Page 3 of 26
OR1.1 | Pre-hospital Trauma Care and Emergency Room Triage — SDL Guide (Part 3)
Orthopaedic Priorities in the Trauma Bay
Orthopaedic injuries rarely cause immediate airway or breathing compromise, but they are major contributors to haemorrhagic shock and long-term disability. Understanding the haemorrhage potential of common fractures and the orthopaedic contributions to the primary survey is essential for all doctors managing trauma. A femoral shaft fracture alone can sequester 1–2 litres of blood into the thigh compartment without any visible external bleeding, and an open-book pelvic disruption can accumulate 2–4 litres in the retroperitoneal space — both sufficient to cause Class III haemorrhagic shock. For this reason, the orthopaedic examination is an integral part of the ATLS primary survey circulation assessment, not an afterthought relegated to the secondary survey.
Blood loss estimation by fracture site provides the clinician with a mental framework for assessing the haemorrhagic risk of skeletal injury:
- Tibial shaft fracture: 0.5–1.5 litres
- Femoral shaft fracture: 1–2 litres (may be more in elderly with poor muscle tone)
- Pelvic fracture (open book): 2–4 litres or more (retroperitoneal haematoma, venous plexus)
- Humeral shaft fracture: 0.5–1 litre
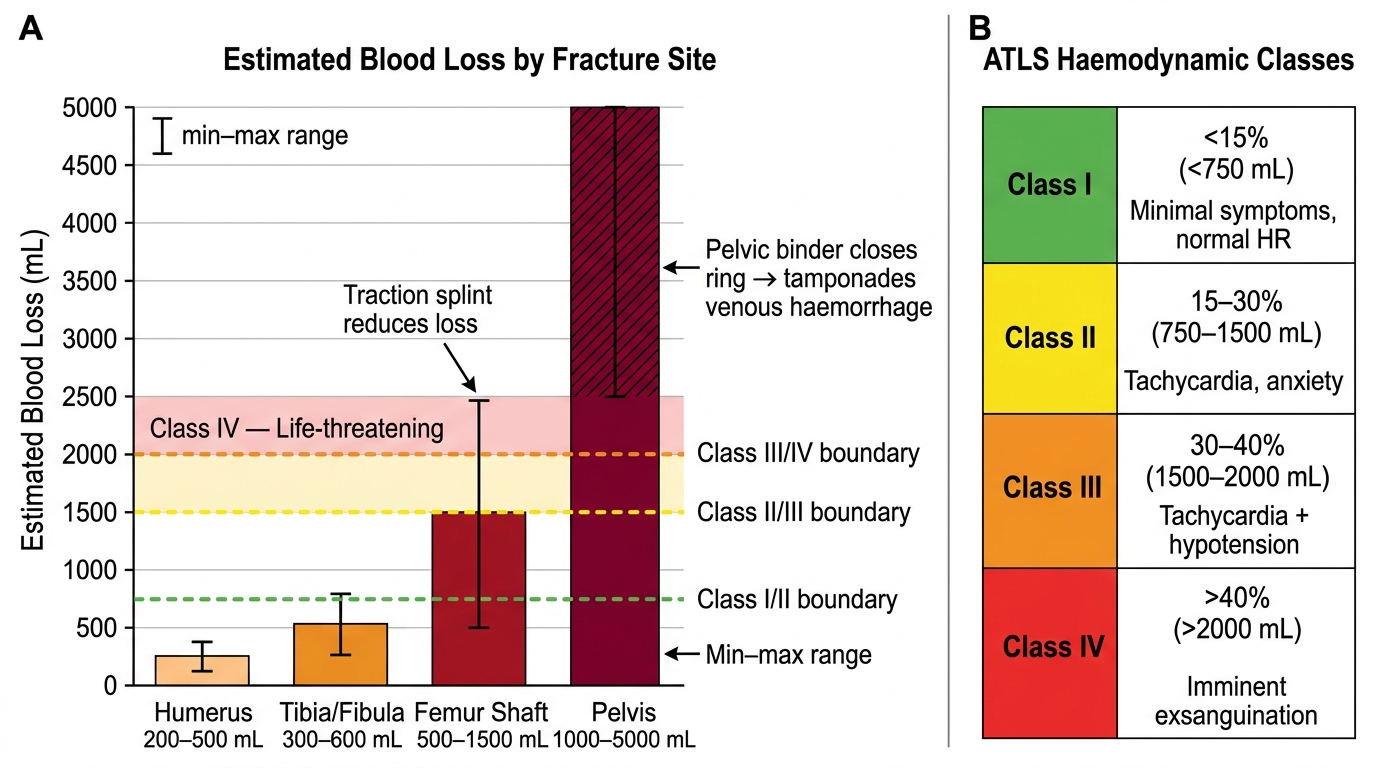
Fracture Site Blood Loss Potential and Haemodynamic Classification Thresholds
The pelvic ring deserves special attention. An open-book pelvic fracture (anteroposterior compression, pubic symphysis diastasis >2.5 cm, sacroiliac joint disruption) dramatically increases pelvic volume, allowing massive haemorrhage into the retroperitoneal space. The immediate intervention is a pelvic binder applied at the level of the greater trochanters (NOT at the level of the iliac crests, which can worsen displacement). A sheet, commercial binder, or improvised wrap all achieve the same haemostatic effect by closing the pelvic ring and tamponading venous haemorrhage.
Open fractures require immediate orthopaedic attention in the emergency room. The Gustilo-Anderson classification (Type I: wound <1 cm, clean; Type II: wound 1–10 cm, moderate contamination; Type IIIA: wound >10 cm, adequate soft tissue coverage; Type IIIB: wound >10 cm, periosteal stripping, requires soft-tissue reconstruction; Type IIIC: arterial injury requiring repair) guides management. All open fractures require:
1. Photography of the wound (document once, then cover with saline-soaked gauze)
2. Wound cover — do NOT repeatedly remove the dressing to examine the wound (increases infection risk)
3. Intravenous antibiotics within 1 hour of injury (co-amoxiclav or cephalosporin; add gentamicin for Grade III; add metronidazole for farm/soil contamination)
4. Tetanus prophylaxis
5. Urgent surgical debridement — the '6-hour rule' (debridement within 6 hours) is now superseded by 'as soon as feasible after stabilisation,' with antibiotics serving as the time-critical intervention
Neurovascular assessment of every injured limb is mandatory before any splinting or manipulation. Document distal pulses, sensation (light touch in the territory of the nerve most at risk), and active motor function. This is especially important for supracondylar fractures of the humerus (risk to brachial artery and median nerve/AIN), knee dislocation (popliteal artery, common peroneal nerve), and hip dislocation (sciatic nerve).
Self-Assessment: Applying ATLS Principles
The following structured self-assessment scenarios allow you to consolidate the ATLS framework, triage principles, and damage control concepts covered in this module. Work through each scenario mentally before reviewing the rationale. The goal is not recall of isolated facts but application of systematic thinking under simulated time pressure — the cognitive skill that ATLS training is designed to build.
Scenario 1: A 35-year-old pedestrian was struck by a truck at 60 km/h. He arrives with a GCS of 12 (E3V4M5), BP 88/60 mmHg, HR 124/min, respiratory rate 26/min. The right thigh is grossly swollen and deformed. There is no obvious external bleeding. What are your first three actions in sequence, and what is the physiological explanation for his haemodynamic state?
Scenario 2: At a road traffic collision with six injured patients, you are the first doctor on scene with only two nurses. Using START triage criteria, describe how you would classify: (a) an 18-year-old walking and crying, (b) a 45-year-old with RR 28/min and a radial pulse but who is confused, (c) a 60-year-old who is apnoeic and remains apnoeic after one jaw thrust, (d) a 30-year-old with RR 14/min, strong radial pulse, and follows commands despite a deformed leg.
Scenario 3: A patient with a closed femur fracture and BP 90/60 mmHg after 1 L of Ringer's lactate — the BP has not improved. What is your next step and why? What are the two main reasons crystalloid alone is insufficient in this setting?
Reflect on the answers after your self-assessment. For any question where you were uncertain, return to the relevant content block and re-read the mechanism before proceeding to the next SDL in this cluster.
CLINICAL PEARL
The 'load and go' rule in trauma: When a trauma patient shows signs of haemorrhagic shock (systolic BP <90 mmHg, HR >120/min, altered consciousness) despite initial IV access, the most life-saving action is to move the patient to theatre or a trauma centre — NOT to spend more time on procedures in the emergency room. A patient with uncontrolled intra-abdominal haemorrhage cannot be resuscitated; they can only be saved by surgically stopping the bleeding. Every minute of delay in reaching operative haemorrhage control costs lives. An ATLS teaching phrase captures this: 'Don't just do something, stand there... and then move the patient to theatre.'
Additionally, remember: in trauma, absent or diminished pulse in a limb is a late sign of vascular injury. Do not be falsely reassured by a palpable pulse. Pain out of proportion to the apparent injury, pallor, paraesthesia, and perishingly cold skin are earlier and more sensitive warning signs. The clinical context — a displaced supracondylar fracture or a knee dislocation — should keep your index of suspicion for vascular injury high regardless of pulse status.