Page 2 of 23
OP8.1-2 | Lens Anatomy and Cataract Pathogenesis — SDL Guide (Part 2)
Aetiology and Classification of Cataract
Cataract is not a single disease but a syndromic endpoint reached by many aetiological pathways. Understanding its classification is fundamental to clinical reasoning: the cause of a cataract determines its morphological pattern, guides the pace of investigation, and — crucially — may reveal a treatable systemic disease. For example, a bilateral posterior subcapsular cataract in a young patient should prompt enquiry about corticosteroid use, diabetes, or atopic disease, not simply referral for surgery. A systematic classification also communicates meaningfully across clinical settings and prevents the diagnostic error of assuming that all cataract is senile in origin. The most clinically useful framework classifies cataract first by aetiology, then further by morphological location within the lens (nuclear, cortical, posterior subcapsular) and by stage of maturation. Each level of classification carries clinical implications that you will be expected to apply at the bedside and in examination settings.
Provided image
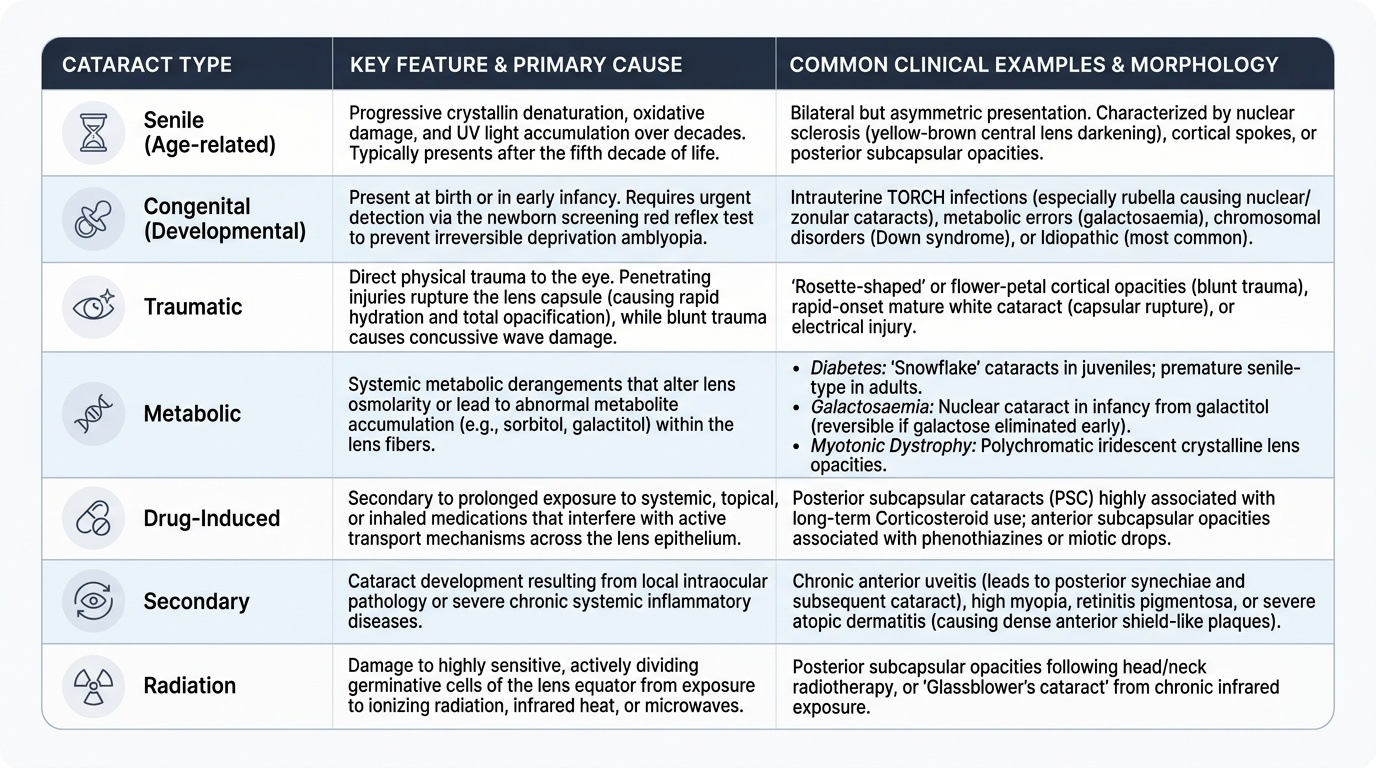
A. By Aetiology:
- Senile (age-related) cataract — the commonest type globally, caused by progressive crystallin denaturation, oxidative damage, and UV accumulation over decades. Bilateral but typically asymmetric. Presents after the fifth decade.
- Congenital (developmental) cataract — present at birth or in early infancy; must be detected by the newborn screening red reflex test and treated urgently to prevent deprivation amblyopia. Causes include: intrauterine TORCH infections (especially rubella — nuclear/zonular cataract), metabolic disorders (galactosaemia, hypoglycaemia), chromosomal abnormalities (Down syndrome, Turner syndrome), and idiopathic (most common). Can be unilateral or bilateral.
- Traumatic cataract — penetrating eye injury (posterior subcapsular opacity, rosette pattern with blunt trauma) or perforating injury with capsular rupture (rapid total lens opacification due to aqueous entry). Electrical injury and ionising radiation also cause this type.
- Metabolic cataract — three main subtypes: Diabetic cataract (sorbitol accumulation causing true diabetic snowflake cataract in juveniles; adults develop premature senile-type); Galactosaemic cataract (nuclear cataract in infancy from galactitol — reversible if galactose eliminated early); Myotonic dystrophy (polychromatic iridescent crystalline lens opacities — 'Christmas tree' cataract).
- Drug-induced (toxic) cataract — Corticosteroids (especially systemic long-term; also topical) cause posterior subcapsular cataract (PSC). Chlorpromazine (phenothiazines) causes anterior subcapsular stellate deposits. Busulfan and amiodarone also implicated.
- Secondary (complicated) cataract — occurs as a complication of ocular disease: chronic anterior uveitis (PSC, most common secondary cataract), retinitis pigmentosa (PSC), glaucoma, hypotony, intraocular tumours, and high myopia (premature nuclear sclerosis).
- Radiation cataract — X-rays, gamma rays, neutrons cause PSC; UV radiation contributes to cortical and nuclear cataract.
B. By Morphological Type (Senile Cataract): Nuclear, Cortical, Posterior subcapsular — each with distinct clinical impact (covered in the next section).
B. By Stage of Maturation: Immature, Mature, Hypermature — clinically critical for surgical timing and complication recognition (next section).
SELF-CHECK
A 6-month-old infant is found to have absent red reflex in the right eye on routine screening. The most likely diagnosis is:
A. Congenital cataract
B. Retinoblastoma
C. Persistent hyperplastic primary vitreous
D. Any of the above — absent red reflex in an infant requires urgent ophthalmic evaluation
Reveal Answer
Answer: D. Any of the above — absent red reflex in an infant requires urgent ophthalmic evaluation
Absent red reflex in an infant is always an ophthalmic emergency. While congenital cataract is a common cause, retinoblastoma and persistent hyperplastic primary vitreous (PHPV) must also be excluded. All require urgent specialist referral — this is the basis of the national newborn eye screening programme.
Stages of Maturation of Senile Cataract
Senile cataract does not appear suddenly — it progresses through distinct clinically recognisable stages, each with characteristic slit-lamp findings, functional impairment, and surgical implications. This maturation sequence is particularly important in India and other developing regions where patients present late, often with advanced cataracts that carry higher surgical risk. The staging framework, based on Khurana's clinical classification, allows the clinician to predict the surgical difficulty, counsel the patient about visual prognosis, and time the intervention appropriately. An immature cataract presenting with good red reflex and partial cortical opacity is technically easier to remove by phacoemulsification than a mature or hypermature (Morgagnian) cataract with a fully opacified lens and absent red reflex. Staging also determines whether fundoscopy is possible: a clear red reflex means the posterior segment can be assessed, while its absence — as in a mature or hypermature cataract — necessitates B-scan ultrasonography to exclude retinal detachment or vitreous pathology before surgery.
Provided image
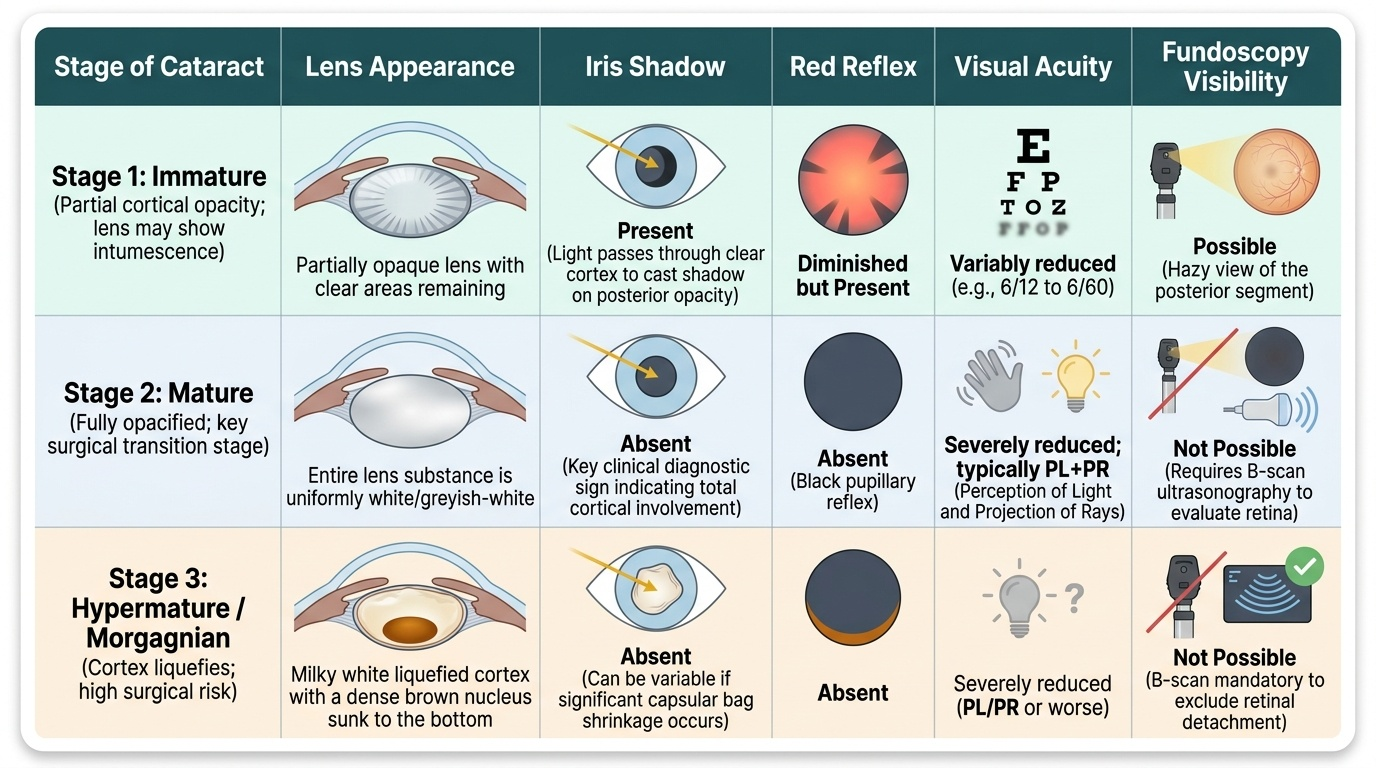
Stage 1 — Immature (Incipient) Cataract: The lens is partially opaque; clear areas remain. The lens may show intumescence (water absorption causing the lens to swell). An iris shadow is present — the shadow of the iris falls on the opaque posterior part of the lens when light is shone from the side, because the anterior lens cortex remains clear. The red reflex is diminished but present. Visual acuity is variably reduced. This is the most common stage encountered in practice.
Stage 2 — Mature Cataract: The entire lens is opaque — uniformly white or greyish-white. No iris shadow (all lens substance is equally opaque, so the iris shadow is absent — this is the key clinical sign distinguishing mature from immature). Red reflex is absent — no light passes through to the retina, so fundoscopy is not possible. Visual acuity is severely reduced, typically to perception of light (PL) with accurate projection of rays (PR). The posterior capsule remains intact. The patient often reports that their previously dim vision has become slightly 'clearer' than in the late immature stage — this is because the fully opaque lens scatters less light than the swollen intumescent one.
Stage 3 — Hypermature Cataract: The lens proteins liquify (degenerate), forming a milky white fluid (the cortex). The nucleus, being denser, sinks inferiorly due to gravity — this is called a Morgagnian cataract (named after Morgagni who first described it). The lens capsule may become wrinkled or shrunken as the liquid cortex leaks out. No iris shadow, absent red reflex. This stage carries significant danger: the liquefied lens proteins can leak through the intact capsule into the anterior chamber, triggering a macrophage-mediated inflammatory response and secondary phacolytic glaucoma. Immediate surgery is warranted.
Summary of key differentiating signs:
- Iris shadow: Present (immature) → Absent (mature) → Absent (hypermature)
- Red reflex: Reduced (immature) → Absent (mature) → Absent (hypermature)
- Lens appearance: Partial opacity (immature) → Uniformly white (mature) → Milky/shrunken with sunken nucleus (Morgagnian)
Morphological Types and Their Clinical Significance
The morphological location of lens opacity determines the pattern of visual disturbance a patient experiences and guides the clinical suspicion of the underlying cause. There are three principal morphological types in senile cataract.
1. Nuclear Cataract (Nuclear Sclerosis): The earliest and most common type in ageing lenses. The nucleus progressively hardens (sclerosis) and develops yellowish-brown discolouration (brunescence). In early stages, increased refractive index of the nucleus may cause myopic shift — the patient finds they can read without their reading glasses ('second sight' of the elderly, though this is not truly an improvement but a refractive change). Nuclear cataract causes predominantly distance vision impairment, while near vision may be temporarily preserved. Slit-lamp examination reveals a dense, amber-to-brown nucleus; retroillumination shows a central opacity.
2. Cortical Cataract: Begins as radial spoke-like opacities (cuneiform opacities) at the equatorial cortex, progressing toward the visual axis. Patients complain of glare, particularly with oncoming headlights (photophobia) and difficulty in bright sunlight. Both distance and near vision are affected. Cortical cataract is associated with UV exposure and dehydration. On slit-lamp: characteristic spoke-wheel pattern, best seen with retroillumination.
3. Posterior Subcapsular Cataract (PSC): Forms just anterior to the posterior capsule, at the visual axis. PSC causes disproportionately severe visual impairment for its size because it directly obstructs the centre of the visual axis. Patients complain of marked glare and difficulty reading. Near vision is typically more affected than distance vision because the pupil constricts during near fixation, concentrating light through the opacity. PSC is the morphological type most associated with steroid use (systemic or topical), diabetes mellitus, uveitis, and retinitis pigmentosa. The slit-lamp shows a granular, 'bread-crumb' appearance at the posterior pole.
Clinical tip: A young patient (30s–40s) with PSC should prompt active inquiry about steroid use, systemic disease, or prior ocular inflammation — this is not a 'senile' pattern.
CLINICAL PEARL
The iris shadow test is clinically decisive. When examining a cataract patient with a pen torch held temporally: presence of a crescentic shadow of the iris on the lens = immature cataract (anterior cortex still clear, allowing the iris to cast a shadow on the posterior opaque part). Absence of iris shadow = mature (entire lens opaque, no shadow possible) OR absent lens (aphakia, pseudophakia). This bedside sign takes 5 seconds and provides immediate staging information even without slit-lamp equipment — crucial in primary care settings.
A second clinical pearl: steroid-induced cataract is always posterior subcapsular in location. If you see a young patient with PSC, do not accept 'early senile' — ask specifically about steroid use (oral, inhaled, topical ophthalmic, or high-dose topical skin creams). The dose and duration threshold is variable; even inhaled steroids over years can cause PSC.