Page 1 of 11
OR10.1 | Bone Tumour and Pathological Fracture Assessment — SDL Guide
Learning Objectives
- Distinguish benign from malignant bone tumours on clinical and radiological grounds
- Describe the characteristic radiological features of osteosarcoma, Ewing's sarcoma, giant cell tumour, and skeletal metastases
- Apply Enneking staging to a described bone tumour scenario
- State the principles of biopsy planning along the future resection line
- Outline the management of pathological fractures through primary bone tumours
INSTRUCTIONS
Bone tumours are uncommon but carry serious consequences when missed or mismanaged at the primary-care level. An inappropriate biopsy outside the planned resection corridor can contaminate tissue planes and render a limb-salvage procedure impossible. As a final-year student about to enter clinical practice, you must be able to recognise the red-flag presentation of a bone swelling, interpret the key radiological patterns, stage the lesion appropriately, and refer it urgently while avoiding the twin traps of premature biopsy and pathological fracture mismanagement.
References
- Maheshwari's Essential Orthopaedics, 6th ed, Chapter 26: Tumours of Bone (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, 10th ed, Chapter 11: Bone Tumours (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 16-year-old boy presents with a three-week history of progressively worsening pain around the lower end of his right femur. His parents thought it was a sports injury and delayed seeking help. On X-ray, you notice a triangular elevation of periosteum at the metaphysis and a sunburst pattern of bone spicules. Beneath your hands, the swelling is warm, tender, and slightly pulsatile. This is not a sprain. The next steps you take — including whether and how you biopsy this lesion — will determine whether this young man keeps his leg.
WHY THIS MATTERS
Bone tumours account for roughly 6% of all childhood cancers, and osteosarcoma alone has a peak incidence in the second decade of life — the very patients who will pass through your outpatient clinic. The consequences of a missed diagnosis (delayed curative surgery) or a poorly planned biopsy (limb-salvage failure, amputation) are irreversible. Pathological fractures through malignant bone add haematogenous dissemination risk. Understanding the diagnostic and staging framework is therefore not an academic exercise but a patient-safety imperative. You will also encounter skeletal metastases frequently in ward patients with known breast, prostate, lung, thyroid, or renal-cell carcinoma — the commonest sources of secondary bone disease.
RECALL
Before proceeding, review what you know: (1) The periosteum is a fibrous layer covering bone that elevates when a rapidly expanding tumour pushes it outward; (2) the metaphysis is the flared region between the epiphysis and the diaphysis — the zone of most active bone growth; (3) normal bone remodelling involves osteoblasts (formation) and osteoclasts (resorption); (4) staging in oncology generally combines tumour size/extent (T), nodal involvement (N), and distant spread (M). Keep these concepts active as you work through the tumour categories below.
Clinical Presentation: Recognising the Red-Flag Bone Swelling
A patient with a bone tumour most often presents with pain — initially intermittent, then constant, worse at night, and unrelieved by rest. This pattern of rest pain and nocturnal pain is a critical red flag that distinguishes tumour-related bone pain from musculoskeletal pain of mechanical origin, which typically improves with rest. The second cardinal feature is swelling: a firm or bony-hard, non-tender (or mildly tender) mass in the region of a long bone. Rapid growth, warmth, and surface-vein dilatation indicate an aggressive lesion.
The third feature — and perhaps the most diagnostically important for the student — is the age of presentation. Osteosarcoma characteristically affects adolescents in the second decade (peak 10–20 years), particularly around the knee (distal femur, proximal tibia) and proximal humerus. Ewing's sarcoma has a similar adolescent peak but involves the diaphysis of long bones and flat bones. Giant cell tumour (GCT) presents in skeletally mature adults (20–40 years) at the epiphysis. Metastatic bone disease dominates in patients over 40 with a known primary tumour.
A pathological fracture — fracture through diseased bone — may be the presenting event. Unlike a traumatic fracture, the history is one of a fracture that occurs with trivial or no trauma, often preceded by weeks of pain. You should also elicit constitutional symptoms: fever and weight loss raise the probability of malignancy or infection.
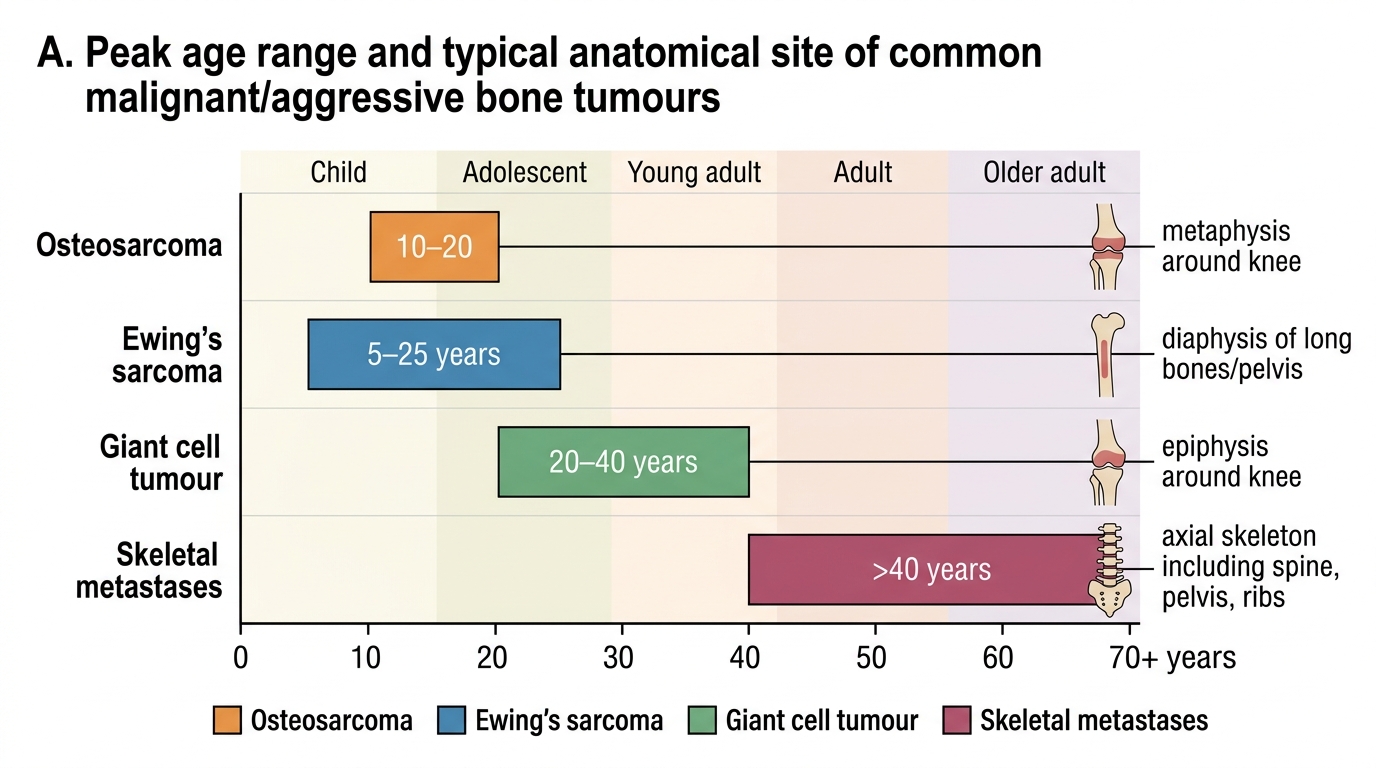
Age Distribution and Typical Sites of Bone Tumours
Pathology and Radiological Patterns: Benign versus Malignant
The radiological distinction between benign and malignant bone tumours rests on a cluster of features that reflect the biological behaviour of the lesion — specifically how rapidly it is growing relative to the bone's ability to contain and react to it. Understanding these features mechanistically makes them far easier to remember and apply than rote memorisation.
Benign tumours grow slowly. The bone has time to lay down a zone of reactive sclerosis around the lesion, producing a well-defined sclerotic margin (Lodwick grade IA/IB). The cortex is intact or thinned but not destroyed. Periosteal reaction, if present, is complete and solid rather than interrupted. Soft-tissue extension is absent.
Malignant tumours (primary or metastatic) grow rapidly. The bone cannot keep pace and the margin becomes ill-defined (Lodwick grade II/III, permeative or moth-eaten). Cortical destruction occurs. The periosteum is elevated at the junction of normal bone and tumour, leaving a triangular shadow — the Codman's triangle — which represents reactive bone at the lifted periosteal edge. As tumour spicules grow outward perpendicular to the shaft in a radial pattern, the appearance is the sunburst (or sunray) pattern. These two signs together are the radiological hallmark of osteosarcoma (also called osteogenic sarcoma).
In Ewing's sarcoma, the radiological pattern differs because the tumour arises from the diaphysis and infiltrates along the medullary canal first. This creates the classic onion-skin appearance — multiple thin, concentric layers of periosteal new bone reflecting the rhythmic attempts of the periosteum to contain the tumour between surges of growth. The diaphyseal location and the age group (5–25 years) are the two most important differentiating clues from osteosarcoma.
Giant cell tumour (GCT) arises at the epiphysis of long bones after physeal closure (hence adulthood presentation). It occupies the end of the bone, typically the distal femur, proximal tibia, or distal radius. The X-ray shows an eccentric, lytic lesion without a sclerotic margin, with a soap-bubble trabecular pattern created by thin bone septa within the tumour. It may expand the cortex but rarely breaks it.
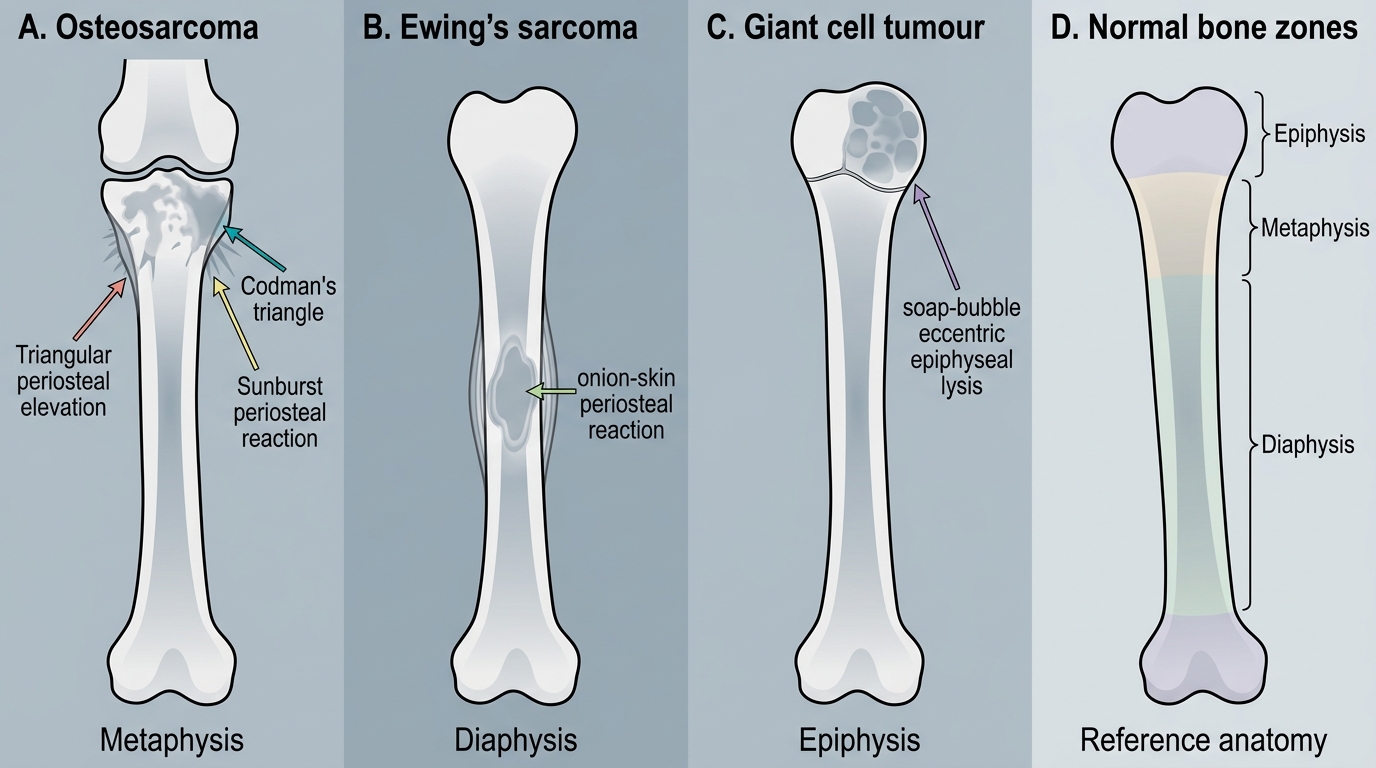
Classic X-ray Patterns of Bone Tumours
Specific Tumour Entities: Features and Location Summary
A systematic review of the most frequently tested primary and secondary bone tumours consolidates the pattern-recognition framework built in the previous section. For each tumour, focus on the triad: patient age — bone zone affected — radiological hallmark.
Osteosarcoma (osteogenic sarcoma) is the commonest primary malignant bone tumour. It occurs in the metaphysis of long bones, predominantly the distal femur (around 40% of cases), proximal tibia, and proximal humerus. Peak age: 10–20 years (a second smaller peak occurs in elderly patients with Paget's disease). The tumour produces osteoid directly from the malignant cells — this distinguishes it histologically. Radiologically: Codman's triangle, sunburst pattern, mixed lytic-and-sclerotic appearance.
Ewing's sarcoma is the second commonest primary bone malignancy in young patients. Location: diaphysis of long bones (femur, tibia, humerus) and flat bones (ilium, ribs — important). Histology: small round blue cells arranged in sheets (Homer-Wright rosettes). Radiologically: onion-skin periosteal reaction, permeative lysis. Clinically important: Ewing's can mimic osteomyelitis (fever, raised ESR, local heat) — think of it as the great imitator in the diaphysis.
Giant cell tumour (GCT) affects epiphyses in skeletally mature adults. The distal femur and proximal tibia account for more than 50% of GCTs. Classification: Campanacci grade I (quiescent), II (active), III (aggressive with cortical breach/soft-tissue extension). GCT is locally aggressive but only 5% are frankly malignant. Treatment: extended curettage + bone cement or bone grafting for grades I/II; wide excision for grade III.
Skeletal metastases are far commoner than all primary bone tumours combined. The commonest primaries to metastasise to bone are: breast, prostate, lung, thyroid, and kidney — a useful mnemonic is the 5 Bs: Breast, Bone (myeloma counts), Bronchus, Blood (haematological), Basicially-thyroid-and-kidney (admittedly imperfect — but the first three are most common). Metastases are typically lytic (breast[some], lung, thyroid, kidney) or sclerotic/blastic (prostate, some breast). The axial skeleton (spine, pelvis, ribs, proximal femur) is preferentially affected because of its red marrow content and vertebral venous plexus (Batson's plexus).
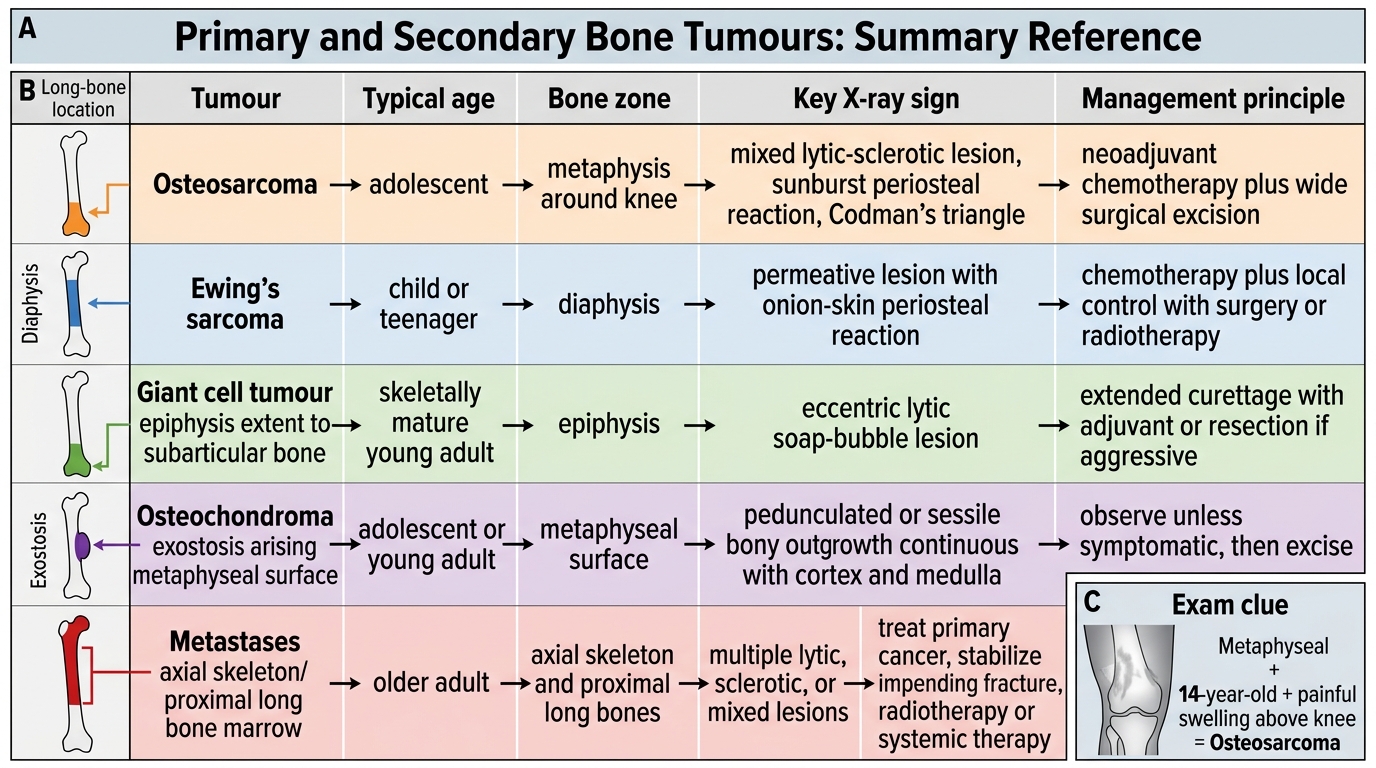
Bone Tumours: Summary Reference Table
SELF-CHECK
A 14-year-old boy presents with a painful swelling above the knee. X-ray shows a mixed lytic-sclerotic lesion at the distal femoral metaphysis with a Codman's triangle. Which tumour is most likely?
A. Ewing's sarcoma
B. Osteosarcoma
C. Giant cell tumour
D. Solitary bone metastasis
Reveal Answer
Answer: B. Osteosarcoma
The combination of adolescent age, metaphyseal location (distal femur), Codman's triangle, and mixed lytic-sclerotic pattern with sunburst formation is the classical presentation of osteosarcoma. Ewing's involves the diaphysis; GCT affects the epiphysis in adults; metastases are rare at 14 years.