Page 2 of 11
OR10.1 | Bone Tumour and Pathological Fracture Assessment — SDL Guide (Part 2)
Examination and Investigations: Staging a Bone Tumour
The clinical examination of a suspected bone tumour follows a systematic sequence. Begin with the general examination: look for weight loss, pallor (anaemia of malignancy), lymphadenopathy, and any soft-tissue mass that may indicate the primary tumour for metastases. Move to local examination: site, size, surface, edge (well-defined or irregular), consistency (hard, bony, firm), temperature (warmth suggests vascularity), transillumination (a cyst would transilluminate), and surface veins. Test regional lymph nodes. Assess neurovascular status of the limb distally.
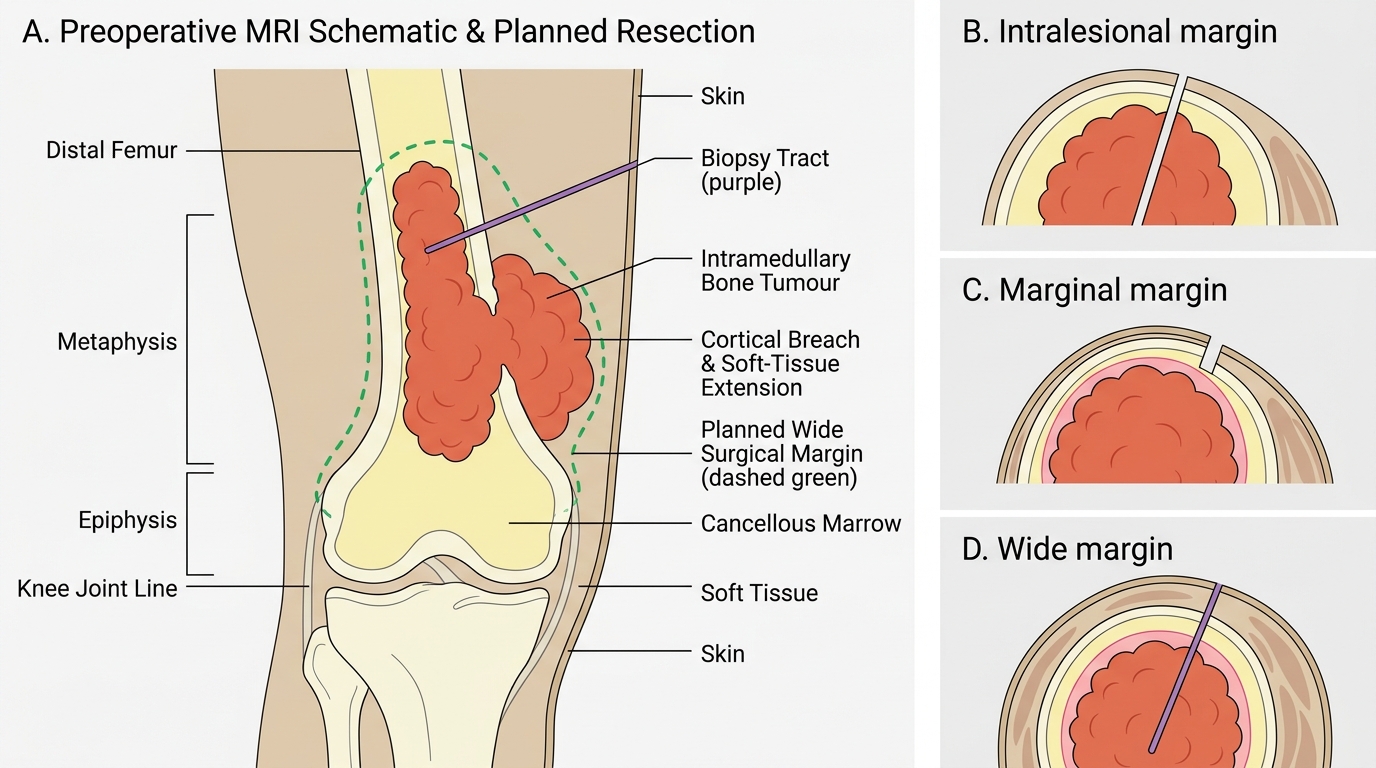
The radiological sequence for staging begins with plain X-rays of the affected bone in two planes — these remain the single most informative initial investigation for characterising the lesion. Next, MRI with contrast delineates the intramedullary extent (critical for planning resection margins), soft-tissue involvement, and skip lesions. CT of the chest is mandatory for pulmonary metastases (the lungs are the most common site of distant spread for primary bone sarcomas). A bone scan (technetium-99m scintigraphy) identifies polyostotic involvement and distant bone metastases. PET-CT provides metabolic activity data and whole-body staging.
Laboratory investigations include serum alkaline phosphatase (markedly elevated in osteosarcoma — a useful marker of disease activity and response to chemotherapy), LDH (elevated in Ewing's — poor prognostic factor if very high), calcium and phosphate (for metabolic bone disease screen), and CBC with ESR. Biopsy is the definitive diagnostic step.
Distal Femur Bone Tumour: Extent and Surgical Margins
Enneking Staging and the Biopsy Principle
The Enneking (MSTS) staging system, developed by William Enneking and adopted by the Musculoskeletal Tumor Society, is the international standard framework for staging primary bone and soft-tissue sarcomas, and it directly determines the required surgical margins and the indication for adjuvant therapies such as chemotherapy and radiotherapy. Unlike the TNM system used for carcinomas, which places major emphasis on regional lymph-node involvement, the Enneking system recognises that primary bone sarcomas spread haematogenously rather than via lymphatics, and that the most important local determinant of surgical outcome is whether the tumour has breached its natural anatomical barriers. The system is therefore built on three independent criteria that reflect biological behaviour: first, histological grade — low-grade (G1, well-differentiated, slow-growing, lower metastatic potential) versus high-grade (G2, poorly differentiated, rapidly growing, high metastatic potential); second, tumour compartment — T1 intracompartmental (confined within the bone cortex or within the muscle compartment of origin) versus T2 extracompartmental (has breached the cortex, joint capsule, or fascial barrier into adjacent tissue); and third, distant metastases — M0 absent versus M1 present. Once a tumour is classified as T2 (extracompartmental), surgical planning must include all contaminated tissue planes, substantially enlarging the required resection. This generates five Enneking stages:
| Stage | Grade | Site | Mets | Description |
|---|---|---|---|---|
| IA | G1 | T1 | M0 | Low-grade, intracompartmental |
| IB | G1 | T2 | M0 | Low-grade, extracompartmental |
| IIA | G2 | T1 | M0 | High-grade, intracompartmental |
| IIB | G2 | T2 | M0 | High-grade, extracompartmental |
| III | G1 or G2 | T1 or T2 | M1 | Any grade, metastatic |
Osteosarcoma and Ewing's sarcoma are typically Stage IIB or III at presentation. The stage determines the surgical margin required: low-grade (Stage I) may allow a marginal or wide excision; high-grade (Stage IIA/IIB) requires a wide margin (en-bloc resection with a cuff of normal tissue on all sides); Stage III requires multimodal oncology involvement.
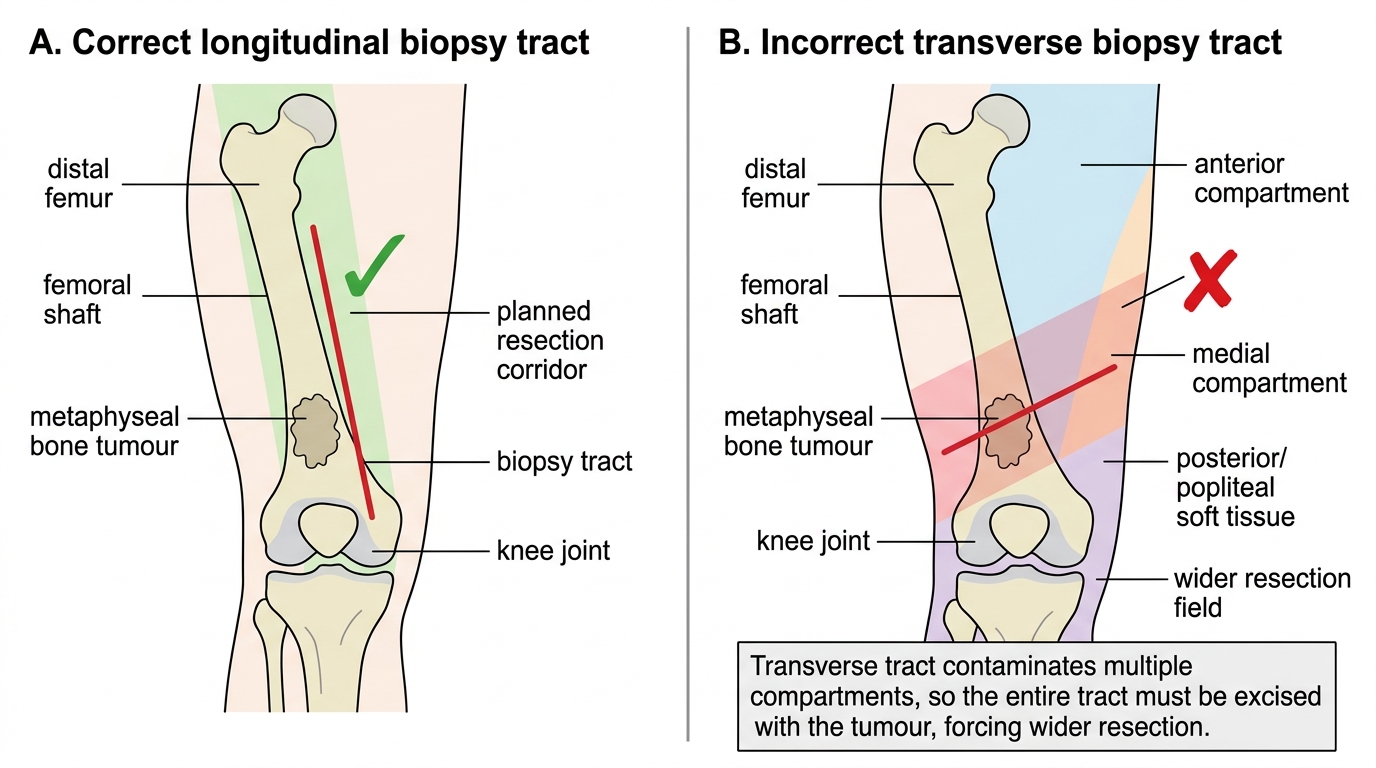
The biopsy principle is arguably the most clinically critical concept in bone-tumour surgery: the biopsy must be planned along the axis of the future definitive surgical resection. The reason is that any tissue contaminated by the biopsy tract must be excised en bloc with the tumour at definitive surgery — a biopsy outside the planned resection corridor contaminates new tissue planes and either forces amputation or leaves positive margins. In practice, this means the biopsy is always placed in line with the planned incision. An incisional biopsy (through a small longitudinal incision) is preferred over a large transverse incision that crosses multiple compartments. Needle core biopsy guided by imaging is preferred for accessible lesions because it minimises contamination while yielding adequate tissue.
Biopsy Tract Placement in Distal Femoral Bone Tumour
SELF-CHECK
A biopsy of a distal femoral mass returns high-grade osteosarcoma. Imaging shows the tumour has breached the posterior cortex into the popliteal soft tissue but there are no lung metastases. What is the Enneking stage?
A. Stage IA
B. Stage IIA
C. Stage IIB
D. Stage III
Reveal Answer
Answer: C. Stage IIB
High-grade (G2) tumour with extracompartmental extension (T2 — has breached the cortex into surrounding tissue) without distant metastases (M0) = Stage IIB by the Enneking system. Stage IIA would be high-grade but confined within the compartment (T1).
Management of Bone Tumours and Pathological Fractures
Management of bone tumours is multidisciplinary and stage-determined. The principles below are organised from benign to malignant primary tumours and then to pathological fractures.
Benign tumours such as osteochondroma (the commonest bone tumour overall — a cartilage-capped bony exostosis from the metaphysis, usually asymptomatic) are managed conservatively if asymptomatic; surgical excision is indicated for cosmetic concerns, mechanical symptoms, or suspected malignant transformation (growth after skeletal maturity, thick cartilage cap >2 cm on MRI). Simple bone cyst (unicameral bone cyst, a fluid-filled intraosseous cavity in the proximal humerus or femur of children) is treated by aspiration-injection (steroid or bone-marrow aspirate) or curettage and grafting if repeated fractures occur.
Osteosarcoma: the current standard of care is neoadjuvant chemotherapy (pre-operative, typically cisplatin + doxorubicin + methotrexate for 8–12 weeks) followed by limb-salvage surgery with wide margins, followed by adjuvant chemotherapy. The purpose of neoadjuvant chemotherapy is threefold: reducing tumour bulk, treating micrometastases, and assessing histological response (>90% necrosis = good response, better prognosis). Amputation is reserved for cases where wide margins cannot be achieved or where the neurovascular bundle is involved. Five-year survival for localised disease is approximately 60–70%.
Ewing's sarcoma: highly chemosensitive. Management: multi-agent chemotherapy (vincristine, actinomycin-D, cyclophosphamide, ifosfamide, etoposide — VAC/IE alternating) followed by local control — either wide surgical excision or radiotherapy (Ewing's is radiosensitive, which osteosarcoma is NOT). Five-year survival for localised disease: 60–70%; for metastatic disease, <30%.
Giant cell tumour: primarily surgical. Extended curettage with high-speed burr + adjuvant (liquid nitrogen cryotherapy, phenol, or hydrogen peroxide) + cavity filling with polymethylmethacrylate (bone cement) or bone graft. Bone cement allows early detection of local recurrence on X-ray. Recurrence rate ~20%. Denosumab (anti-RANKL monoclonal antibody) is used as adjuvant for unresectable or recurrent GCT.
Skeletal metastases: the goal shifts from cure to pain control and fracture prevention. Management includes the EBRT (external beam radiotherapy) for pain relief (70-80% response), bisphosphonates (zoledronic acid) or denosumab for bone protection, orthopaedic fixation for actual or impending pathological fractures, and systemic therapy targeting the primary tumour.
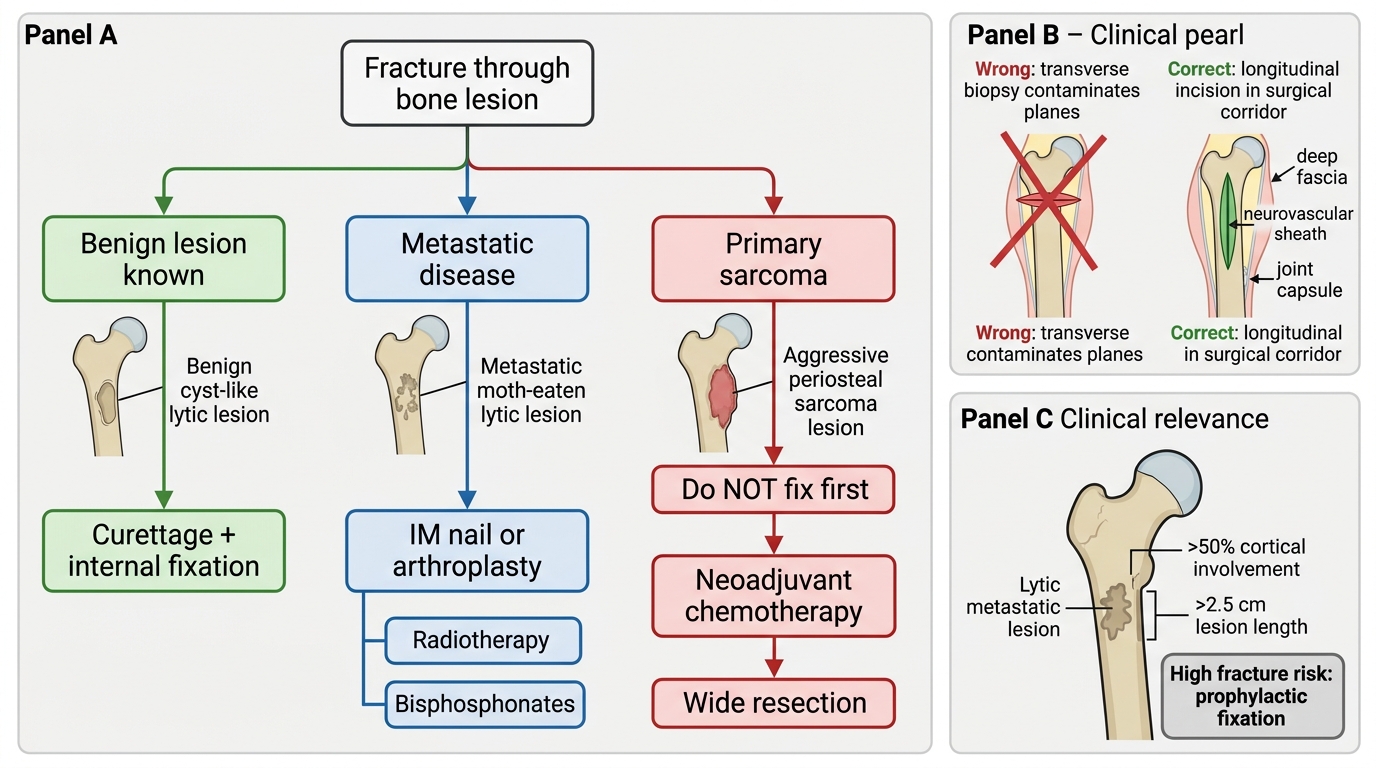
Pathological fracture management follows a distinct algorithm from traumatic fractures because the fracture is through diseased bone with inherent impaired healing. Key principles: (1) exclude a benign lesion (simple bone cyst, fibrous dysplasia) that can be treated with curettage + fixation; (2) for metastatic fractures, intramedullary nailing (IM nail) is the preferred fixation because it stabilises the entire bone, controls the fracture, and allows early weight-bearing and mobilisation — this is critical in palliative patients; (3) for pathological fractures in primary malignant tumours, the fracture does NOT change the Enneking stage but may complicate margins — neoadjuvant chemotherapy is still given first in osteosarcoma; (4) pathological fractures through metastatic lesions in the femoral head/neck may require hemiarthroplasty or total hip replacement rather than fixation; (5) impending pathological fracture (Mirels score ≥9) should be prophylactically fixed before the fracture occurs.
Management of Pathological Fracture Through a Bone Lesion
CLINICAL PEARL
Never biopsy a bone tumour through a transverse incision. A transverse biopsy wound crosses multiple tissue planes and cannot be cleanly excised en bloc — contaminating the deep fascia, neurovascular sheath, or joint capsule forces either amputation or positive margins. Always use a small longitudinal incision in line with the definitive surgical corridor, and discuss biopsy site with the orthopaedic oncology team BEFORE making the cut. An inappropriate biopsy is the single most preventable cause of unnecessary amputation in bone-tumour surgery.
For skeletal metastases: a lytic lesion in the proximal femur with >50% cortical involvement and >2.5 cm length = high risk of pathological fracture (Mirels score). Fix it prophylactically — waiting for the fracture doubles operative risk and significantly worsens functional outcomes in a patient with limited prognosis.
Self-Assessment: Consolidating Bone Tumour Knowledge
Work through the following scenarios to consolidate your understanding of bone tumour recognition, staging, and management principles. For each scenario, form your differential, identify the most likely diagnosis, determine the Enneking stage where applicable, and outline the first steps in management.
Scenario A: A 55-year-old woman with known breast cancer presents with severe pain in the right hip. X-ray shows a 3 cm lytic lesion in the femoral neck with 60% cortical destruction. She walks with a limp. What is the Mirels score likely to suggest, and what is the management?
Scenario B: A 22-year-old man has a painless swelling at the distal femur for four years. It has grown slowly. X-ray shows a pedunculated bony exostosis pointing away from the joint with a cartilage cap. No pain, no night symptoms. Most likely diagnosis and management?
Scenario C: A 17-year-old presents with fever, raised ESR (82 mm/h), and a warm, tender swelling over the mid-femoral diaphysis. X-ray shows a permeative lytic lesion with faint onion-skin periosteal layering. Blood cultures are negative. What two diagnoses should be foremost in your mind, and what investigation will differentiate them?
Expected reasoning: A = metastatic bone disease, prophylactic fixation (IM nail or hemiarthroplasty), bisphosphonates, radiotherapy; B = osteochondroma, conservative management (wide excision if symptomatic); C = Ewing's sarcoma vs osteomyelitis — both present identically clinically; differentiated by bone biopsy (core needle biopsy, preferably at a specialist centre).