Page 1 of 23
OP8.1-2 | Lens Anatomy and Cataract Pathogenesis — SDL Guide
Learning Objectives
- Describe the surgical anatomy of the lens including its layers, dimensions, vascularity, and attachments
- Explain the metabolic basis of lens transparency and the mechanisms by which opacity develops
- Classify cataract by aetiology, morphology, and stage of maturation
- Describe the clinical features at each stage of senile cataract maturation
- Enumerate the complications of cataract
- Outline the diagnostic workup and management principles for cataract
INSTRUCTIONS
Cataract — opacity of the crystalline lens — is the single largest cause of reversible blindness in India, and your understanding of its anatomy and pathogenesis is the foundation for every clinical decision from diagnosis through surgical planning. This module builds from the microscopic structure of the lens to the clinical spectrum of cataract, covering classification, maturation stages, and complications that you will recognise and manage throughout your surgical career.
References
- Khurana AK. Comprehensive Ophthalmology, 7th edition. New Age International. Chapter 7: Diseases of the Lens. (textbook)
- Parson JH. Diseases of the Eye, 22nd edition. CBS Publishers. Chapter 8: Cataract. (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Mr. Ramasamy, a 68-year-old farmer from rural Tamil Nadu, visits the ophthalmology outpatient department with his daughter. Over the past three years, he has noticed gradual blurring of vision in both eyes — worse in sunlight, and now so severe that he can no longer recognise faces or work in the fields. He has no pain, no redness, and no history of injury. On examination, his visual acuity is 2/60 in the right eye and counting fingers at 1 metre in the left. There is no red reflex in the left eye, but the right shows a dull, hazy red reflex. This is a case of bilateral senile cataract — the leading cause of preventable blindness worldwide and the most common indication for ophthalmic surgery in India. Before you can counsel, operate, or counsel the family, you must understand exactly what you are operating on.
WHY THIS MATTERS
Cataract surgery is the highest-volume elective surgical procedure performed in India, with over 6 million surgeries performed annually under the National Programme for Control of Blindness and Visual Impairment (NPCBVI). Every medical graduate will encounter patients with cataract in any clinical setting — primary care, casualty, or specialist outpatient. Understanding lens anatomy is not academic: it directly determines surgical approach, IOL selection, anaesthetic technique, and the recognition of complications such as phacolytic glaucoma or posterior capsular rupture. A firm grasp of classification and maturation stages allows you to triage urgency, explain the condition to patients in plain language, and detect sight-threatening complications before they become irreversible.
RECALL
Before we explore the lens, recall what you learned in anatomy: the eyeball contains three tunics and three chambers. The crystalline lens sits between the posterior chamber anteriorly and the vitreous cavity posteriorly, suspended by the zonule of Zinn (suspensory ligament), which runs from the ciliary body to the lens equator. The lens is a biconvex, avascular, transparent structure. In physiology, you learned that the lens contributes approximately +18 to +20 dioptres of the eye's total refracting power (~+60D) and is responsible for accommodation through ciliary muscle contraction (changing lens curvature). In biochemistry, you encountered crystallin proteins as the principal structural proteins of the lens. These foundations are now brought into clinical focus.
Clinical Presentation of Cataract
Cataract presents insidiously, and the clinical history is as important as the slit-lamp examination in establishing the diagnosis and its functional impact. The cardinal symptom is progressive, painless blurring of vision — the gradual onset distinguishes cataract from acute causes of visual loss such as retinal detachment or vascular occlusion. Patients frequently describe difficulty in dim light (nuclear cataract preferentially impairs scotopic vision early), problems with bright light and glare (posterior subcapsular cataracts are notoriously glare-sensitive), and reduced ability to read small print or recognise faces at a distance depending on whether the cataract is predominantly nuclear or cortical.
A characteristic early symptom of nuclear cataract is myopic shift — the increasing refractive index of the hardening nucleus creates a temporary "second sight" in presbyopic patients who find they can read without spectacles again. This apparent improvement masks progressive nuclear sclerosis and should not reassure either the patient or the clinician. Monocular diplopia or polyopia (multiple ghost images from a single eye) may also occur as irregular refractive changes develop across the lens.
Red flag symptoms that mandate urgent evaluation beyond cataract: sudden loss of vision, pain, redness, or photophobia — these point to concurrent pathology (acute glaucoma, uveitis, vitreous haemorrhage) that must not be attributed to cataract alone. The clinical history should also capture the impact on daily activities — driving, reading, occupational tasks — as functional impairment, not visual acuity alone, determines the timing of surgical intervention.
Surgical Anatomy of the Lens
The crystalline lens is a remarkable biological structure — biconvex, transparent, avascular, and devoid of nerve supply — that must maintain absolute optical clarity throughout life. Understanding its architecture is essential for the surgeon who must navigate it layer by layer. The lens in an adult measures approximately 9–10 mm in equatorial diameter and 4–5 mm in axial thickness (increasing with age). It is housed within an elastic lens capsule (thickest at the anterior midperiphery, ~14 µm; thinnest at the posterior pole, ~2–4 µm), which serves as the basement membrane of the lens epithelium and an important boundary during surgery.
Beneath the anterior capsule lies a single layer of cuboidal cells, the lens epithelium — the only mitotically active component of the adult lens. Epithelial cells at the equatorial region (the germinative zone or bow region) continuously divide and differentiate, migrating posteriorly to form new lens fibres. These lens fibres are tightly packed, elongated cells that have lost their nuclei and organelles to maximise transparency; their junctions form a characteristic suture pattern (Y-anteriorly, inverted Y-posteriorly). The lens has three main optical zones: the cortex (outermost, softer, newly formed fibres), the adult nucleus (denser, formed from adolescent lens fibres), and the more compacted fetal nucleus and embryonic nucleus at the centre.
The lens is avascular — it receives all nutrition (glucose, amino acids) and removes metabolic waste exclusively through the aqueous humour that bathes it. This avascular nature means that any disruption to aqueous circulation or lens capsule integrity immediately threatens lens metabolism. The lens is attached to the ciliary body by the zonular fibres (fibres of Zinn), which insert into the equatorial capsule and function as the tension-transmitting mechanism for accommodation.
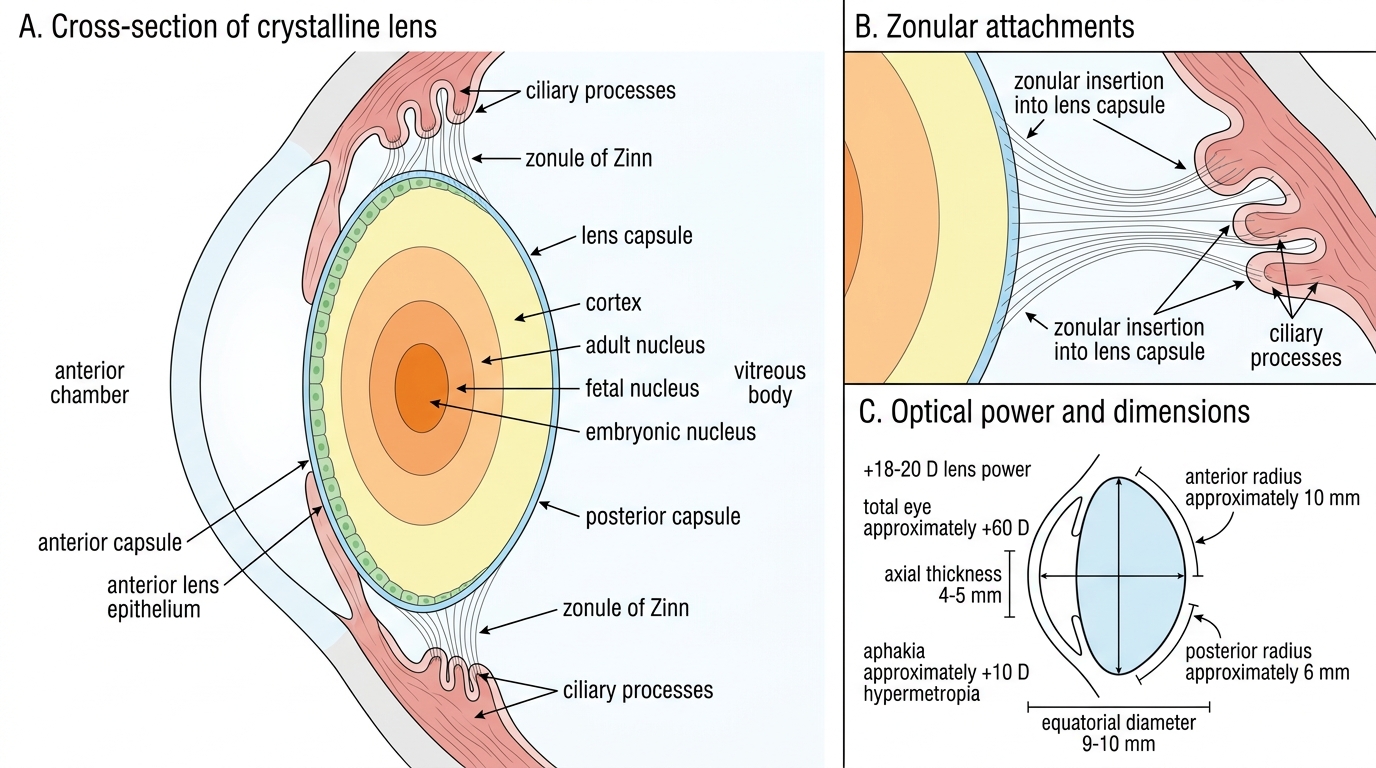
Human Lens: Cross-Section, Zonules, and Optical Significance
Refractive contribution: The lens contributes approximately +18–20 dioptres to the total refracting power of the eye (~+60D). The anterior cornea provides about +43D. Removal of the lens during cataract surgery therefore leaves the eye profoundly hypermetropic (aphakia, ~+10D), which must be corrected by an intraocular lens (IOL) implant.
Key dimensions (for surgical planning):
- Axial length: ~4–5 mm (increases with age, nuclear sclerosis)
- Equatorial diameter: ~9–10 mm
- Anterior radius of curvature: ~10 mm; posterior: ~6 mm
Lens Metabolism and Transparency Maintenance
Lens transparency depends on an exquisitely regulated biochemical environment. Unlike most tissues, the lens has almost no blood supply and must maintain low water content, high protein concentration, and minimal light scatter — all simultaneously, for a lifetime. Understanding these mechanisms explains how cataract develops at the molecular level.
The principal structural proteins of the lens are the crystallins — alpha (α), beta (β), and gamma (γ) crystallins in humans. α-crystallin also functions as a molecular chaperone, preventing aggregation of damaged proteins. In a healthy lens, crystallin proteins are arranged in an orderly short-range spatial pattern that minimises light scatter. Cataract begins when crystallin proteins denature, aggregate, or are modified (by oxidation, glycation, UV radiation, or enzyme defects), disrupting this ordered packing and creating refractive index variations that scatter light.
The lens uses anaerobic glycolysis (Embden–Meyerhof pathway) as its primary energy source, producing ATP for the Na⁺/K⁺-ATPase pump that maintains the low intracellular sodium and relatively dehydrated state of lens fibres. A small proportion of metabolism proceeds via the sorbitol pathway (aldose reductase converts glucose to sorbitol) — critically important in diabetic cataract, where hyperglycaemia drives excess sorbitol accumulation, osmotic swelling of the lens fibres, and subsequent cataract formation. Similarly, galactosaemia (galactitol accumulation) causes early childhood cataract via the same mechanism.
Reduced glutathione is the principal antioxidant in the lens, protecting against oxidative damage from UV radiation and metabolic free radicals. Decreased glutathione levels — seen with age, UV exposure, and malnutrition — predispose to nuclear sclerosis and cortical cataract. Vitamin C (ascorbic acid) is present in high concentrations in aqueous humour and also plays an antioxidant role.
The lens epithelium is the metabolic powerhouse: it synthesises proteins, maintains ionic gradients, and controls water content. Damage to epithelial cells (trauma, radiation, inflammation) directly leads to posterior subcapsular cataract. After extracapsular surgery, residual equatorial epithelial cells can migrate, proliferate, and lay down fibrous metaplastic tissue — the basis of posterior capsular opacification (PCO), the commonest late complication of cataract surgery.