Page 2 of 26
OR1.1 | Pre-hospital Trauma Care and Emergency Room Triage — SDL Guide (Part 2)
ATLS Primary Survey: The ABCDE Approach
The Advanced Trauma Life Support (ATLS) programme, developed by the American College of Surgeons Committee on Trauma, provides a systematic, prioritised approach to the trauma patient based on the principle that the most immediately life-threatening problems are addressed first, in order of the speed with which they can kill. The sequence is not alphabetical convenience — it reflects the hierarchy of lethal physiology: a patient with a blocked airway dies faster than one with a haemothorax, who dies faster than one with an open fracture.
The primary survey uses the ABCDE sequence:
A — Airway with C-spine control: Assess and secure the airway while maintaining inline cervical spine stabilisation. Listen for stridor (supraglottic obstruction), observe for cyanosis and use of accessory muscles. Interventions escalate from jaw thrust/chin lift → suction of secretions/blood → oropharyngeal or nasopharyngeal airway → rapid sequence intubation (RSI) → surgical airway (cricothyroidotomy) if intubation fails. The rule is: if in doubt, secure the airway definitively.
B — Breathing and ventilation: Even a patent airway does not guarantee adequate ventilation. Inspect, palpate, percuss, and auscultate the chest. Detect and immediately treat: tension pneumothorax (needle decompression, 2nd intercostal space mid-clavicular line or 4th–5th ICS anterior axillary line; then intercostal drain), open pneumothorax (three-sided occlusive dressing), and massive haemothorax (intercostal drain + volume resuscitation).
C — Circulation with haemorrhage control: Assess haemodynamic status (heart rate, blood pressure, capillary refill, level of consciousness, urine output). Identify and control active bleeding. Establish large-bore intravenous access (two peripheral 16G cannulae minimum). The ATLS initial fluid resuscitation is 1 litre of warm crystalloid (Ringer's lactate preferred over normal saline for large volumes) as a bolus, followed by reassessment. Move rapidly to blood products (O-negative or type-specific) in patients who do not respond.
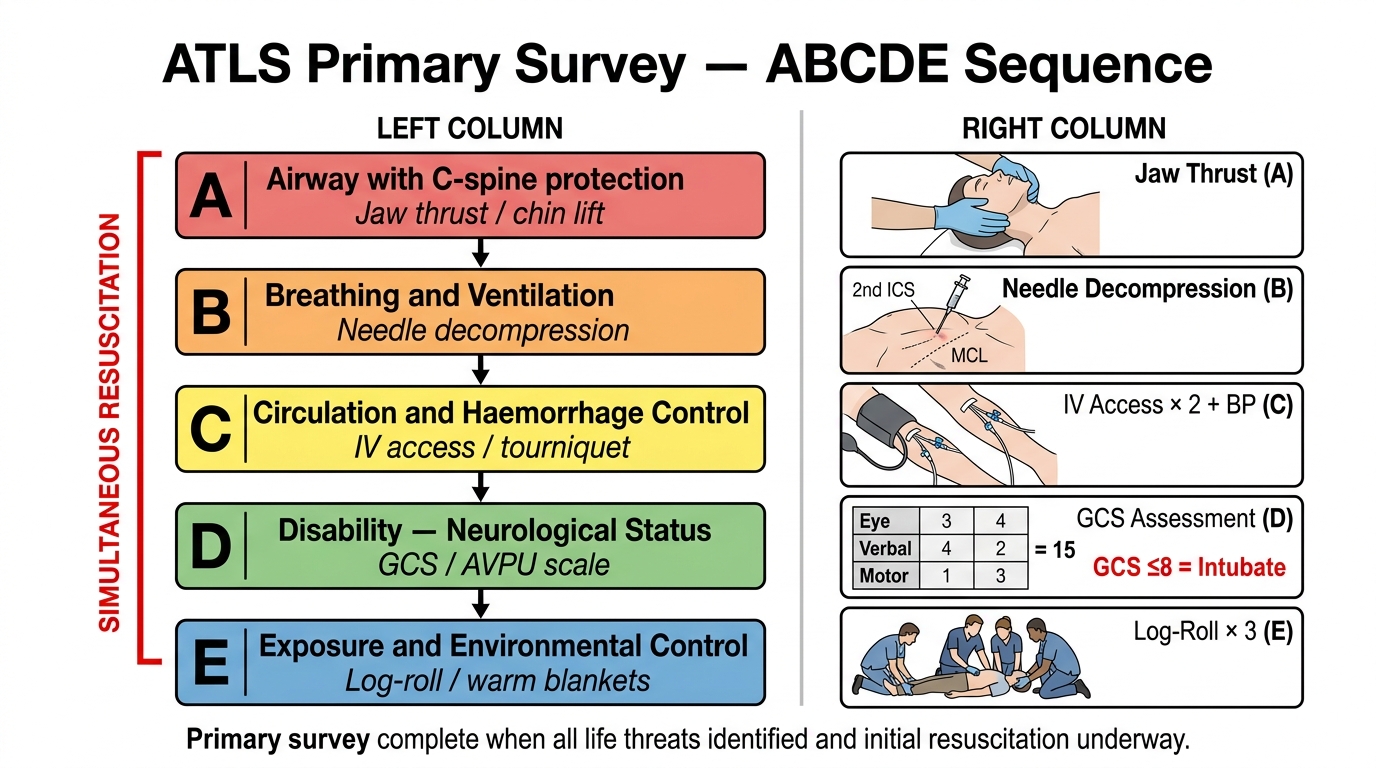
ATLS ABCDE Primary Survey Sequence with Key Interventions
D — Disability (Neurological status): Rapid neurological assessment using the AVPU scale (Alert, Voice responsive, Pain responsive, Unresponsive) or GCS. Pupillary response (size, symmetry, reaction). Lateralising signs (one-sided weakness, posturing). A GCS ≤8 defines coma and mandates airway protection.
E — Exposure and Environmental control: Fully undress the patient to detect occult injuries (posterior wounds, perineal injury, limb deformities). Immediately cover with warm blankets to prevent hypothermia. The log-roll (maintaining spinal alignment) examines the back. Place urinary catheter (if no urethral injury) and nasogastric tube.
Resuscitation occurs simultaneously with the survey. A team leader does not perform each step sequentially before treating — team members manage airway, breathing, and venous access in parallel. The primary survey is complete when all life threats have been identified and initial resuscitation is underway.
ATLS Secondary Survey and Adjuncts
The secondary survey begins only after the primary survey is complete and the patient is haemodynamically responding (or has been identified as requiring immediate operative intervention and should proceed directly to theatre). A secondary survey of a patient who is still haemodynamically compromised risks distracting from definitive management and must never be commenced prematurely. The secondary survey follows the primary survey's completion as a deliberately sequenced, not parallel, activity — this sequencing is a core ATLS teaching point that prevents the common error of 'finding an obvious injury and stopping the examination.'
The secondary survey is a head-to-toe examination with a complete history (AMPLE: Allergies, Medications, Past medical history, Last meal, Events/mechanism of injury), and systematic physical examination of every anatomical region. It aims to detect injuries not immediately life-threatening but clinically significant — facial fractures, thoracic spine fractures, urogenital trauma, peripheral nerve injuries, and all orthopaedic injuries.
Adjunct investigations during the primary survey:
- FAST (Focused Assessment with Sonography in Trauma): bedside ultrasound examining four windows (pericardial, right upper quadrant, left upper quadrant, pelvis) for free fluid. A FAST-positive haemodynamically unstable patient with abdominal or pelvic free fluid goes immediately to theatre.
- Chest X-ray: rapid portable AP view to detect haemothorax, pneumothorax, mediastinal widening (aortic injury), rib fractures.
- Pelvis X-ray: single AP pelvic view to detect open-book pelvic fractures, which can harbour massive retroperitoneal haemorrhage.
- ECG monitoring: for blunt cardiac injury detection (arrhythmias, right heart strain).
- Arterial blood gas (ABG): base deficit >-6 mEq/L suggests significant haemorrhage and underresuscitation.

FAST Examination: Four Acoustic Windows and Probe Positions
Following the secondary survey, further imaging is guided by clinical findings. CT scan of the head, chest, abdomen, and pelvis with contrast ('pan-scan') in haemodynamically stable patients with high-energy mechanisms has become standard in major trauma centres, significantly improving the detection of occult injuries.
A critical ATLS teaching point is the 'missed injury' — the most commonly missed injuries in trauma include posterior thoracic and lumbar spine fractures, diaphragmatic rupture, bladder injuries, and pelvic fractures without external clinical signs. The secondary survey and repeat examination (the 'tertiary survey' at 24 hours) systematically reduce this risk.
Damage Control Resuscitation and Damage Control Surgery
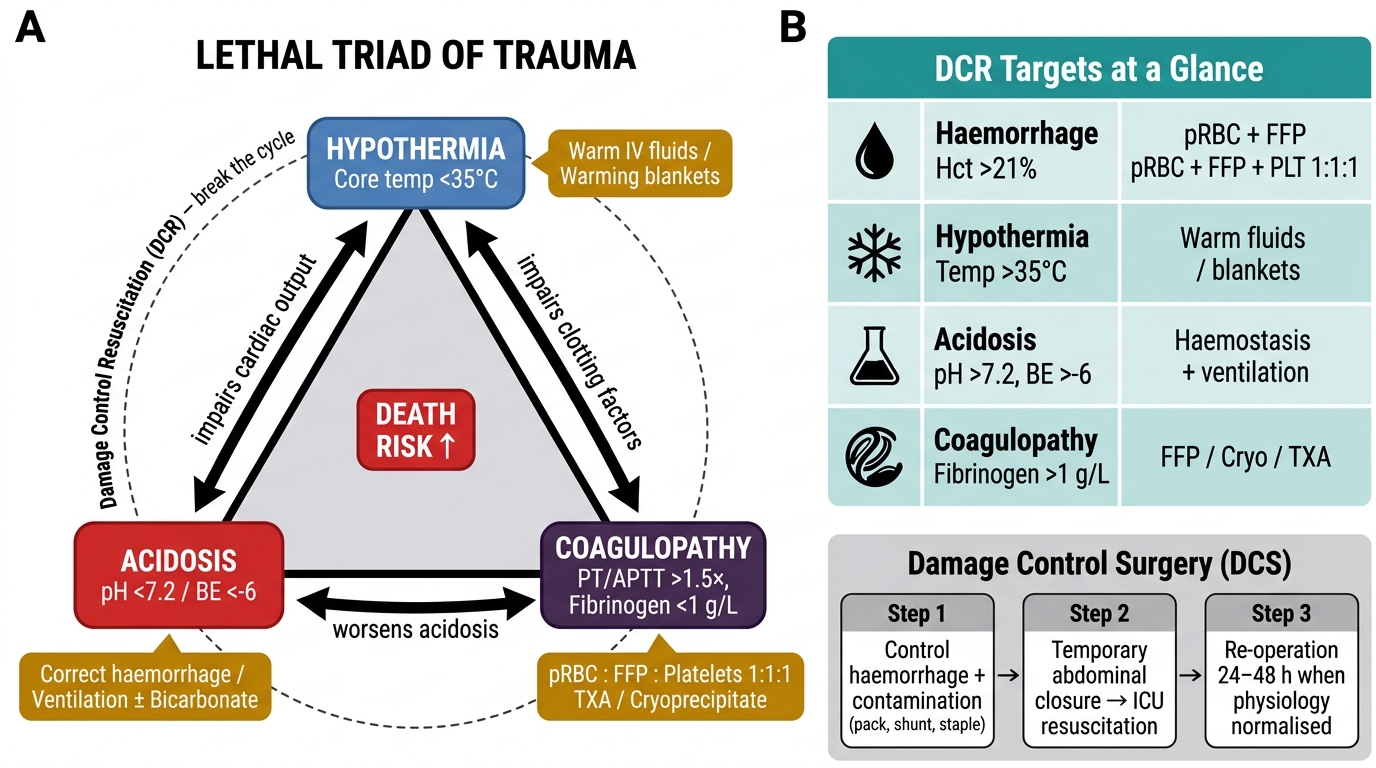
Damage control resuscitation (DCR) is a physiological strategy developed from military trauma experience that shifts the paradigm of resuscitation from 'normalise all parameters with crystalloid' to 'limit crystalloid, aggressively replace blood components, and tolerate permissive hypotension until haemorrhage is controlled.' The rationale emerges from understanding the lethal triad of trauma: coagulopathy, hypothermia, and acidosis. These three derangements form a self-reinforcing cycle — coagulopathy worsens haemorrhage, which worsens acidosis and hypothermia, which further impairs coagulation. Recognising this cycle early and interrupting it with targeted interventions is the essence of the damage control philosophy and separates modern trauma resuscitation from older volume-first approaches.
Large volumes of crystalloid (saline or Ringer's lactate), historically the first-line resuscitative fluid, contribute to dilutional coagulopathy, hypothermia (IV fluids at room temperature reduce core body temperature), and abdominal compartment syndrome from oedema. The current evidence-based approach, reflected in ATLS 10th edition, recommends:
- Haemostatic resuscitation: early fresh frozen plasma (FFP) + packed red blood cells (pRBC) + platelets in a balanced ratio (1:1:1 by units), mimicking whole blood.
- Permissive hypotension: accepting a systolic BP of 80–90 mmHg in penetrating trauma until surgical haemorrhage control is achieved (contraindicated in traumatic brain injury, where cerebral perfusion pressure must be maintained).
- Tranexamic acid (TXA): an antifibrinolytic that significantly reduces mortality in haemorrhagic trauma if given within 3 hours of injury (CRASH-2 trial, >20,000 patients). Dose: 1 g IV over 10 minutes, followed by 1 g over 8 hours.
The Lethal Triad of Trauma and Damage Control Resuscitation Targets
Damage control surgery (DCS) is the operative analogue: instead of performing a definitive complex repair in a haemodynamically unstable patient, the surgeon performs the minimum surgery to control haemorrhage and contamination (packing, vascular shunts, stapling bowel ends), closes the abdomen temporarily, and allows resuscitation in the ICU before planned re-operation in 24–48 hours when physiology has normalised. This staged approach saves patients who would not survive a prolonged single-stage operation.
| Physiological derangement | DCR target | Intervention |
|---|---|---|
| Haemorrhage / anaemia | Haematocrit >21%, ongoing haemostasis | pRBC + FFP + platelets 1:1:1 |
| Coagulopathy | PT/APTT <1.5× normal, fibrinogen >1 g/L | FFP, cryoprecipitate, TXA |
| Hypothermia | Core temp >35°C | Warm IV fluids, warming blankets, warm environment |
| Acidosis | pH >7.2, base excess >-6 | Correct by addressing haemorrhage + ventilation |
SELF-CHECK
A 28-year-old man is brought in after a stabbing wound to the left side of his chest. On primary survey: BP 70/40 mmHg, HR 130/min, trachea deviated to the right, absent breath sounds on the left, distended neck veins. What is the FIRST intervention?
A. Obtain a chest X-ray immediately
B. Insert a large-bore intercostal drain on the left
C. Needle decompression at the 2nd intercostal space mid-clavicular line on the left
D. Start 2 litres of IV Ringer's lactate immediately
Reveal Answer
Answer: C. Needle decompression at the 2nd intercostal space mid-clavicular line on the left
This is a tension pneumothorax: haemodynamic instability + tracheal deviation AWAY from the affected side + absent breath sounds + distended neck veins. It is a clinical diagnosis requiring immediate needle decompression (2nd ICS, MCL) BEFORE any radiological investigation. A chest X-ray would cause a fatal delay. After needle decompression (which converts the tension pneumothorax to a simple pneumothorax), an intercostal drain is inserted definitively.