Page 5 of 18
OP6.2 | Iridocyclitis: Complications, Investigations and Treatment — SDL Guide (Part 2)
Investigations in Iridocyclitis: What to Order and Why
The decision to investigate — and which tests to order — must be driven by the clinical context. Investigations are NOT required for every first presentation of acute anterior uveitis in a young adult (which is most likely idiopathic or HLA-B27-associated). Investigation becomes mandatory when: (1) the clinical picture is bilateral, (2) the course is chronic or recurrent, (3) features suggest a granulomatous aetiology, (4) posterior segment involvement is present, or (5) response to treatment is poor. A blanket investigative approach to every red eye is wasteful, anxiety-provoking, and often misleading — a mildly elevated ACE level in a young patient with a clear-cut first episode of HLA-B27-associated iridocyclitis is more likely a laboratory variation than sarcoidosis, and acting on it drags the patient into an unnecessary specialist workup. Conversely, failing to order a chest X-ray and Mantoux in a patient with mutton-fat KPs in the Indian subcontinent risks missing treatable ocular tuberculosis — with potentially catastrophic consequences for both vision and systemic health. Clinical context is therefore the filter through which every investigation decision must pass.
Provided image
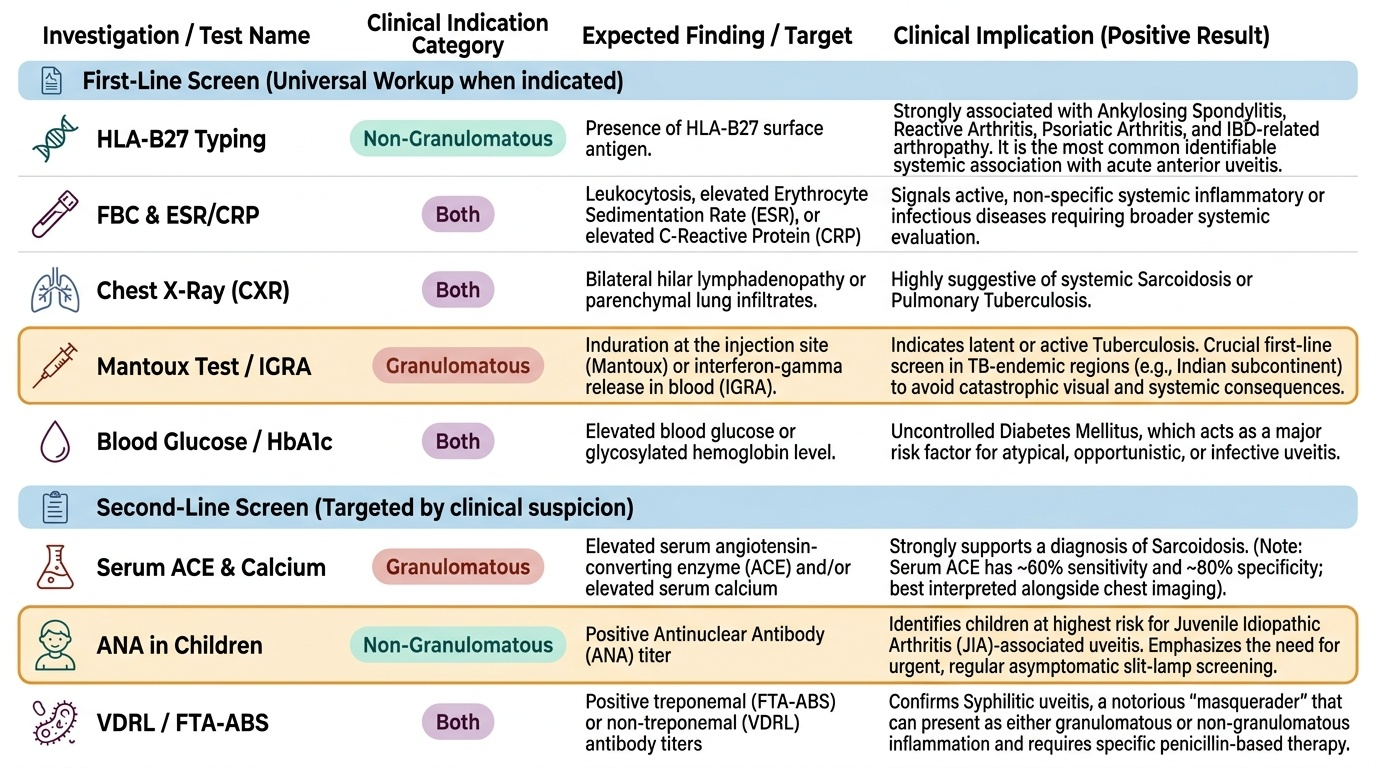
A tiered investigation strategy avoids unnecessary cost and patient anxiety:
First-line screen (for most patients requiring workup):
- HLA-B27 typing: positive in ankylosing spondylitis, reactive arthritis, psoriatic arthritis, IBD-related arthropathy — the most common identifiable systemic association with acute non-granulomatous anterior uveitis.
- Full blood count (FBC) and ESR/CRP: screens for systemic inflammatory disease.
- Chest X-ray: sarcoidosis (bilateral hilar lymphadenopathy), tuberculosis.
- Mantoux test/IGRA (interferon-gamma release assay): tuberculosis screening — essential in India where TB is the most common granulomatous uveitis cause.
- Blood glucose / HbA1c: diabetes as a risk factor for infective uveitis.
Second-line (targeted by clinical suspicion):
- Serum ACE (angiotensin-converting enzyme) and serum calcium: sarcoidosis (sensitivity ~60%, specificity ~80%; useful alongside chest X-ray and CT chest).
- ANA (antinuclear antibody) in children: JIA-associated uveitis (ANA-positive JIA carries highest risk of chronic anterior uveitis — must have regular slit-lamp screening even when asymptomatic).
- VDRL/FTA-ABS: syphilitic uveitis (a cause of any anatomical type, bilateral chronic uveitis).
- Toxoplasma IgG/IgM: posterior uveitis with retinochoroiditis (pale focus adjacent to old pigmented scar).
- ANCA (antineutrophil cytoplasmic antibody): granulomatosis with polyangiitis (scleritis/uveitis association).
Ocular imaging for complications:
- OCT (optical coherence tomography): investigation of choice for CMO, epiretinal membrane, and retinal structural complications; monitor response to treatment.
- FFA (fundus fluorescein angiography): maps vascular leakage in CMO (flower-petal pattern), neovascularisation, vasculitis.
- B-scan ultrasonography: if media opacity prevents visualisation of the posterior segment (e.g. cataract, vitreous haemorrhage).
Establishing the Aetiology: Diagnosing the Underlying Cause
Integrating investigation results with clinical features establishes the aetiological diagnosis that drives specific treatment beyond generic steroids and cycloplegia. The following profiles guide clinical reasoning:
HLA-B27-positive + spondyloarthropathy history: Acute, non-granulomatous, unilateral alternating anterior uveitis. Treatment is ophthalmological (topical steroids/cycloplegia); systemic disease managed by rheumatology. Inform patient that recurrences are expected and any red eye requires same-day ophthalmology referral.
Chest X-ray showing bilateral hilar lymphadenopathy + elevated serum ACE + granulomatous KPs: Strongly suggests sarcoidosis. Can cause anterior, intermediate, posterior, or panuveitis. Systemic steroids (and steroid-sparing agents) are the mainstay; tissue biopsy (e.g. conjunctival nodule, lymph node) may confirm.
Mantoux positive/IGRA positive + granulomatous uveitis in India: Suspect ocular tuberculosis. Initiation of anti-tubercular therapy (ATT — four-drug HRZE regimen for 2 months, then HR for 4 months) in addition to topical steroids is standard practice. Paradoxical worsening of inflammation on starting ATT (immune reconstitution) can occur — continued topical steroids manage this.
ANA-positive child with JIA (oligoarticular type): High risk of JIA-associated chronic uveitis — asymptomatic, bilateral, fine KPs, requires 3–6-monthly slit-lamp screening regardless of symptoms. Band keratopathy and complicated cataract are the signature complications. Methotrexate and adalimumab are used when topical steroids are insufficient.
Posterior retinochoroiditis lesion with adjacent pigmented scar: Classic toxoplasma retinochoroiditis (Toxoplasma gondii). Treat with pyrimethamine + sulfadiazine + folinic acid (or clindamycin as alternative); steroids added to reduce inflammatory response around the lesion once anti-parasite cover is established.
Young woman, bilateral, with systemic features (meningism, vitiligo, alopecia, tinnitus): Vogt-Koyanagi-Harada (VKH) syndrome — bilateral granulomatous panuveitis with exudative retinal detachment; high-dose systemic steroids are the treatment of choice.
SELF-CHECK
A 14-year-old girl with oligoarticular JIA (ANA-positive) presents for a routine check-up with NO eye complaints. Slit-lamp reveals 1+ cells bilaterally. The MOST appropriate immediate action is:
A. Reassure — cells are expected with JIA and treatment is not required while asymptomatic
B. Start topical prednisolone acetate 1% four times daily and arrange urgent review in 2 weeks
C. Perform HLA-B27 testing before starting any treatment
D. Refer directly for systemic methotrexate without topical treatment
Reveal Answer
Answer: B. Start topical prednisolone acetate 1% four times daily and arrange urgent review in 2 weeks
JIA-associated uveitis is characteristically asymptomatic, yet active inflammation (cells present on slit-lamp) causes progressive damage — posterior synechiae, band keratopathy, cataract, and CMO. Even 'silent' cellular activity must be treated. Topical prednisolone acetate and cycloplegia are the first-line agents; if insufficient, methotrexate or adalimumab are added. HLA-B27 is not relevant (JIA-uveitis is ANA-associated); methotrexate alone without topical treatment is not standard first-line.
Treatment of Iridocyclitis: The Therapeutic Ladder
Treatment of iridocyclitis follows a stepwise therapeutic ladder, escalating from local to systemic agents as required by severity and chronicity. The overarching goals at every step are to suppress inflammation, maintain vision, and minimise treatment toxicity. The ladder metaphor is deliberate: each rung is justified by failure or insufficiency of the rung below, and jumping rungs exposes patients to unnecessary systemic toxicity. A first episode of acute non-granulomatous anterior uveitis almost never needs systemic immunosuppression; conversely, a child with JIA-associated chronic bilateral uveitis who is still showing 2+ cells after adequate topical prednisolone should be escalated promptly to methotrexate — delay accumulates irreversible structural damage. Understanding which clinical features trigger each step-up, and which monitoring obligations accompany each level, is the practical core of this framework.
Provided image
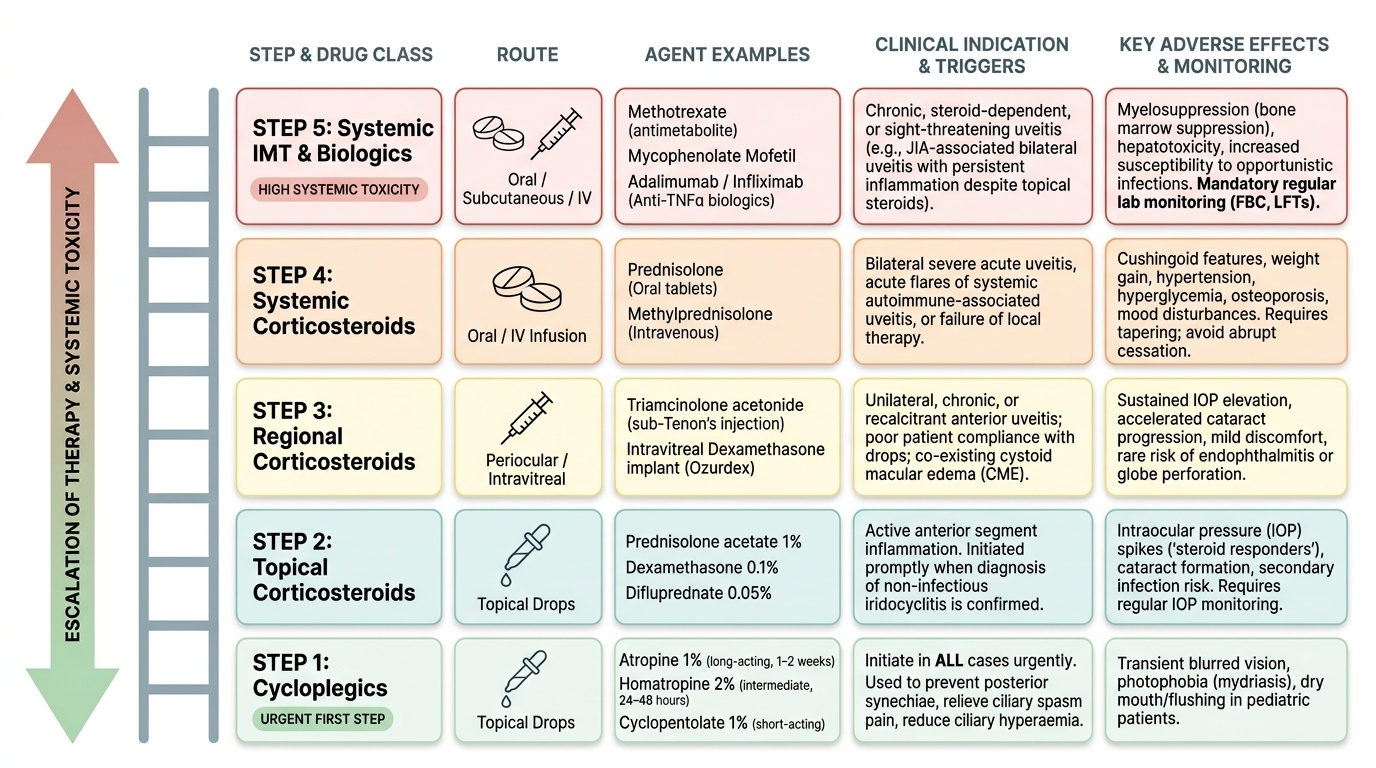
Step 1 — Cycloplegia (ALL cases, first and urgently):
Cycloplegic agents (anticholinergics) paralyse the iris sphincter and ciliary muscle, keeping the pupil dilated. Agents used:
- Atropine 1% eye drops: long-acting (1–2 weeks), used in severe acute iridocyclitis and in children to prevent amblyopia.
- Homatropine 2% eye drops: intermediate duration (24–48 hours), preferred for milder or monitoring-phase treatment.
- Cyclopentolate 1%: shorter acting, used diagnostically and in milder cases.
Purpose: prevent posterior synechiae, relieve ciliary spasm pain, and reduce ciliary hyperaemia. Must be started before steroids — this is the urgent non-negotiable first step.
Step 2 — Topical corticosteroids:
Prednisolone acetate 1% (preferred — best anterior chamber penetration) or dexamethasone 0.1% are instilled frequently: up to every 1–2 hours in severe acute disease, tapering as inflammation resolves. Taper is achieved by reducing frequency (from hourly → 2-hourly → 4× daily → twice daily → once daily → alternate days → stop), NOT by switching to a weaker concentration. The taper must be slow — rapid withdrawal risks rebound flare.
Monitor IOP at every visit during topical steroid use — steroid responders can develop raised IOP within 2–6 weeks.
Step 3 — Periocular corticosteroids:
For persistent or severe anterior/intermediate uveitis not controlled by topical drops. Sub-Tenon's injection of triamcinolone acetonide (40 mg) or methylprednisolone delivers high local concentration with reduced systemic absorption. Intravitreal triamcinolone is used for posterior uveitis and CMO.
Step 4 — Systemic corticosteroids:
Indicated when: bilateral disease, intermediate/posterior/panuveitis, failure of topical alone, or when a systemic disease requires systemic treatment. Oral prednisolone is started at 1 mg/kg/day (typically 40–80 mg/day) and tapered over weeks to months guided by clinical and OCT response.
Step 5 — Steroid-sparing immunosuppressants:
When steroid doses needed to control uveitis cause unacceptable toxicity (Cushingoid features, glaucoma, osteoporosis, diabetes), or when disease is chronic and high-dose steroids cannot be sustained:
- Methotrexate (7.5–25 mg weekly): first-choice in JIA-associated uveitis; requires folate supplementation and LFT monitoring.
- Mycophenolate mofetil: effective in non-infectious uveitis, well tolerated.
- Azathioprine: used in Behçet's disease and other systemic uveitis syndromes.
- Ciclosporin: effective but nephrotoxic; reserved for refractory cases.
Step 6 — Biologics:
Anti-TNF agents (adalimumab, infliximab) are used in refractory uveitis associated with JIA (adalimumab is FDA-approved specifically for JIA uveitis) and spondyloarthropathies. Rituximab (anti-CD20) is used in ANCA-associated uveitis.