Page 1 of 26
OR1.1 | Pre-hospital Trauma Care and Emergency Room Triage — SDL Guide
Learning Objectives
- Describe the principles of pre-hospital trauma care including the 'platinum ten minutes' and primary survey priorities
- Explain the components of Advanced Trauma Life Support (ATLS) primary and secondary surveys
- Apply the START triage algorithm to classify multiple-casualty patients into priority categories
- Outline the ABCDE approach for initial stabilisation of the trauma victim in the emergency room
- Discuss the concept of damage control resuscitation and its rationale in haemorrhagic shock
INSTRUCTIONS
Road traffic injuries and falls are among the leading causes of disability and death in India. For final-year medical students who will work in district hospitals, emergency departments, and primary health centres, understanding the initial management of trauma is not optional — it is a survival skill for your patients. This module grounds you in the global standard framework, ATLS, and shows you how triage decisions made in the first few minutes determine whether a patient reaches definitive care alive. The principles you learn here directly connect to your clinical postings in orthopaedics, surgery, and emergency medicine.
References
- Maheshwari's Essential Orthopaedics, Chapter 1 — Trauma and its Management (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, Chapter 22 — Principles of Fractures (textbook)
- ATLS Student Course Manual, 10th edition, American College of Surgeons Committee on Trauma (guideline)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
At 11 PM, a call comes in to the district hospital: a mini-bus has overturned on the highway, and twelve people are en route. You are the only doctor on duty. Three minutes later, the first ambulance arrives. One patient is unconscious with an obvious deformed femur, gurgling breathing, and a bleeding scalp wound. The second has a painful abdomen and a BP of 80/50. The third is screaming in pain with a deformed wrist but appears haemodynamically stable. Who do you treat first? What do you do in the first sixty seconds? The answer to these questions is not instinct — it is a system, and it is called ATLS.
WHY THIS MATTERS
Trauma is the leading cause of death in Indians aged 15–44 years, and the majority of preventable trauma deaths occur in the first hour — the so-called 'golden hour.' Most district hospitals in India lack trauma surgeons, neurosurgeons, or dedicated trauma teams. The final-year MBBS doctor is therefore frequently the first and only physician to evaluate the multiply-injured patient. Understanding the ATLS framework, triage principles, and the physiological priorities of initial resuscitation equips you to make the highest-yield interventions in the shortest time, buying the patient the window needed to reach a tertiary centre.
RECALL
Before proceeding, briefly recall the following from your prior learning:
- The ABCDE approach (Airway, Breathing, Circulation, Disability, Exposure) as a systematic examination sequence
- The physiology of haemorrhagic shock: what happens to heart rate, blood pressure, and tissue perfusion when blood volume decreases
- The difference between a closed and open fracture, and why soft tissue integrity matters
- Basic anatomy of the thorax relevant to a tension pneumothorax (mediastinal shift, tracheal deviation)
- The Glasgow Coma Scale (GCS) components and its range (3–15)
The Golden Hour and Trimodal Distribution of Trauma Deaths
The concept of the golden hour was introduced by R Adams Cowley in the 1970s, arising from the observation that trauma patients who reached definitive surgical care within sixty minutes of injury had dramatically better survival than those who did not. While the 'one hour' is now understood to be a metaphor for urgency rather than a precise biological window, the concept remains clinically powerful: the speed with which airway, breathing, and circulation are stabilised determines whether the patient reaches the operating theatre or the morgue.
Trimodal distribution of trauma deaths (originally described by Trunkey) identifies three peaks of death after injury. The first peak occurs within seconds to minutes of injury, typically from devastating neurological or vascular injuries (aortic transection, high-level spinal cord injury) — these are rarely salvageable. The second peak occurs minutes to hours after injury and represents the group where pre-hospital care and the emergency room response matter most: expanding intracranial haematoma, tension pneumothorax, haemoperitoneum, and haemorrhage from major vessel or solid organ injury. The third peak occurs days to weeks later from multi-organ failure and sepsis, and is influenced by the quality of in-hospital care. The ATLS system is designed primarily to address second-peak deaths.
The platinum ten minutes is the pre-hospital analogue of the golden hour: the principle that the scene time for a trauma patient should be no more than ten minutes (for basic stabilisation and packaging), with rapid transport to the nearest appropriate facility. Prolonged scene time for definitive intervention is not appropriate in trauma — 'scoop and run' supersedes 'stay and play' for the majority of serious trauma cases.
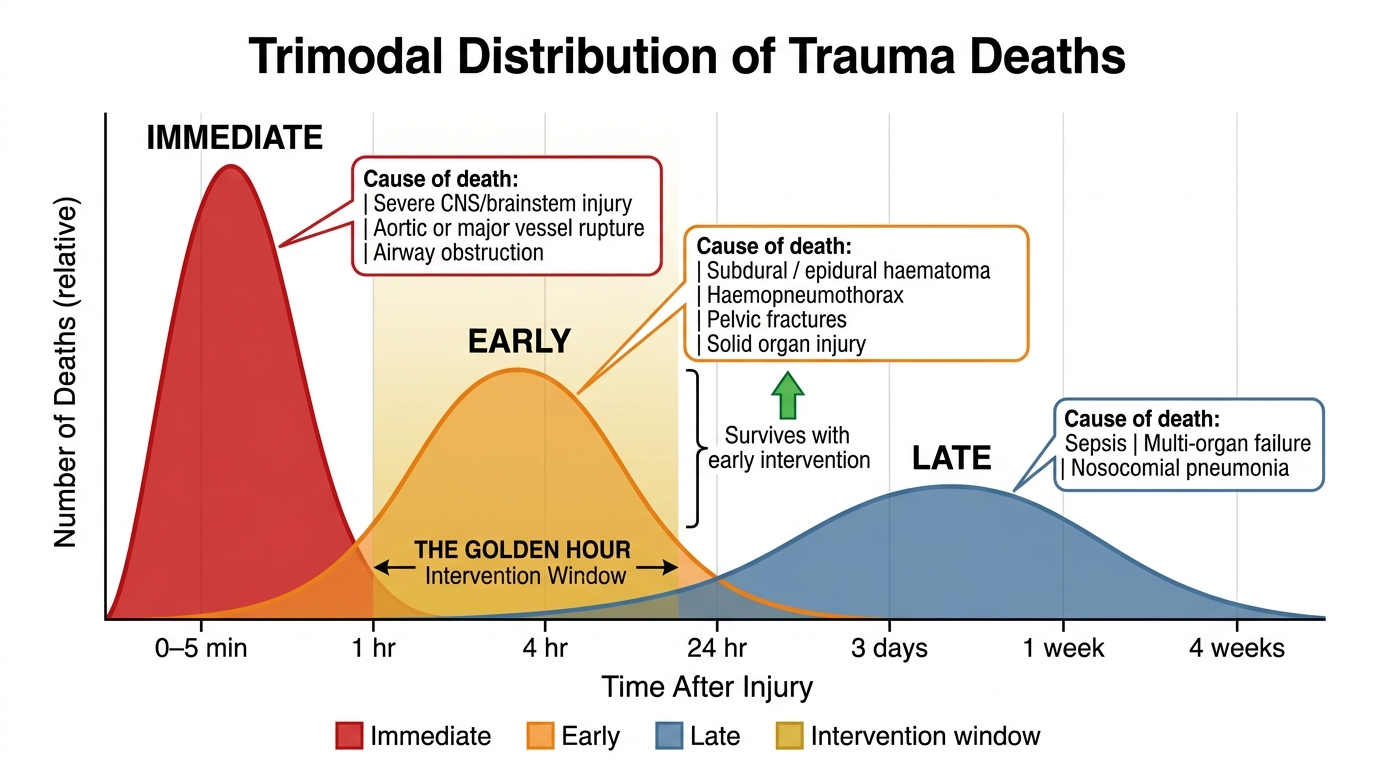
Trimodal Distribution of Trauma Deaths and the Intervention Window
The practical implication is that pre-hospital teams should focus on three things at the scene: controlling external haemorrhage (tourniquet, wound packing), maintaining a patent airway (jaw thrust, airway adjunct), and rapidly transporting the patient. Intravenous access and fluid administration en route are acceptable; complex procedures at the scene are not.
Pre-hospital Trauma Care: Principles and Protocols
Pre-hospital trauma care encompasses all interventions delivered from the moment of injury until the patient arrives at a receiving hospital. The quality of this phase of care is highly variable in India, ranging from advanced paramedic-run ambulance services in metropolitan areas to basic first-aid applied by bystanders in rural settings. Regardless of the level of provider, the principles remain constant and are grounded in an understanding of which physiological derangements kill patients most rapidly.
Mechanism of injury is the first piece of information pre-hospital providers should document and communicate to the receiving hospital. High-energy mechanisms — falls from height greater than three metres, high-speed road traffic collisions, blast injuries, penetrating trauma to the torso — trigger a higher index of suspicion for occult injuries and mandate a more thorough evaluation. Low-energy mechanisms in elderly patients can still cause serious injury (a ground-level fall can fracture the proximal femur or cause a subdural haematoma in an anticoagulated patient).
Spinal precautions in the pre-hospital setting have evolved considerably. Traditional teaching mandated rigid cervical collar and spinal board for all trauma patients. Current evidence suggests that universal spinal immobilisation in penetrating trauma actually increases mortality (delays to resuscitation) and that clinical decision tools (NEXUS criteria, Canadian C-spine Rule) should guide selective immobilisation. However, in the absence of validated triage tools or for unconscious patients with unknown mechanism, maintaining spinal precautions is still appropriate in the Indian pre-hospital context.
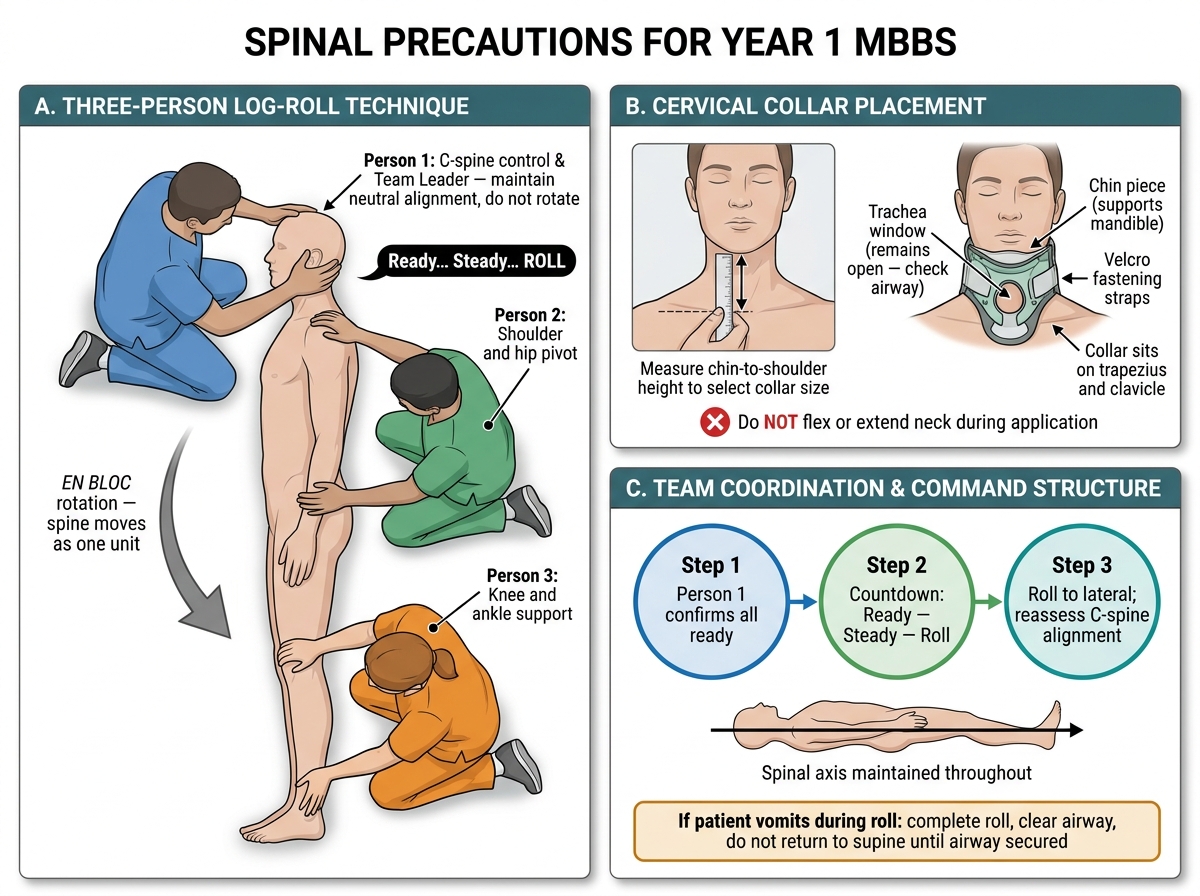
Spinal Precautions: Cervical Collar Application and Three-Person Log-Roll Technique
Haemorrhage control remains the most impactful pre-hospital intervention. Direct pressure, wound packing (for junctional wounds), and tourniquet application for extremity haemorrhage are all within the scope of basic first responders. The 'haemostatic triangle' concept teaches that three concurrent problems — hypothermia, acidosis, and coagulopathy — form a lethal triad that worsens once established; halting haemorrhage at the earliest opportunity interrupts this cascade before it begins.
| Pre-hospital intervention | Priority level | Acceptable time | Notes |
|---|---|---|---|
| Airway opening (jaw thrust, adjunct) | Immediate | <1 min | Head tilt-chin lift contraindicated if C-spine injury suspected |
| External haemorrhage control | Immediate | <2 min | Tourniquet for limb, pack-and-pressure for torso |
| Spinal immobilisation | High | <5 min | Selective based on mechanism + conscious state |
| IV access + fluids | Moderate | En route | Do not delay transport for IV access |
| Splinting of fractures | Low | En route | Reduces pain and blood loss from femoral shaft fractures |
Triage: Principles and the START System
Triage (from the French trier, to sort) is the process of systematically categorising patients in a mass-casualty or multi-casualty incident to maximise overall survival when resources are overwhelmed. The fundamental ethical shift in triage is from individual patient advocacy to utilitarian population-level benefit: the most severely injured patient who cannot survive with available resources does not receive priority over the many with survivable injuries who will die without treatment.
The START (Simple Triage and Rapid Treatment) algorithm is the most widely used initial triage tool for mass-casualty incidents. It was developed in the United States in the 1980s and uses three physiological parameters — respiratory status, perfusion (radial pulse or capillary refill), and mental status (ability to follow commands) — to sort patients into four colour-coded categories in approximately 30 seconds per patient.
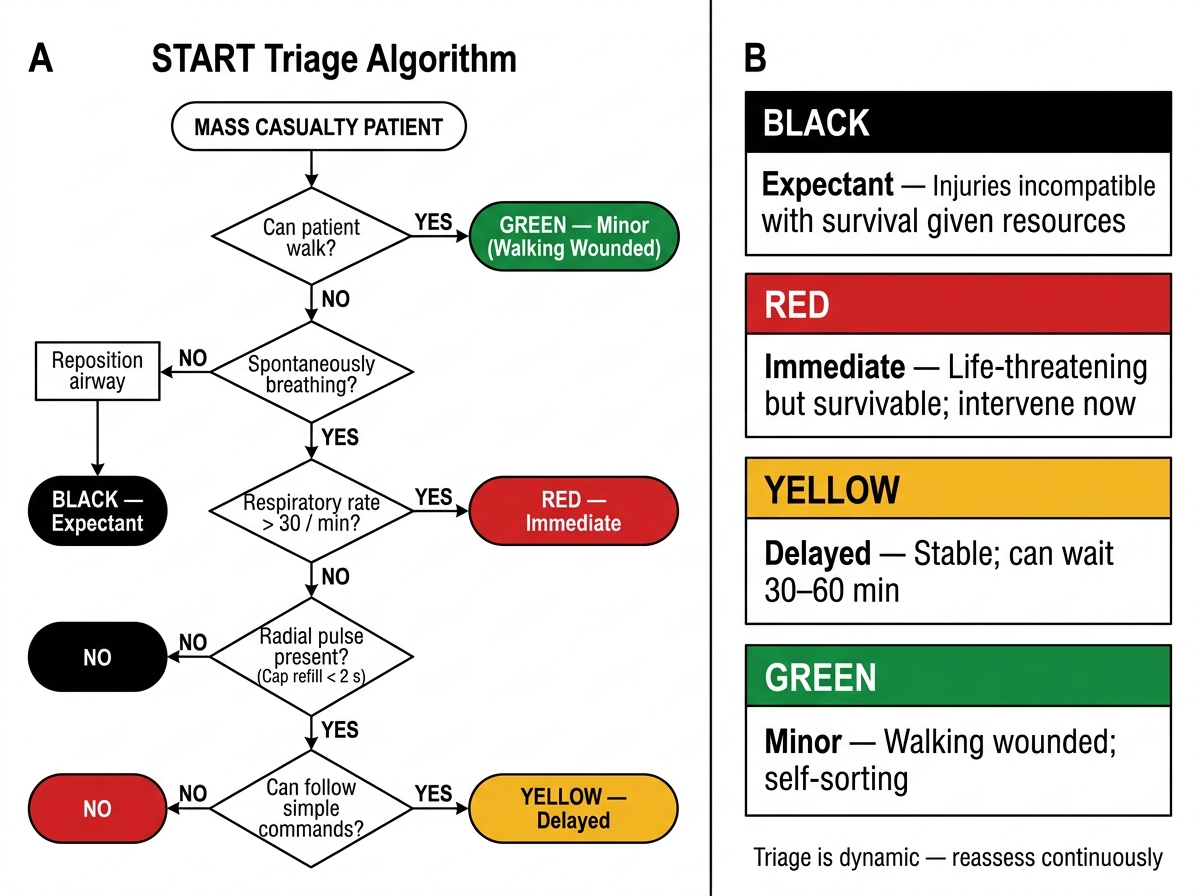
START Mass-Casualty Triage Algorithm
The four START categories are:
- Black (expectant): not breathing after one attempt to reposition airway, or respiratory rate >30 AND no radial pulse AND unable to follow commands. These patients have injuries incompatible with survival given available resources.
- Red (immediate): requires immediate intervention to survive — typically airway compromise, respiratory rate >30 with maintained perfusion, or altered mental status with otherwise survivable physiology.
- Yellow (delayed): has survivable injuries but is physiologically stable; can wait 30–60 minutes for treatment without deterioration.
- Green (minor): the 'walking wounded' — ambulatory, communicating, able to follow commands. These patients sort themselves first.
In secondary triage at the emergency room, the SALT (Sort, Assess, Lifesaving Interventions, Treatment/Transport) algorithm or hospital-based triage systems are applied. An important principle is that triage is dynamic — a green patient who develops haemodynamic instability must be re-triaged.
The mass-casualty incident (MCI) response requires activation of a hospital disaster plan, designation of a triage officer (typically the most senior clinician who does NOT begin treating individual patients), establishment of a treatment area with separate immediate and delayed zones, and communication with a receiving hospital network to distribute patients equitably.
| Triage colour | Status | Management | Example clinical scenario |
|---|---|---|---|
| Black | Expectant | Comfort only | Apnoeic after airway repositioning, no pulse |
| Red | Immediate | Treat within minutes | Tension pneumothorax, uncontrolled haemorrhage |
| Yellow | Delayed | Treat within hours | Closed femur fracture, stable vitals |
| Green | Minor | Self-care or basic first aid | Superficial lacerations, minor contusions |
SELF-CHECK
A patient in a bus crash is not breathing after you open the airway. Under START triage, you correctly reposition the airway but the patient remains apnoeic. What triage category does this patient receive?
A. Red (Immediate)
B. Yellow (Delayed)
C. Black (Expectant)
D. Green (Minor)
Reveal Answer
Answer: C. Black (Expectant)
Under START, a patient who does not begin breathing after a single attempt to open the airway is classified as Black (Expectant). The algorithm directs responders NOT to spend time on further airway manoeuvres in a mass-casualty scenario, to preserve those resources for patients with survivable injuries. This is the key utilitarian distinction of mass-casualty triage from individual patient care.