Page 10 of 23
OP8.4 | Cataract Surgery: Anaesthesia, ECCE Steps, Complications and Postoperative Treatment — SDL Guide (Part 2)
Steps of Extracapsular Cataract Extraction (ECCE)
ECCE remains the cornerstone surgical technique for the NMC CBME examination because it is technically teachable and historically validated, and because all modern techniques — phaco, MSICS — share the same fundamental principles: capsular preservation, cortex aspiration, and IOL implantation. The following steps describe a classic ECCE under peribulbar block. Mastering the sequence of ECCE steps, and the reasoning behind each, prepares you to understand the surgical complications that can occur at each stage — and to anticipate the surgeon's next action during theatre observation. The steps also teach the anatomy of the anterior segment from a surgical perspective: why the incision is placed at the limbus, why the capsulotomy must be complete before nucleus expression, and why cortical aspiration requires such meticulous technique to avoid posterior capsule rupture. Each step has an intraoperative complication that can arise if it is performed incorrectly — knowing the steps allows you to recognise and understand those complications when you see them.
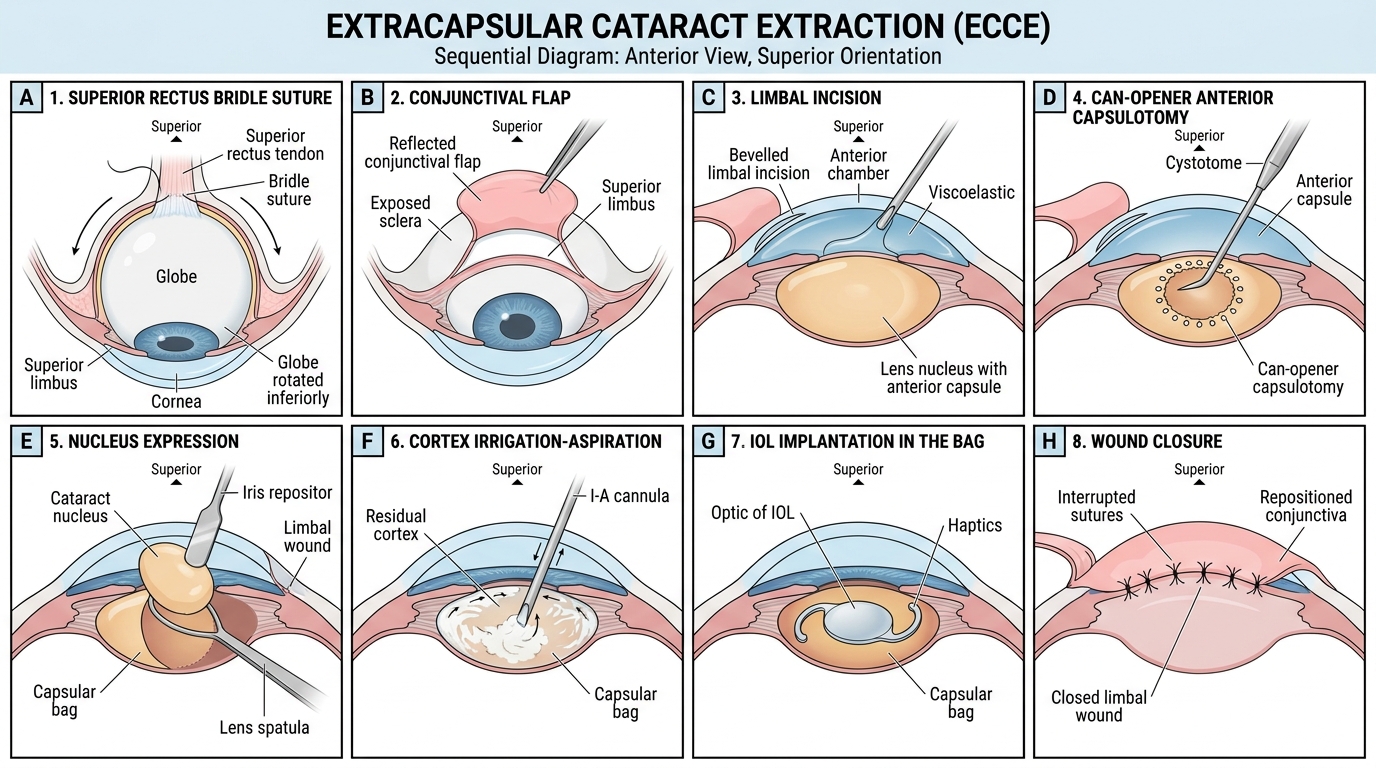
Eight Steps of Extracapsular Cataract Extraction
Step 1 — Superior Rectus Bridle Suture: A 4-0 black silk suture is passed beneath the superior rectus muscle tendon to fix and control the globe position (preventing eye movement under local block) and to rotate the eye inferiorly for better surgical access. This is less used with topical anaesthesia.
Step 2 — Conjunctival Flap: A limbus-based or fornix-based conjunctival flap is raised at the superior limbus to expose the scleral tissue and the limbus, and to protect the conjunctiva from sutures.
Step 3 — Limbal Incision: A 10–12 mm incision is made at or just posterior to the corneoscleral junction (limbus), at the superior aspect. The incision is bevelled to create a shelved entry into the anterior chamber. Viscoelastic (methylcellulose or hyaluronic acid) is injected to maintain the anterior chamber and protect the endothelium.
Step 4 — Anterior Capsulotomy (Can-Opener Capsulotomy): Using a cystotome (a bent 26-gauge needle) or a utrata forceps, a series of small punctures are made in the anterior capsule in a circular pattern — creating a 'can-opener' opening approximately 8–9 mm in diameter. This opens the anterior face of the capsular bag to access the nucleus. In modern surgery, a continuous curvilinear capsulorhexis (CCC) is preferred — a smooth, uninterrupted circular tear that is stronger and less likely to extend posteriorly.
Step 5 — Hydrodissection and Nucleus Expression: Balanced salt solution (BSS) is injected under the anterior capsule to separate the nucleus from the cortex (hydrodissection) and to free the nuclear–epinuclear junction (hydrodelineation). The lens is then expressed by combined pressure at the 6 o'clock limbus (with an irrigating vectis or lens spoon) while counter-pressure is applied at the 12 o'clock limbal lip — the nucleus is delivered into the anterior chamber and out through the wound.
Step 6 — Cortex Aspiration (Irrigation-Aspiration): Residual soft cortical material is removed using a manual irrigation-aspiration (I/A) cannula or an automated I/A handpiece. Complete cortex removal is critical — residual cortex causes inflammation and increases PCO risk. The posterior capsule must be kept intact throughout.
Step 7 — IOL Implantation: The capsular bag is inflated with viscoelastic. A rigid PMMA IOL (typically 6.5 mm optic, 12.5–13 mm total length) is introduced into the capsular bag with an IOL introducer or forceps. The haptics (supporting arms) are positioned within the bag to centre the optic. The viscoelastic is then thoroughly aspirated (residual viscoelastic causes post-operative IOP spike).
Step 8 — Wound Closure: The limbal incision is closed with multiple interrupted 10-0 nylon sutures (or a single continuous suture). The conjunctival flap is repositioned and sutured or cauterised. A subconjunctival injection of antibiotic (e.g. gentamicin 20 mg) and steroid (betamethasone 2 mg) is given. An eye pad and shield are applied.
Intraoperative Complications of ECCE
Every surgical step in cataract surgery carries a specific risk. Recognising intraoperative complications immediately and responding correctly determines the final visual outcome. The following are the major intraoperative complications, listed from most to least frequent in typical practice.
1. Posterior Capsular Rupture (PCR): The most common serious intraoperative complication — occurs during hydrodissection, nucleus expression, or cortex aspiration if the posterior capsule (only 2–4 µm thick) is inadvertently torn. If PCR is small and without vitreous prolapse: a three-piece IOL can still be placed in the sulcus (not in the bag). If vitreous prolapses through the tear: an anterior vitrectomy must be performed to clear vitreous from the anterior chamber (vitreous in the wound causes cystoid macular oedema and increases retinal traction risk).
2. Vitreous Loss: Occurs when vitreous prolapse follows PCR. Vitreous must be meticulously cleared with a vitrector — no vitreous should incarcerate in the wound. If extensive vitreous loss occurs, IOL implantation may need to be deferred or an anterior chamber IOL used.
3. Nucleus Drop into Vitreous: If the posterior capsule ruptures completely during nucleus expression or phacoemulsification, the entire nucleus or a fragment may fall into the vitreous cavity. This is a serious complication requiring planned pars plana vitrectomy (posterior segment surgery) — typically by a vitreoretinal surgeon. Do NOT attempt to retrieve the nucleus blindly through the anterior chamber.
4. Corneal Burn (during phacoemulsification): Excessive ultrasonic energy or inadvertent phaco probe contact with the corneal tunnel can cause a thermal corneal wound burn — the collagen denatures, the incision becomes misshapen, and significant astigmatism and scarring result.
5. Hyphema: Bleeding into the anterior chamber from iris or ciliary body vessels — especially if iris trauma occurs. Usually resolves spontaneously, but may temporarily obscure the view.
6. Expulsive (Suprachoroidal) Haemorrhage: A rare but catastrophic event — sudden massive bleeding in the suprachoroidal space during surgery, causing dramatic rise in IOP, the wound to open, and the intraocular contents to be expelled ('expulsed') from the eye. Risk factors: uncontrolled hypertension, anticoagulation, high myopia, arteriosclerosis. Management: immediately close the wound and apply pressure; posterior sclerotomies may be needed to drain blood.
7. Phacodonesis / Zonular Dialysis: Weak or broken zonular fibres (seen in pseudoexfoliation, trauma, Marfan syndrome) may cause the lens to wobble or luxate during surgery, dramatically increasing the risk of PCR and nucleus drop.
SELF-CHECK
During ECCE in a 68-year-old patient, the posterior capsule ruptures with vitreous prolapse. The nucleus has been delivered successfully. What is the MOST appropriate next step?
A. Complete the IOL implantation in the capsular bag and close the wound
B. Perform anterior vitrectomy to clear vitreous from the anterior chamber, then place IOL in the sulcus if possible
C. Immediately refer to retinal surgery for pars plana vitrectomy
D. Close the wound and defer IOL implantation to a second surgery
Reveal Answer
Answer: B. Perform anterior vitrectomy to clear vitreous from the anterior chamber, then place IOL in the sulcus if possible
After posterior capsular rupture with vitreous prolapse, the priority is meticulous anterior vitrectomy — clearing all vitreous from the anterior chamber and wound to prevent vitreous incarceration, cystoid macular oedema, and retinal traction. After vitrectomy, if sufficient capsular support exists, an IOL can be placed in the sulcus (not in the bag, since the bag is now compromised). Pars plana vitrectomy by a retinal surgeon is needed only if the nucleus has dropped into the vitreous — not for anterior vitreous prolapse alone. Closing without vitrectomy leaves vitreous in the wound, a major source of long-term complications.
Postoperative Complications and Their Management
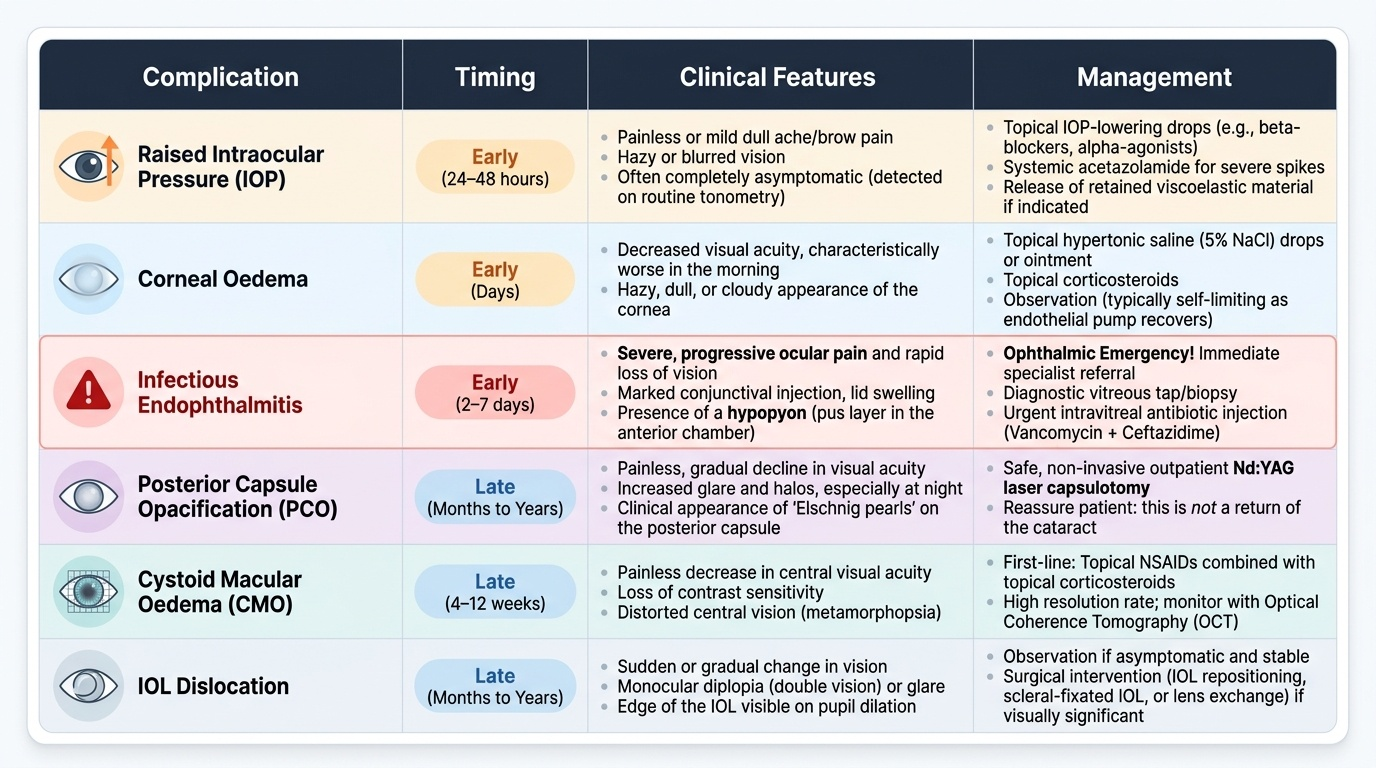
Postoperative complications after cataract surgery are classified as early (within the first six weeks) and late (months to years after surgery). Recognition of these complications — their presentation, timeline, and management — is essential for every doctor who may see a post-cataract patient, whether in an ophthalmic unit or a general outpatient clinic. The most feared early complication is infectious endophthalmitis, a sight-threatening emergency requiring immediate intravitreal antibiotic injection and specialist input; delay by even a few hours significantly worsens the visual outcome. Other early complications — raised IOP, corneal oedema, wound leak — are more common but less catastrophic when recognised promptly. Late complications, particularly posterior capsule opacification (PCO), are so common that patients must be counselled about them before surgery: PCO is not a return of the cataract, and can be permanently corrected with a single YAG laser capsulotomy in the outpatient clinic. Understanding the complication profile also informs the postoperative prescription and counselling about red-flag symptoms.
Provided image
Early Complications:
1. Raised Intraocular Pressure (IOP): Occurs within the first 24–48 hours; causes include residual viscoelastic in the trabecular meshwork, pupillary block from the IOL, or pre-existing glaucoma. Managed with IOP-lowering medications (timolol, acetazolamide); IOL-induced pupillary block requires peripheral iridotomy.
2. Corneal Oedema (Striate Keratopathy): Reversible corneal endothelial cell loss from surgical trauma, phacoemulsification energy, or iris/instruments contact. Presents as stromal oedema, Descemet folds, and reduced vision in the first few days. Usually resolves spontaneously as endothelium recovers (2–4 weeks). Persistent oedema (bullous keratopathy) = irreversible endothelial failure requiring corneal graft (DSAEK/DMEK).
3. Uveitis (Anterior Iritis): Mild post-operative inflammation is universal; sterile uveitis is managed with topical steroid drops (prednisolone acetate 1% six times daily) tapering over 6 weeks. Severe or worsening uveitis after the first 48 hours requires exclusion of endophthalmitis.
4. Endophthalmitis: The most dreaded early post-operative complication. Typically presents 2–7 days after surgery with acute pain, red eye, photophobia, reduced vision, hypopyon (pus in anterior chamber), and vitreous haze. The commonest causative organism is Staphylococcus epidermidis (normal ocular surface flora). Treatment: urgent intravitreal antibiotics (vancomycin + ceftazidime or amikacin) with or without intravitreal steroids. The Endophthalmitis Vitrectomy Study (EVS) showed: patients with hand motion (HM) or worse vision benefit from pars plana vitrectomy + antibiotics vs intravitreal antibiotics alone; those with better than HM vision do equally well with intravitreal antibiotics alone.
5. Wound Leak (Filter Bleb / Aqueous Leakage): Positive Seidel test (fluorescein leaks from wound with blue light) indicates wound dehiscence. Managed by pressure patch; surgical re-suturing if not self-resolving.
Late Complications:
6. Posterior Capsular Opacification (PCO): The commonest late complication — occurs in 20–40% of patients within 2–5 years. Residual equatorial lens epithelial cells proliferate and migrate across the posterior capsule, causing Elschnig pearl formation and fibrous metaplasia. Presents with gradual blurring and glare — identical in character to the original cataract. Treated definitively by Nd:YAG laser capsulotomy (outpatient, painless, takes 5 minutes) — a laser creates a central aperture in the posterior capsule. NOT a second surgery.
7. Cystoid Macular Oedema (CMO / Irvine-Gass Syndrome): Fluid accumulation in the macula (petaloid pattern on fluorescein angiography/OCT) — related to prostaglandin-mediated inflammation and vitreous incarceration in the wound. Occurs weeks to months post-operatively; causes central visual blurring despite an apparently good surgical outcome. Treated with topical NSAIDs (ketorolac, bromfenac), steroids, and intravitreal anti-VEGF in refractory cases.
8. IOL Dislocation: Late decentration or dislocation of the IOL into the vitreous — from zonular dehiscence, weak capsular bag contraction, or inadequate capsular support at surgery. Requires surgical repositioning or IOL exchange.
9. Refractive Surprise: Unexpected post-operative refractive error (myopia, hypermetropia, or astigmatism) from biometry error, incorrect formula selection, or surgically induced astigmatism. Managed with spectacle correction; persistent significant error may require IOL exchange or laser refractive surgery.