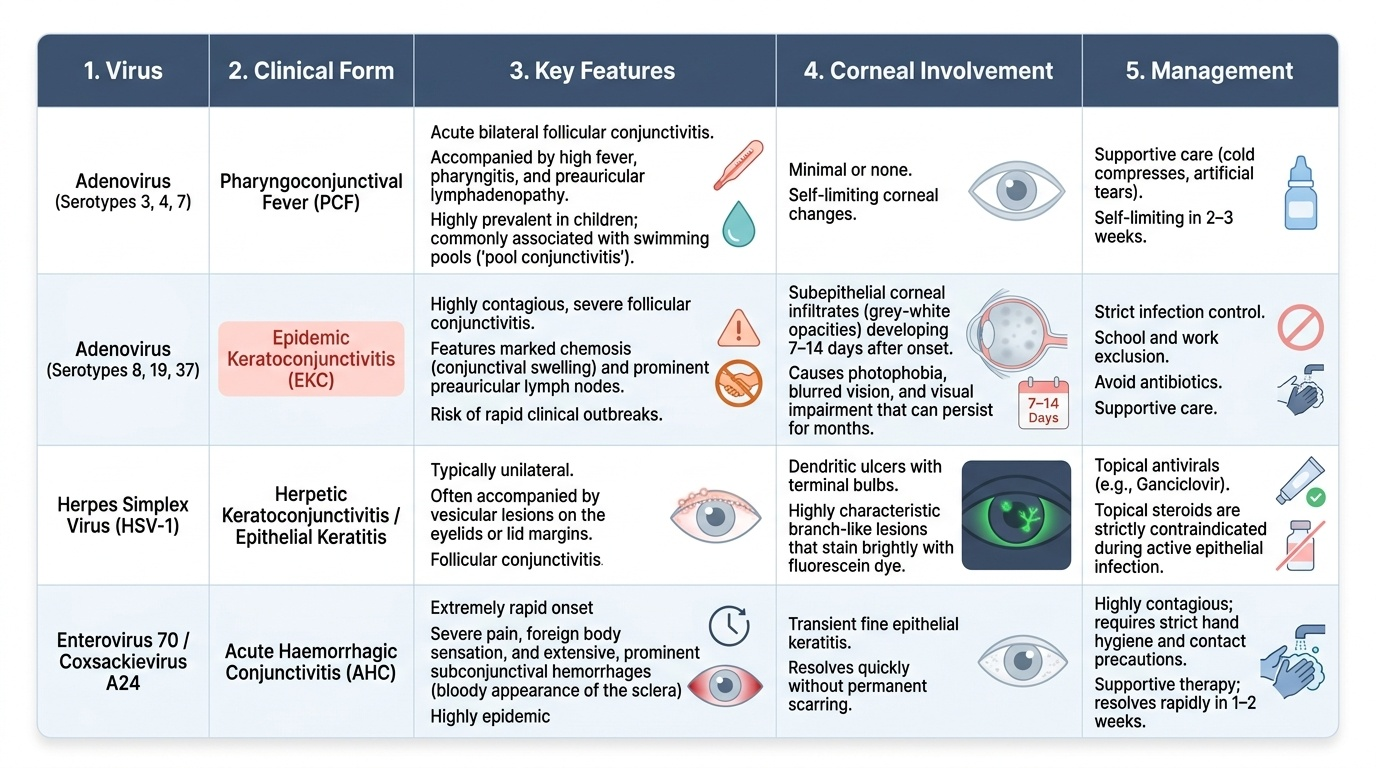
Adenoviral conjunctivitis:
Adenovirus causes two main clinical syndromes based on the serotype:
- Pharyngoconjunctival fever (PCF) — caused by adenovirus types 3, 4, and 7. Presents as an acute bilateral follicular conjunctivitis with prominent fever, pharyngitis, and preauricular lymphadenopathy — hence the name. Corneal involvement is minimal. Typically affects children in epidemics, often in relation to swimming pools ('pool conjunctivitis'). Self-limiting in 2–3 weeks.
- Epidemic keratoconjunctivitis (EKC) — caused by adenovirus types 8, 19, and 37. This is the more severe and more contagious form. Initial conjunctivitis (follicular, with marked chemosis and preauricular node) is followed after approximately 7–14 days by subepithelial corneal infiltrates — grey-white opacities beneath the corneal epithelium that cause photophobia, blurred vision, and prolonged visual impairment. These infiltrates may persist for several months and can cause significant morbidity in health workers (EKC outbreaks in ophthalmic clinics are well documented). The conjunctivitis itself is highly contagious — a single touch from an infected surface to the eye is sufficient. EKC patients must be excluded from work/school and ophthalmology clinics for at least 2 weeks.
Management of adenoviral conjunctivitis:
Treatment is supportive: cold compresses, lubricant drops, hygiene measures. Topical steroids are sometimes used for the subepithelial infiltrates of EKC but must only be prescribed by an ophthalmologist (they can reactivate the infiltrates when weaned). There is NO licensed antiviral for adenoviral conjunctivitis. Topical antibiotics are inappropriate and should NOT be prescribed.
Acute haemorrhagic conjunctivitis (AHC):
Caused by Enterovirus 70 or Coxsackievirus A24, AHC presents as a dramatically painful, sudden-onset bilateral conjunctivitis with profuse subconjunctival haemorrhages that appear within hours. It spreads explosively in epidemics (particularly in crowded conditions) and has caused major outbreaks in South and Southeast Asia, Africa, and Latin America. Despite its alarming appearance, it is self-limiting in 5–10 days and treatment is supportive.
Herpes simplex conjunctivitis:
Primary herpes simplex virus (HSV-1) can cause an acute unilateral follicular conjunctivitis, usually in children, associated with a vesicular skin rash on the eyelid. It is typically self-limiting but topical aciclovir ointment is given to reduce viral shedding and the risk of corneal involvement.
Differential Diagnosis and When to Be Worried
The distinction between bacterial and viral conjunctivitis is clinically important but the more critical skill is recognising when a presentation labelled 'conjunctivitis' is actually something more dangerous. Two situations require special alertness. The first situation is the case where a dangerous diagnosis — anterior uveitis, acute angle-closure glaucoma, keratitis — mimics simple conjunctivitis on superficial inspection because the eye is red and the patient reports discomfort. The second situation is the case where a genuinely infective conjunctivitis has a feature — purulent discharge that reforms immediately after wiping, a neonatal age, failure to respond to appropriate antibiotics — that signals a specific organism requiring non-standard treatment. In both situations, the discriminating features are the red-flag symptoms and signs detailed below. Knowing these red flags, and actively checking for them rather than assuming conjunctivitis on the basis of redness and discharge alone, is the single most important habit for safe management of the acute red eye in primary care.
Bacterial vs viral — practical discrimination:
The most reliable discriminators are discharge character (mucopurulent → bacterial; watery → viral), conjunctival reaction (papillary → bacterial/allergic; follicular → viral/chlamydial), and preauricular node (present and tender → viral). No single feature is 100% sensitive — clinical judgement integrates all findings.
| Feature | Bacterial | Viral |
|---|---|---|
| Discharge | Mucopurulent, lid sticking | Watery/serous |
| Conjunctival reaction | Papillary | Follicular |
| Preauricular node | Absent | Present, tender |
| Corneal involvement | Rare (unless gonococcal) | EKC: subepithelial infiltrates |
| Course | 7–10 days | 2–3 weeks |
Red flags that demand reassessment:
- Any reduction in visual acuity → suspect keratitis or uveitis.
- Photophobia → ciliary spasm from corneal or uveal inflammation, not conjunctivitis.
- Corneal opacity, hypopyon (white fluid level in anterior chamber), or a dendritic ulcer pattern on fluorescein staining → keratitis requiring urgent specialist care.
- Profuse purulent discharge reforming immediately after wiping → gonococcal emergency.
- Neonatal conjunctivitis in the first 28 days of life → always investigate organism before starting topical antibiotics.
- A 'conjunctivitis' that has not improved after 7–10 days of appropriate topical antibiotics → suspect chlamydial (inclusion conjunctivitis) or reconsider diagnosis entirely.
The key teaching point here is that conjunctivitis is a diagnosis of exclusion of the dangerous causes — not the default first assumption.
CLINICAL PEARL
The adenovirus trap: A patient with EKC consults on day 3 of the illness with a red, watery eye and a tender preauricular node. You correctly diagnose viral conjunctivitis and advise lubricants + hygiene. They return on day 14 with blurred vision, photophobia, and gritty discomfort — the subepithelial infiltrates have appeared. This is an expected progression of EKC, not a new infection. Warn every patient with adenoviral conjunctivitis at the first visit that visual symptoms can develop in the second week and they must return immediately if they do — do not wait for a scheduled follow-up.