Page 4 of 18
OP6.2 | Iridocyclitis: Complications, Investigations and Treatment — SDL Guide
Learning Objectives
- Enumerate the complications of iridocyclitis affecting the anterior and posterior segments, with their pathogenetic mechanisms
- Describe a systematic, tiered investigation approach for identifying the underlying aetiology of uveitis
- Explain the pharmacological basis and clinical indications for each step of the iridocyclitis treatment ladder
- Outline the management of the major complications: secondary glaucoma, complicated cataract, and cystoid macular oedema
INSTRUCTIONS
In OP6.1 you learned to recognise iridocyclitis and classify it. This module takes you to the next clinical level: what happens if inflammation is not adequately controlled, how to investigate for the underlying cause, and how to build a treatment plan that prevents both visual loss and steroid toxicity. The complications of undertreated iridocyclitis — posterior synechiae leading to secondary glaucoma, complicated cataract, and cystoid macular oedema — are all preventable with timely, appropriately escalated treatment. Understanding the treatment ladder from cycloplegia through to biologics equips you to manage a wide spectrum of severity and to justify every prescribing decision.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. Ch. 8 — Diseases of the Uveal Tract (textbook)
- Parsons' Diseases of the Eye, 23rd ed. Ch. 17 — The Uveal Tract (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old woman with a 4-year history of juvenile idiopathic arthritis (JIA) presents for a routine check-up. She reports no eye symptoms whatsoever — no redness, no pain. On slit-lamp examination you find 2+ cells in the anterior chamber bilaterally, fine KPs, and beginning posterior synechiae in the right eye. Her best corrected visual acuity is 6/9 on the right, which was 6/6 six months ago. What complications should you now actively look for? What investigations will you order? How will you escalate her treatment, and what is the most sight-threatening complication you must prevent?
WHY THIS MATTERS
Iridocyclitis is not simply an acute inconvenience — undertreated or inadequately managed inflammation leads to a cascade of irreversible structural damage. The visual loss from iridocyclitis complications is largely preventable with timely recognition and appropriate treatment escalation. As a medical graduate, you will be expected to understand not only the first-line treatment but also the rationale for stepping up therapy, the complications of the treatment itself (steroid-induced glaucoma and cataract), and when to refer to or work alongside a rheumatologist for systemic immunosuppression. This module operationalises the clinical decision-making framework that separates competent from excellent management of uveitis.
RECALL
Recall from OP6.1 that iridocyclitis causes breakdown of the blood–aqueous barrier, flooding the anterior chamber with inflammatory cells and protein. Posterior synechiae — adhesions between the posterior iris and anterior lens capsule — were identified as the most important acute complication to prevent. Recall also that the SUN Working Group described four clinical course patterns: acute (<3 months, single episode), recurrent (repeated episodes separated by quiescence ≥3 months without treatment), chronic (persistent inflammation with <3 months quiescence), and chronic recurrent (persistent with acute flares). Chronic and recurrent disease carries by far the greatest risk of complications. In this module you will extend your understanding from recognition to prevention and treatment.
Clinical Presentation and Recurrent Course of Iridocyclitis
Iridocyclitis can present across a wide clinical spectrum — from a dramatic, acutely painful red eye with profound photophobia (classical HLA-B27-associated acute anterior uveitis) to a completely asymptomatic, low-grade chronic inflammation discovered only on routine slit-lamp screening (as in JIA-associated uveitis). This spectrum is clinically important because the asymptomatic forms are paradoxically the most dangerous for long-term vision: patients do not seek care until complications have already developed. The disease course also determines how long treatment must continue and at what threshold further investigation or systemic immunosuppression is warranted. A single acute episode resolving completely with topical therapy carries a different long-term risk profile from chronic smouldering disease that persists despite drops — and the clinician who fails to distinguish these patterns will under-treat the latter and over-investigate the former. Mapping the clinical course is therefore the essential first step before any investigation or treatment escalation decision.
The SUN Working Group's classification of clinical course guides both the duration of treatment and the threshold for escalation:
- Acute uveitis: sudden onset with a limited course (<3 months). The prototype is HLA-B27-associated acute anterior uveitis — dramatic presentation, typically responds well to topical steroids and cycloplegia, resolves fully, but may recur.
- Recurrent uveitis: repeated acute episodes separated by quiescent intervals of ≥3 months without treatment. Each recurrence risks fresh synechiae and cumulative complications.
- Chronic uveitis: persistent inflammation lasting >3 months with <3 months of quiescence off treatment. Associated with JIA (in children), sarcoidosis, TB, Fuchs heterochromic iridocyclitis, and Behçet's disease. Complications accumulate silently over months to years.
- Chronic recurrent uveitis: persistent background inflammation with intercurrent acute exacerbations — the combination most likely to produce severe structural damage.
Understanding the course pattern helps predict the risk of complications and the likely need for systemic immunosuppression.
Anterior Segment Complications of Iridocyclitis
Anterior segment complications arise directly from the inflammatory milieu in the anterior chamber. Each complication follows a mechanistic sequence that can be interrupted at any stage by appropriate treatment — understanding these pathways is the basis for understanding treatment priorities.
1. Posterior synechiae and their consequences:
Posterior synechiae form when inflammatory exudate glues the posterior iris surface to the anterior lens capsule. Partial synechiae produce an irregular, distorted pupil. When synechiae extend to 360° around the pupil, the condition is called seclusio pupillae — the pupil is completely occluded, blocking aqueous flow from the posterior chamber (where it is secreted by the ciliary body) to the anterior chamber (from where it drains). The resulting pressure build-up in the posterior chamber bows the peripheral iris forward — iris bombé — producing a secondary form of angle-closure glaucoma (the angle closes because the peripheral iris contacts the trabecular meshwork).
2. Secondary glaucoma:
Secondary glaucoma complicates iridocyclitis by three distinct mechanisms:
- Trabecular blockage: inflammatory cells, debris, and fibrin physically obstruct the trabecular meshwork, reducing aqueous drainage and raising IOP while the angle itself remains open (secondary open-angle glaucoma pattern).
- Iris bombé/angle-closure: as described above, from seclusio pupillae.
- Steroid-induced IOP rise: a well-recognised adverse effect of topical corticosteroids (particularly prednisolone acetate), which occurs in genetically susceptible individuals (steroid responders — approximately 30% of the population show some IOP rise; 4-6% are high-responders). IOP must be monitored at every visit during steroid treatment.
3. Complicated cataract:
Complicated cataract — typically a posterior subcapsular opacity — develops from two sources: (a) direct toxic effect of chronic inflammation on lens metabolism (altered lens epithelial cell function, disruption of crystallin proteins), and (b) prolonged topical or systemic corticosteroid use, which independently causes posterior subcapsular cataract. The combination of both insults in poorly controlled chronic uveitis makes cataract an almost inevitable complication over years.
4. Band keratopathy:
Band keratopathy is deposition of calcium in Bowman's layer and the superficial corneal stroma, appearing as a greyish-white horizontal band across the interpalpebral zone (the exposed part of the cornea). It occurs in chronic uveitis, particularly in JIA-associated disease (where it is a classical association), hypercalcaemia, and phthisis bulbi. It is treated by chelation with EDTA (ethylenediaminetetraacetic acid) applied topically after superficial keratectomy.
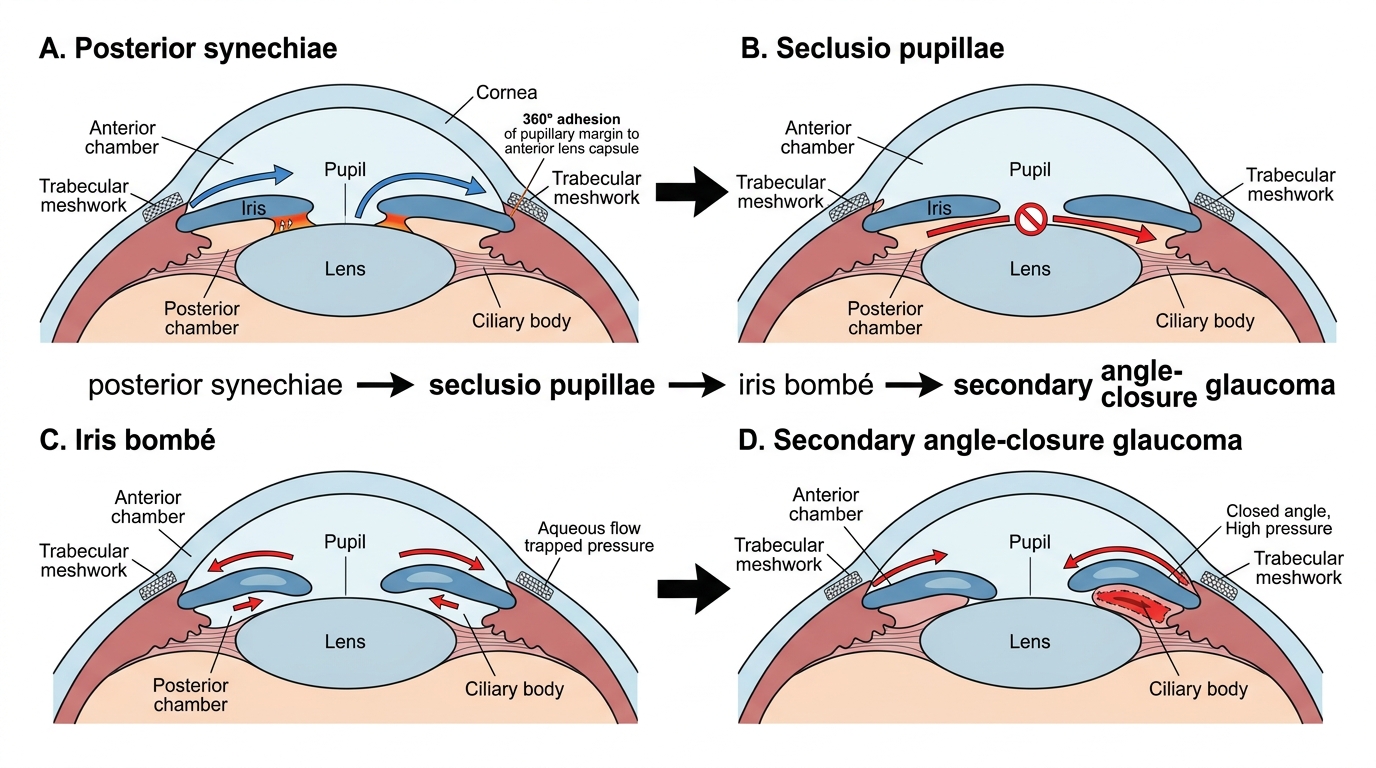
Posterior Synechiae to Iris Bombé and Angle-Closure Glaucoma
Posterior Segment Complications of Iridocyclitis
Although anterior uveitis is, by definition, primarily an anterior segment disease, inflammation in the eye does not respect anatomical boundaries cleanly — particularly in chronic or poorly controlled disease. Posterior segment involvement is especially common in intermediate, posterior, and panuveitis, but can also complicate severe or chronic anterior uveitis.
1. Cystoid macular oedema (CMO): The leading cause of permanent visual loss in uveitis. CMO occurs when inflammatory mediators (prostaglandins, cytokines, and leakage from perifoveal capillaries) disrupt the blood–retinal barrier, allowing fluid to accumulate in the outer plexiform and inner nuclear layers of the macula in a petaloid (flower-petal) pattern — the characteristic appearance on fundus fluorescein angiography (FFA) and optical coherence tomography (OCT). OCT is the investigation of choice for diagnosis and monitoring. CMO reduces central vision insidiously and may not be noticed by the patient until visual acuity has already deteriorated significantly.
2. Epiretinal membrane (ERM): Proliferation of fibrous tissue on the inner retinal surface, leading to macular wrinkling (cellophane maculopathy) and distortion. Detected on OCT. Visual symptoms include metamorphopsia (distorted straight lines).
3. Optic disc oedema and papillitis: Inflammation can involve the optic nerve head (papillitis — anterior optic neuritis), causing swelling of the optic disc and reduced vision with a central/paracentral scotoma. In panuveitis, this is an indicator of severe inflammatory activity.
4. Retinal detachment: In severe uveitis, exudative retinal detachment can occur from massive subretinal fluid accumulation (as in Vogt-Koyanagi-Harada disease). Tractional retinal detachment is a late complication of neovascularisation in chronic disease.
5. Hypotony maculopathy: Paradoxically, very low IOP from ciliary body shutdown in severe chronic uveitis can cause macular folds and visual loss — hypotony maculopathy.
SELF-CHECK
A patient with chronic uveitis reports gradual blurring of central vision over 3 months despite having quiet-looking anterior chambers. OCT of the macula shows fluid in a flower-petal pattern around the fovea. The most likely diagnosis is:
A. Epiretinal membrane
B. Cystoid macular oedema (CMO)
C. Exudative retinal detachment
D. Hypotony maculopathy
Reveal Answer
Answer: B. Cystoid macular oedema (CMO)
Cystoid macular oedema (CMO) is the leading cause of visual loss in chronic uveitis. It presents with gradual central blurring and shows a characteristic 'flower-petal' or cystoid pattern of fluid in the perifoveal area on OCT and FFA. The anterior chamber may appear deceptively quiet while CMO progresses — OCT monitoring is essential in all patients with chronic uveitis.