Page 9 of 23
OP8.4 | Cataract Surgery: Anaesthesia, ECCE Steps, Complications and Postoperative Treatment — SDL Guide
Learning Objectives
- Enumerate the types of cataract surgery and their indications, with emphasis on phacoemulsification, MSICS, ECCE, and ICCE
- Describe the techniques of ocular anaesthesia used for cataract surgery including topical, sub-Tenon, peribulbar, retrobulbar, and general anaesthesia
- Describe the sequential steps of extracapsular cataract extraction (ECCE)
- Enumerate the intraoperative complications of cataract surgery and their immediate management
- Discuss the postoperative complications of cataract surgery — early and late — with their clinical features and management
- Describe the standard postoperative treatment protocol following cataract surgery
INSTRUCTIONS
Cataract surgery is the most commonly performed elective surgical procedure in India and one of the most transformative in all of medicine — a 30-minute operation that restores a patient's ability to see their grandchildren's faces, read the newspaper, and work safely. This module takes you inside the operating theatre: from the choice of anaesthesia to the final suture, from the predictable steps of extracapsular extraction to the complications that test even experienced surgeons. Whether you will perform cataract surgery yourself or assist and counsel patients, this knowledge is clinically essential.
References
- Khurana AK. Comprehensive Ophthalmology, 7th edition. Chapter 7: Diseases of the Lens — Cataract Surgery. (textbook)
- Parson JH. Diseases of the Eye, 22nd edition. Chapter 8: Cataract — Surgical Techniques and Complications. (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 8:00 AM in the operating theatre. You are standing at the foot of the table as an observer, watching Dr. Lakshmi, a senior ophthalmologist, prepare for the first case — a 70-year-old man with a mature senile cataract. The patient is draped and positioned. Two drops of proxymetacaine were instilled twenty minutes ago. The microscope is adjusted to 20× magnification. With steady hands, Dr. Lakshmi makes a 2.5 mm clear corneal incision and positions a capsulorhexis forceps at the lens capsule. Within 20 minutes, a phacoemulsification probe has emulsified the brown nucleus, the cortex has been aspirated, and a foldable acrylic IOL is being unfolded inside the capsular bag. The patient is calm, awake, and conversing quietly. By the time the drape is removed, his vision — blurry beyond the bright operative light — has already begun its journey to recovery. This is modern cataract surgery. But to understand it fully, you must also understand its historical predecessors, its complications, and the post-operative regimen that determines whether the surgical result holds.
WHY THIS MATTERS
OP8.4 is classified at KH (Knowledge with Help) level under NMC CBME — meaning you must be able to enumerate, describe, and discuss cataract surgery techniques, anaesthesia, and complications in clinical examinations and case discussions. More importantly, as a doctor in any setting — district hospital, community health centre, or urban referral unit — you will counsel patients before surgery, recognise post-operative complications when they present to you, and decide urgency of referral. A patient who presents three days post-cataract surgery with a red eye, pain, and reduced vision needs you to immediately consider endophthalmitis and arrange urgent ophthalmic review. This knowledge is clinical, not academic.
RECALL
Recall from the cataract pathogenesis module that the lens has three zones — cortex, adult nucleus, and fetal/embryonic nucleus — and is enclosed by an elastic capsule. The posterior capsule is especially thin (~2–4 µm) and is the most important surgical boundary in cataract surgery — its integrity determines whether an IOL can be placed in the capsular bag. Recall also the four surgical options introduced there: phacoemulsification (small incision, foldable IOL, current standard), MSICS (manual small-incision, India high-volume), ECCE (large incision, largely replaced), and ICCE (whole lens, largely obsolete). In the preoperative module, you learned that the choice of technique depends on corneal endothelial count, nuclear hardness, available equipment, and surgeon expertise. This module fills in the surgical detail.
Clinical Presentation — When the Cataract Patient Reaches Surgery
The patient presenting for cataract surgery has already traversed a clinical journey: vision loss identified, cataract diagnosed, medical fitness assessed, and a decision reached that surgical benefit outweighs operative risk. Understanding this patient's perspective and clinical context before entering the surgical and anaesthetic detail grounds the learner in clinical reality. Symptoms that drive the referral are the same as those of cataract in general — progressive painless visual blur, glare, monocular diplopia, and functional impairment in occupational or daily tasks. The threshold for surgical intervention is functional, not acuity-based: a driver who can no longer pass the vision standard, a weaver who cannot see the needle, or a reader who cannot manage with updated spectacles are all appropriate surgical candidates even if formal Snellen acuity appears borderline.
At the point of surgical listing, the patient typically has best-corrected visual acuity worse than 6/18 in the operative eye, or has a lens opacity causing functional impairment disproportionate to the measured acuity (as in posterior subcapsular cataract, where glare and contrast sensitivity loss are severe while Snellen acuity may be preserved in clinic lighting). The preoperative surgical candidate has also been screened for red-flag findings — poorly controlled systemic disease, concurrent ocular pathology limiting visual prognosis, or anatomical factors increasing surgical risk — that may alter the surgical plan or delay the procedure. Your role as a student or intern in this setting is to understand how these clinical criteria were applied to the individual patient in front of you, and to participate meaningfully in the preoperative workup and counselling.
Types of Cataract Surgery and Their Indications
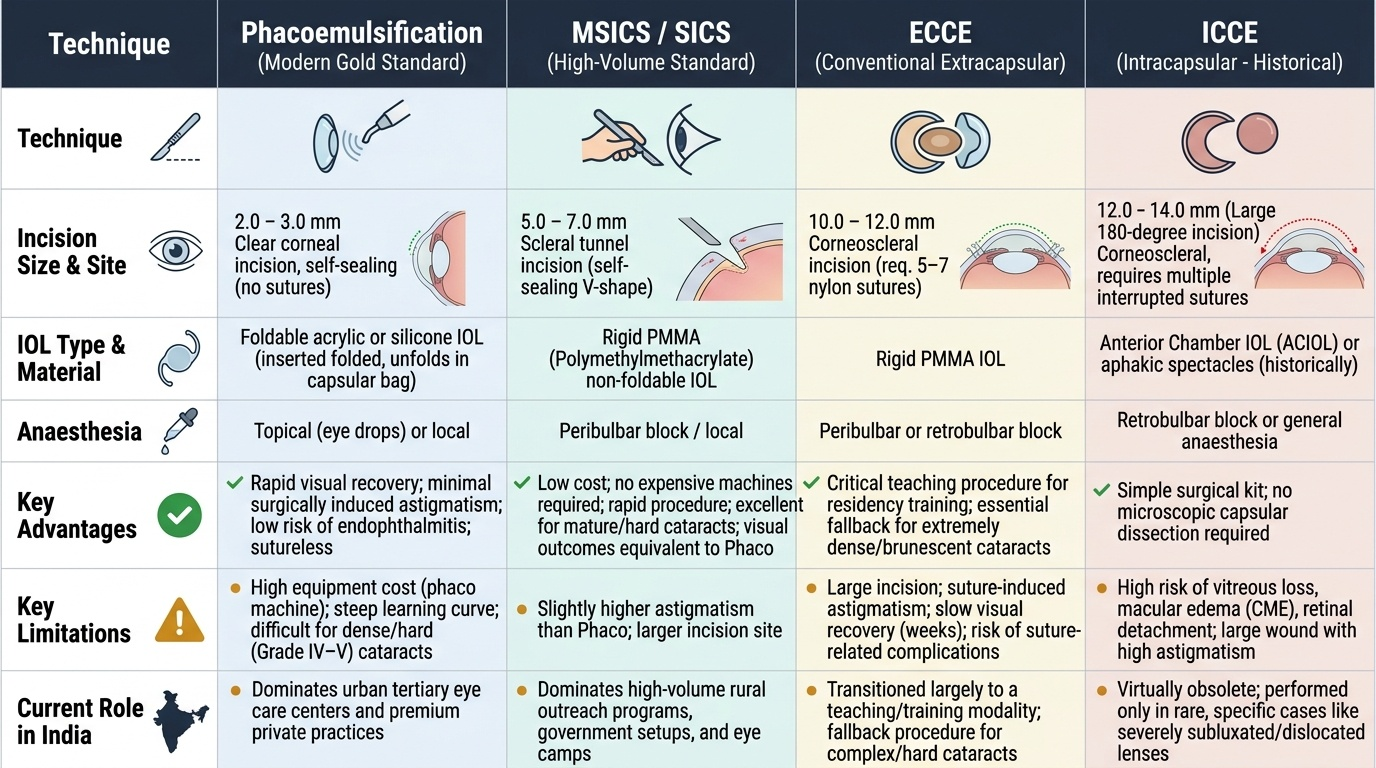
Four surgical techniques have been developed for cataract extraction, representing successive generations of innovation — from the crude couching described in ancient Sushruta Samhita, to the precision of modern phacoemulsification. Each technique remains relevant to some degree in the Indian context, where infrastructure, cataract density, and patient volume vary enormously across settings. Phacoemulsification dominates urban tertiary centres; MSICS dominates high-volume rural and camp settings; ECCE is now largely a teaching procedure but remains essential for very dense cataracts unsuitable for phaco; ICCE is almost never performed today except in rare cases of subluxated lenses. Understanding the indications, advantages, and limitations of each technique is essential for the NMC CBME examination, for clinical rotations, and for career-long surgical decision-making. An intern who understands why a surgeon chooses MSICS over phaco in a given patient can contribute meaningfully to the consent discussion and anticipate the postoperative care pathway.
Provided image
1. Phacoemulsification ('Phaco'): A 2–3 mm self-sealing clear corneal incision is made. A phacoemulsification probe uses ultrasonic energy (approximately 40 kHz) to emulsify the lens nucleus, which is then aspirated. A foldable IOL (acrylic or silicone) is inserted folded through the same small incision and unfolds within the capsular bag. The incision seals by itself (no sutures in most cases). This is the current global standard: rapid recovery, minimal surgically induced astigmatism, reduced endophthalmitis risk, early visual rehabilitation. Limitations: requires expensive phacoemulsification machine, learning curve, difficult with very hard brunescent (grade IV–V) nuclei, and potential for more endothelial cell loss in dense cataracts.
2. Manual Small-Incision Cataract Surgery (MSICS/SICS): A 5–7 mm self-sealing scleral tunnel incision allows the nucleus to be expressed manually without phacoemulsification energy. A rigid PMMA (polymethylmethacrylate) IOL is implanted (one suture sometimes needed). Visual outcomes are equivalent to phacoemulsification in multiple Indian studies. MSICS is the preferred technique for Indian high-volume settings, high-density nuclei, and low-resource environments — it requires no expensive machine, works well with hard cataracts, and is faster per case in experienced hands. It is the workhorse of the NPCBVI camp surgery programme.
3. Extracapsular Cataract Extraction (ECCE): A 10–12 mm limbal incision is made; the anterior capsule is opened; the nucleus is expressed in one piece manually; cortex is aspirated; and a rigid PMMA IOL is implanted. The wound requires multiple interrupted or continuous sutures (7-0/10-0 nylon), which cause significant post-operative astigmatism and extend recovery time. ECCE is now largely replaced by phacoemulsification and MSICS in most centres, but remains relevant where equipment for phaco/MSICS is unavailable, and historically it remains the reference standard for surgical teaching of steps and complications.
4. Intracapsular Cataract Extraction (ICCE): The entire lens — including its capsule — is extracted using a cryoprobe that freezes to and lifts the lens, after enzymatic zonulysis with alpha-chymotrypsin. No capsular bag remains for a standard IOL; an anterior chamber IOL (AC-IOL) must be used, or the patient is left aphakic and corrected with spectacles/contact lens. ICCE is now largely obsolete — it carries high risk of vitreous prolapse, cystoid macular oedema, and corneal endothelial damage. It is reserved for specific situations such as complete zonular dehiscence with a totally subluxated lens.
Ocular Anaesthesia Techniques
The choice of anaesthesia for cataract surgery depends on the surgical technique, surgeon preference, patient cooperation, and patient systemic status. Unlike most major surgeries, cataract surgery is typically performed under local anaesthesia in adults — the patient remains awake throughout, which necessitates clear pre-operative communication about what to expect.
1. Topical Anaesthesia: Instillation of proxymetacaine 0.5% (or lignocaine 2% gel) drops 10–15 minutes before surgery. This eliminates surface pain without injection. The patient can move their eye freely but cooperates voluntarily. No akinesia (eye movement is possible — requires experienced surgeon and fully cooperative patient). The most modern and minimally invasive form — no injection risk, fastest recovery from anaesthesia effect, no lid/conjunctival swelling. Ideal for phacoemulsification in cooperative patients.
2. Sub-Tenon Block (Episcleral Block): A small cut in the conjunctiva and Tenon's capsule near the limbus; a blunt cannula delivers local anaesthetic (lignocaine + bupivacaine) into the episcleral space. Provides good akinesia and analgesia with minimal risk — no risk of globe perforation or retrobulbar haemorrhage. Increasingly preferred over retrobulbar block.
3. Peribulbar Block: Injection of local anaesthetic into the peribulbar space (outside the extraocular muscle cone), using one or two injections at the inferior orbital rim and/or lateral canthus. Provides akinesia and good analgesia. Safer than retrobulbar because the needle does not enter the muscle cone — lower risk of globe perforation and optic nerve injury. May require larger volume (~8–12 mL) and 5–10 minutes to take full effect. Widely used in ECCE and MSICS.
4. Retrobulbar Block: Injection of local anaesthetic inside the muscle cone (retrobulbar space), using a sharp needle directed posteriorly. Provides excellent akinesia and profound analgesia rapidly with smaller volume. However, carries higher risks: globe perforation (especially in highly myopic eyes with long axial length), optic nerve injury (direct needle trauma or optic nerve sheath haematoma), retrobulbar haemorrhage (rapidly expanding — can compress optic nerve and cause blindness; requires lateral canthotomy), and brainstem anaesthesia (accidental subarachnoid injection via optic nerve dural sleeve). Use with caution — increasingly replaced by peribulbar and sub-Tenon techniques.
5. General Anaesthesia: Reserved for children (congenital cataract), patients unable to cooperate (intellectual disability, Parkinson's disease, severe anxiety), and patients requiring combined surgery. Carries full systemic anaesthetic risks — full pre-anaesthetic assessment required.
Local anaesthetic agents: Lignocaine 2% (rapid onset, 1–2 hours duration) ± bupivacaine 0.5% (slower onset, 4–6 hours duration) are the most commonly used combination. Hyaluronidase is often added to facilitate spread of the anaesthetic agent.
SELF-CHECK
A surgeon is performing cataract surgery under retrobulbar block on a 65-year-old woman with a history of high myopia (axial length 28 mm). Which serious complication is most at risk from this anaesthetic choice?
A. Corneal decompensation
B. Globe perforation
C. Posterior capsular rupture
D. Endophthalmitis
Reveal Answer
Answer: B. Globe perforation
Highly myopic eyes have an elongated axial length, making the globe more prominent and longer. This increases the risk of globe perforation with a retrobulbar needle. The needle may enter the eye through the sclera — especially at the back of the globe — during retrobulbar injection. This is one reason why sub-Tenon or peribulbar blocks are preferred in highly myopic patients. Corneal decompensation is related to endothelial cell damage from phacoemulsification energy, not anaesthesia. Posterior capsular rupture and endophthalmitis are intraoperative and postoperative surgical complications.