Page 1 of 11
OR12.1 | Congenital Malformation and Deformity Assessment — SDL Guide
Learning Objectives
- Describe the clinical features, examination findings, and diagnostic criteria for scoliosis, including Cobb angle measurement and differentiation of idiopathic from congenital forms
- Outline the clinical presentation, examination manoeuvres (Ortolani, Barlow, Galeazzi), imaging selection, and management of developmental dysplasia of the hip (DDH)
- Describe the aetiopathogenesis, clinical features, and management of congenital muscular torticollis
- Explain the CAVE components of congenital talipes equinovarus (CTEV), apply the Pirani score, and describe the Ponseti method of conservative correction
- Identify key red-flag features requiring urgent referral and select appropriate imaging modalities by age and diagnosis
INSTRUCTIONS
Congenital musculoskeletal disorders are among the most common structural abnormalities encountered in newborn examinations and paediatric outpatient clinics. Early detection transforms outcomes: developmental dysplasia of the hip detected in the neonatal period is correctable with a simple harness, while the same condition missed until walking age requires complex surgery. As a final-year student rotating through orthopaedics, you will be expected to perform or assist with newborn hip screening examinations, recognise positional foot and spine deformities, and counsel families on prognosis and referral pathways. This module addresses four core conditions — scoliosis, spinal dysraphism, DDH, congenital muscular torticollis, and clubfoot — equipping you with a systematic approach to examination, appropriate investigation selection, and evidence-based first-line management.
References
- Maheshwari's Essential Orthopaedics, Chapter on Congenital Disorders (textbook)
- Apley and Solomon's System of Orthopaedics and Trauma, Congenital and Developmental Disorders (textbook)
- Ebnezar's Textbook of Orthopaedics, Congenital Anomalies and Deformities (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A mother brings her three-day-old baby to the newborn clinic. During routine examination you attempt to abduct the infant's hips and feel a distinct 'clunk' on the left side. The mother has no idea what this might mean. She wants to know: is this serious? Will my child walk normally? Does she need surgery? Your ability to answer these questions — and to initiate the correct pathway today — will determine whether this child has normal hip development or faces reconstructive surgery at age two.
WHY THIS MATTERS
Congenital musculoskeletal disorders collectively affect approximately 1–2% of all live births. They are among the conditions most subject to missed diagnosis at the primary care and general practice level, yet they are also the conditions most responsive to early intervention. The window for conservative, non-surgical treatment is narrow and age-dependent: it closes decisively for DDH by six months of age, for clubfoot deformity by about one year, and for neuromuscular scoliosis by skeletal maturity. As a doctor in any setting — emergency department, rural health centre, or urban clinic — you will encounter these children, and the quality of your initial assessment directly determines whether they access timely specialist care.
RECALL
Before proceeding, take a moment to recall your earlier learning on musculoskeletal anatomy and development:
- The embryological origin of the musculoskeletal system: mesenchymal condensation, chondrification, and ossification
- Normal range of hip abduction in a neonate (approximately 70–80°) and how restriction differs from normal
- The concept of the acetabular index and how it changes with age in normal hip development
- Basic anatomy of the foot — the talus, calcaneus, cuboid, navicular — and the normal axis relationships
- What 'equinus', 'varus', and 'adduction' mean as positional descriptors in foot deformity
- Basic vertebral anatomy and the concept of the three-column spine
Scoliosis: Definition, Classification, and Clinical Presentation
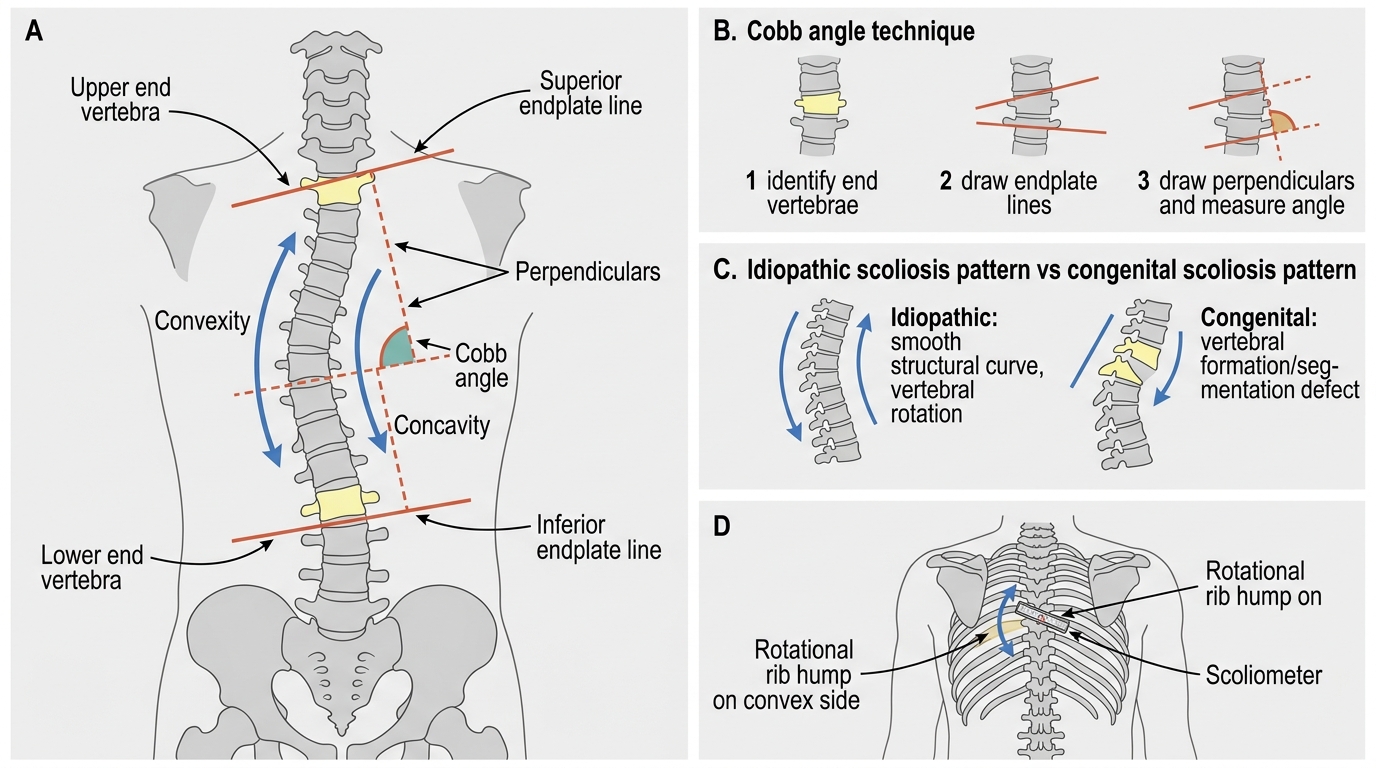
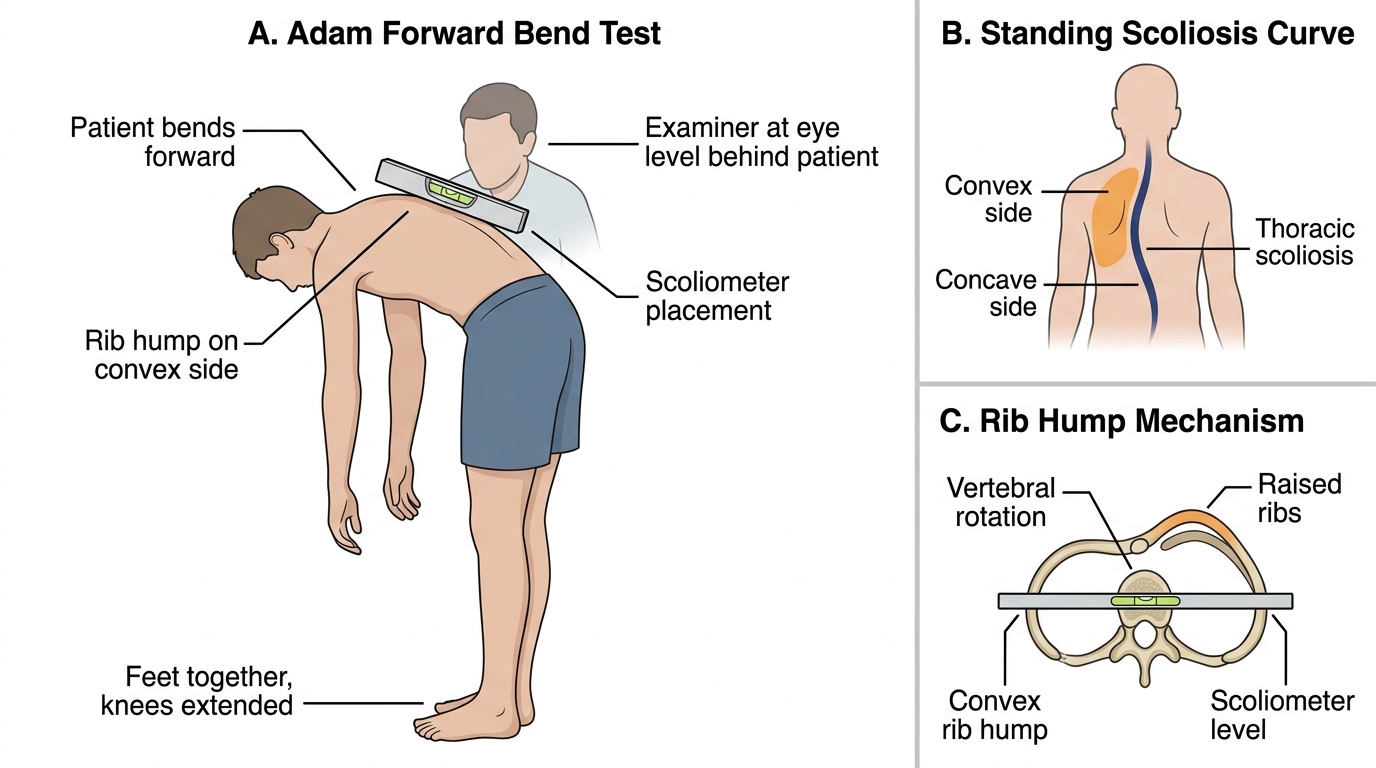
Scoliosis is defined as a lateral curvature of the spine measuring ≥10° by the Cobb angle method on a standing anteroposterior radiograph, almost invariably accompanied by vertebral rotation. This rotation is the pathological hallmark of structural scoliosis: the vertebral bodies rotate toward the convexity of the curve, causing rib hump formation on the convex side when the patient bends forward (the Adam's forward bend test). Understanding this rotational component is critical because it distinguishes true structural scoliosis from the non-structural (postural) curvatures that disappear on forward bending or when the child lies down.
The vast majority of scoliosis cases in clinical practice are idiopathic, meaning no underlying structural vertebral anomaly or neuromuscular disease is identified. Idiopathic scoliosis is further classified by age of onset: infantile (birth to 3 years), juvenile (3–10 years), and adolescent (>10 years). Adolescent idiopathic scoliosis (AIS) is by far the most prevalent, affecting 2–3% of adolescents and demonstrating a striking female preponderance of approximately 7:1 for curves requiring treatment. The aetiology remains incompletely understood but likely involves genetic susceptibility, abnormal axial loading, and asymmetric vertebral growth plate activity.
Congenital scoliosis arises from embryological failures of vertebral formation (hemivertebra — a unilateral failure of segmentation or formation creating a wedge-shaped bone that drives lateral deviation) or segmentation (unsegmented bars — bony bridges fusing adjacent vertebrae unilaterally, producing tethering that promotes asymmetric growth). A unilateral unsegmented bar with a contralateral hemivertebra represents the most aggressive pattern of progression and requires early surgical referral. Congenital scoliosis demands investigation for associated anomalies, particularly genitourinary malformations (30% of cases), congenital heart disease, and intraspinal anomalies such as diastematomyelia or a tethered cord — making MRI of the whole spine mandatory.
Clinically, the patient presents with visible trunk asymmetry: uneven shoulder heights, prominent scapula on one side, unequal waist creases, or a tilted pelvis. Pain is not a typical feature of adolescent idiopathic scoliosis; its presence should prompt investigation for an underlying cause such as osteoid osteoma or a herniated disc. Leg-length discrepancy may produce a compensatory pelvic tilt and apparent lumbar curve, which corrects when the patient sits; this is a non-structural compensatory curve, not true scoliosis.
Cobb Angle Measurement and Scoliosis Curve Patterns
Adam Forward Bend Test and Rib Hump Assessment
Cobb Angle Measurement and Curve Grading
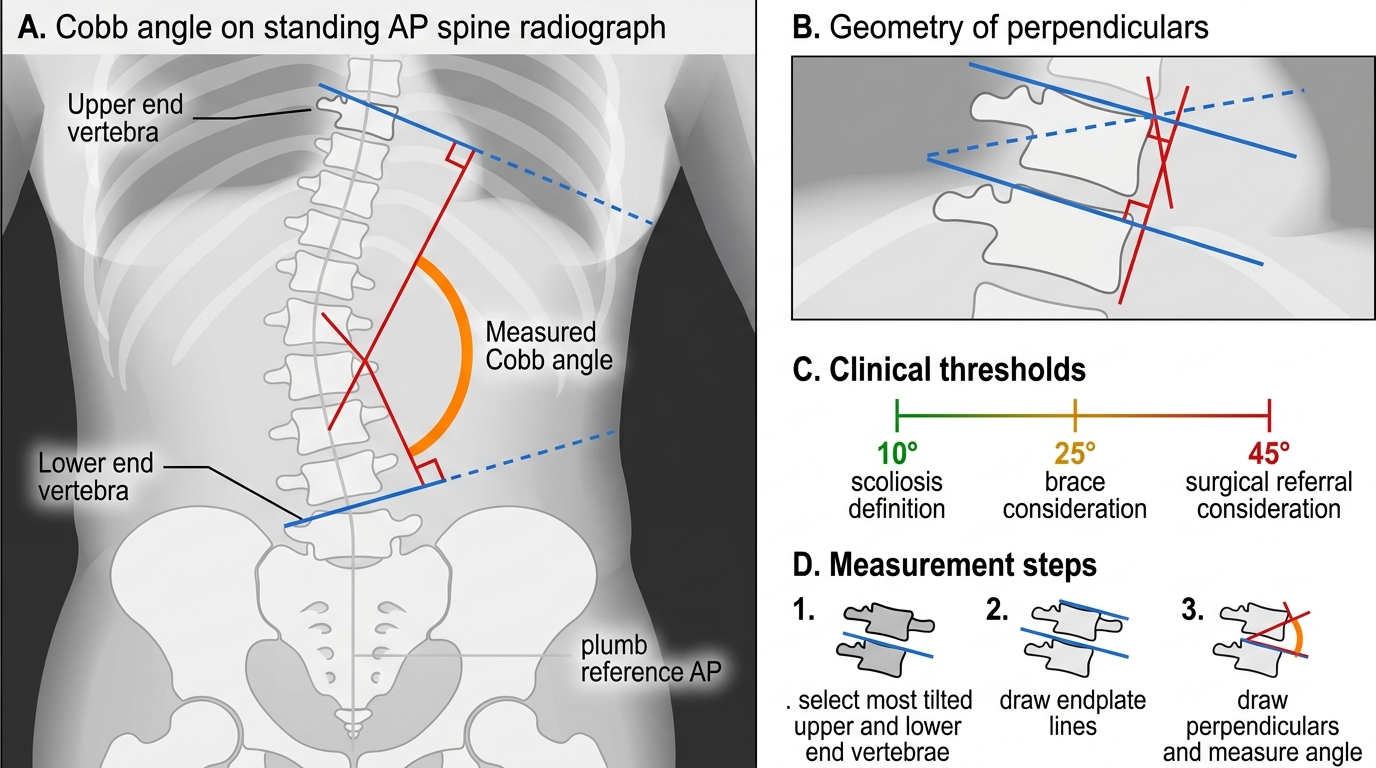
The Cobb angle is the internationally accepted metric for measuring scoliotic curve magnitude, and its accurate determination is fundamental to treatment decisions. On a standing AP radiograph of the full spine, the examiner identifies the most tilted vertebra at the upper end of the curve (the upper end vertebra) and the most tilted vertebra at the lower end (the lower end vertebra). A line is drawn along the superior endplate of the upper end vertebra and along the inferior endplate of the lower end vertebra. Perpendiculars are erected from each of these lines, and the angle between the perpendiculars (or equivalently, between the endplate lines themselves if extended) is the Cobb angle.
Curve magnitude drives management thresholds in clinical practice. For adolescent idiopathic scoliosis, the widely applied guidelines are as follows: curves less than 25° are observed with clinical review every four to six months; curves between 25° and 45° in a skeletally immature patient are managed with bracing (the thoracolumbosacral orthosis, or TLSO, worn 16–23 hours per day) to prevent progression; curves exceeding 45–50° are generally referred for surgical correction because bracing at this magnitude is ineffective and continued progression after skeletal maturity is likely. Surgery aims to achieve correction and spinal fusion, typically via posterior instrumented fusion using pedicle screws and rods.
Skeletal maturity is assessed using the Risser sign — the degree of ossification of the iliac crest apophysis, graded 0 to 5, where Risser 5 indicates complete fusion and minimal residual growth potential. Risser 0 in a pre-pubescent child with a 30° curve represents a high-risk situation for progression, warranting aggressive bracing and close surveillance.
Cobb Angle Measurement in Scoliosis
Spina Bifida: Types and Clinical Significance
Spina bifida is a neural tube defect arising from failure of the posterior neural tube to close during embryogenesis, typically in the fourth week of gestation. It represents the convergence of genetic predisposition and environmental factors — the most critical modifiable risk factor being folate deficiency during early pregnancy, which is why folic acid supplementation (400 µg daily) is recommended to all women planning pregnancy. The term encompasses a spectrum of severity, and understanding this spectrum is essential for counselling families.
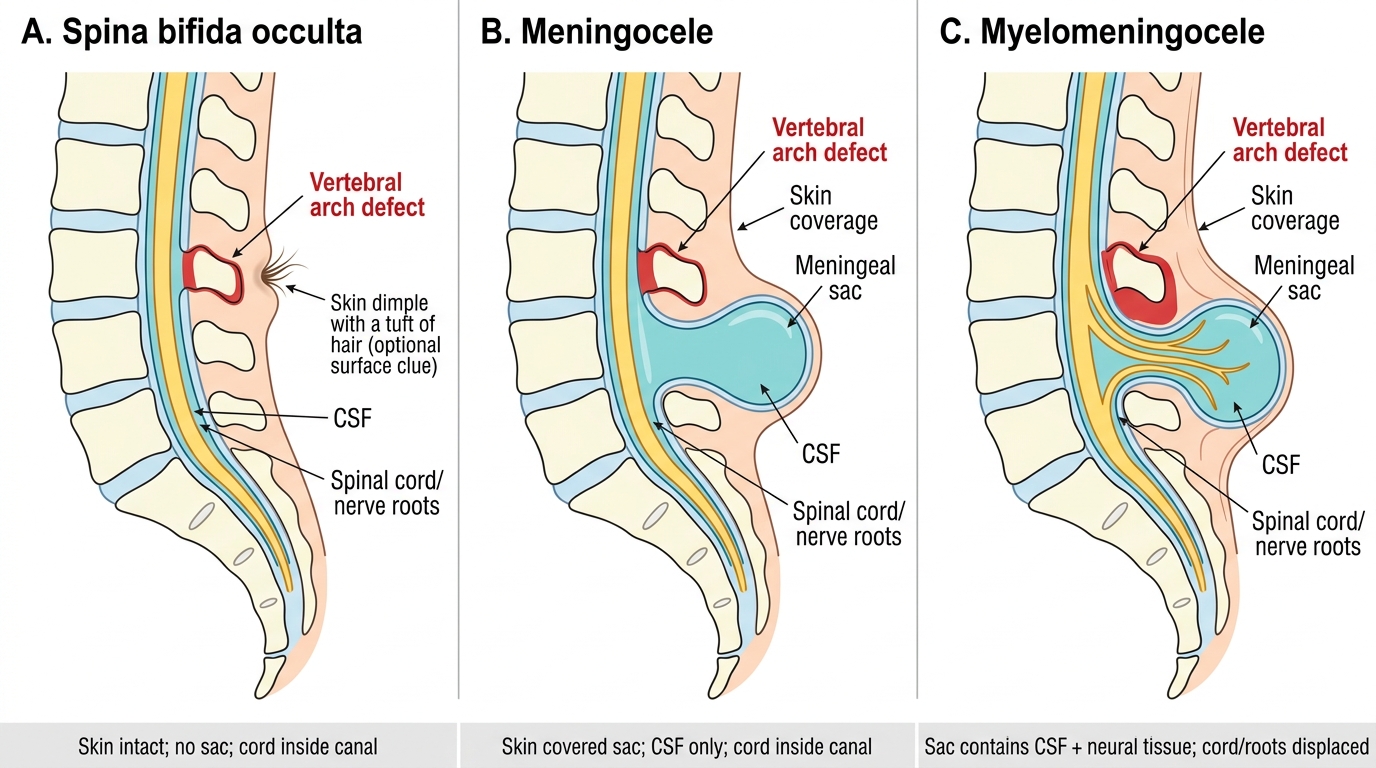
Spina bifida occulta is the mildest form: the posterior vertebral arch fails to fuse but there is no herniation of the meninges or neural tissue, and the defect is covered by intact skin. It is present in approximately 5–10% of the general population and is usually asymptomatic, discovered incidentally on radiographs or during investigation of back pain. Cutaneous stigmata — a midline tuft of hair, a dermal sinus, a capillary haemangioma, or a skin dimple above the sacral crease — may overlie the defect and should prompt further evaluation with MRI to exclude a tethered spinal cord, which can cause progressive neurological deficits as the child grows.
Spina bifida cystica encompasses two clinically important subtypes. Meningocele involves herniation of the meninges alone through the bony defect, forming a cystic sac filled with cerebrospinal fluid (CSF); the neural tissue remains within the spinal canal, so neurological function is usually intact. Myelomeningocele (or meningomyelocele) is the most severe and most clinically significant form: the meninges, CSF, and neural tissue (spinal cord or nerve roots) all herniate through the defect. This produces predictable neurological impairment below the level of the lesion — motor paralysis, sensory loss, bladder and bowel dysfunction — and is commonly associated with the Arnold–Chiari II malformation (downward displacement of the cerebellar tonsils and brainstem through the foramen magnum) and hydrocephalus (present in 70–90% of cases, requiring ventriculoperitoneal shunting).
Management of myelomeningocele begins at birth: the sac must be protected from rupture (risk of meningitis), and neurosurgical closure is performed within 24–48 hours. Prenatal diagnosis via alpha-fetoprotein measurement and anomaly ultrasound enables planned delivery at a tertiary centre. Fetal surgery for in-utero closure (before 26 weeks) has shown benefit in selected cases by reducing the need for VP shunting and improving motor outcomes.
Spina Bifida: Occulta, Meningocele, and Myelomeningocele