Page 2 of 11
OR12.1 | Congenital Malformation and Deformity Assessment — SDL Guide (Part 2)
Developmental Dysplasia of the Hip (DDH): Pathology and Risk Factors
Developmental dysplasia of the hip (DDH) — formerly called congenital dislocation of the hip (CDH) — encompasses a spectrum of abnormal hip development ranging from subtle acetabular dysplasia through subluxation (partial loss of contact between femoral head and acetabulum) to complete dislocation (the femoral head lies entirely outside the acetabulum). The term 'developmental' is preferred because the abnormality may not be present at birth in all cases: some hips are only subluxable (reducible in the examination room, unstable under physiological loading) at birth and progress to frank dislocation during the early postnatal weeks if undetected.
The pathological basis lies in the relationship between the femoral head and the acetabulum during the critical period of hip development. The acetabulum is largely fibrocartilaginous and plastically remodelled by the mechanical stimulus of the femoral head pressing into it; if the head is subluxed or dislocated, the acetabulum fails to deepen properly, remaining shallow (acetabular dysplasia). The fibrocartilaginous labrum is everted, the joint capsule becomes elongated and lax, and the psoas tendon may interpose across the acetabulum, creating a barrier to reduction (the hourglass constriction).
Risk factors for DDH follow a recognisable clinical pattern. The most important are: female sex (6:1 female predominance — oestrogen-induced ligamentous laxity affects females more, as does the response to maternal progesterone and relaxin); positive family history (10-fold increased risk in a first-degree relative); breech presentation (20-fold increased risk — the flexed, adducted position of a frank breech limits hip abduction and impairs acetabular moulding); firstborn status (primigravid uterus is less accommodating); oligohydramnios (reduced amniotic fluid limits fetal movement and promotes intrauterine postural deformity); and associated congenital conditions such as torticollis, metatarsus adductus, and calcaneovalgus foot. The left hip is affected more frequently than the right (60% vs 20%; both hips affected in 20%), reflecting the typical intrauterine position of the left hip against the maternal sacrum.
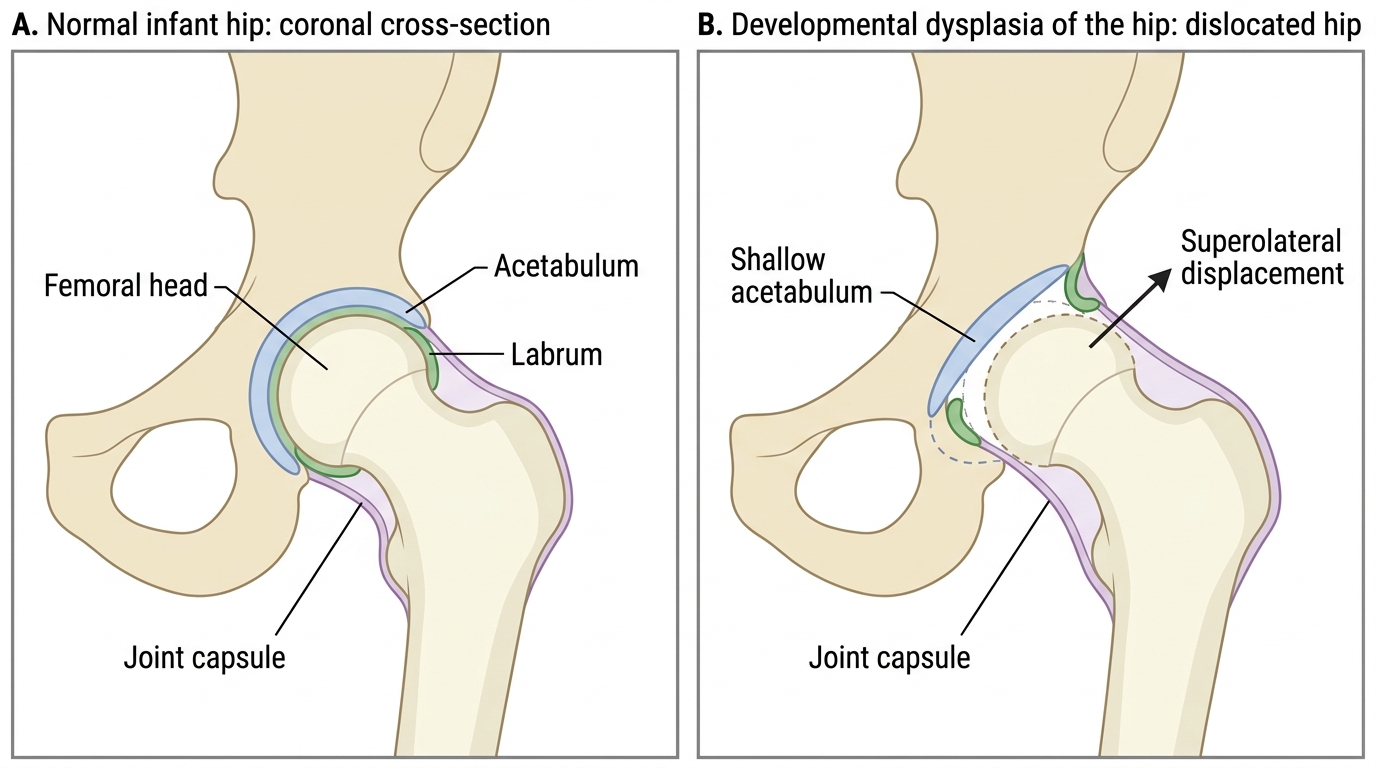
Normal Infant Hip Versus Dislocated Hip in DDH
DDH: Examination Manoeuvres and Clinical Signs
The neonatal hip examination is a clinical skill every doctor should be able to perform reliably in the first 24–48 hours of life. The examination is conducted with the infant warm, relaxed, and supine on a firm flat surface; a crying, tense infant will generate false-positive results. The examiner must distinguish between the Ortolani test (a reduction manoeuvre — detecting a dislocated hip that can be reduced) and the Barlow test (a provocation manoeuvre — detecting a reducible hip that can be dislocated).
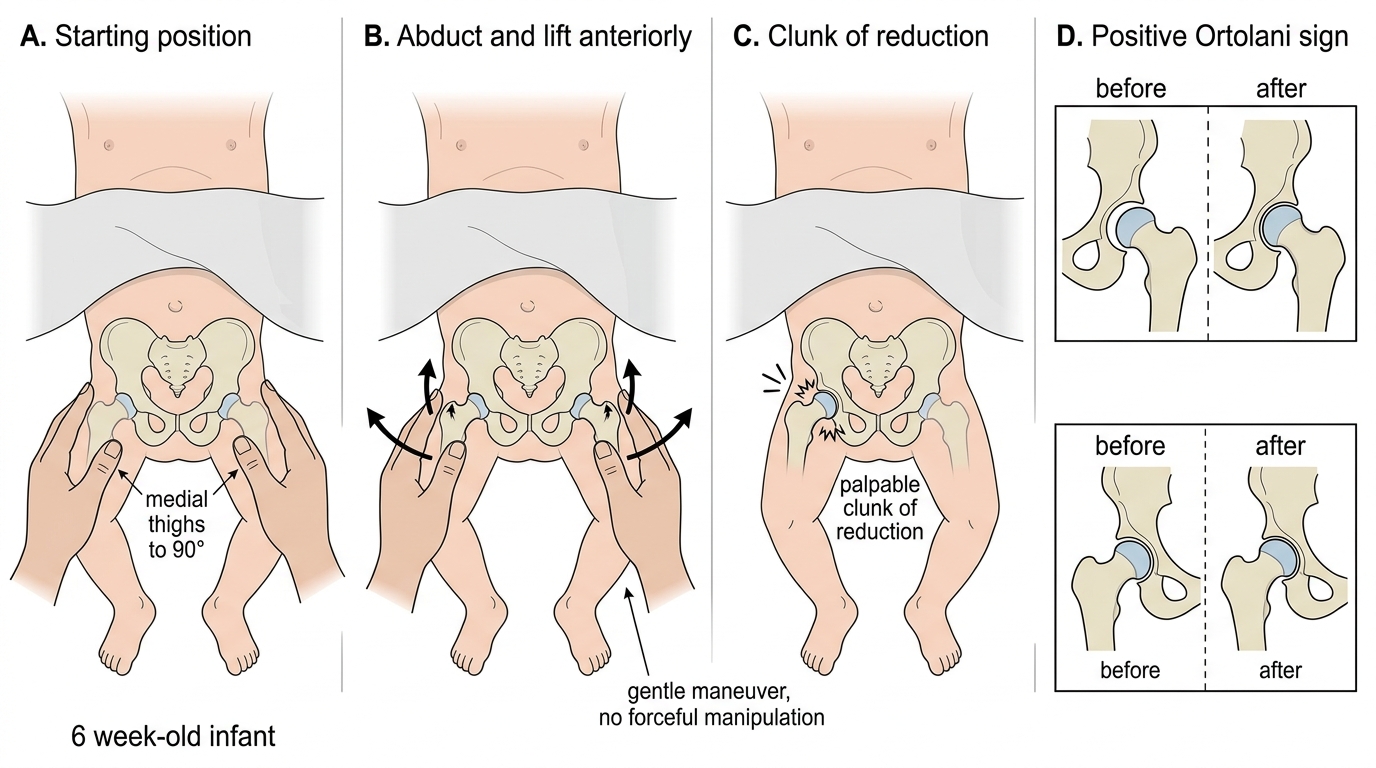
Ortolani's test is performed by placing the thumb over the lesser trochanter and the middle finger over the greater trochanter, with the hip flexed to 90°. The examiner gently abducts the hip while applying anterior pressure with the middle finger (lifting the greater trochanter anteriorly toward the socket). A positive Ortolani sign — felt, not heard — is a palpable 'clunk' of reduction as the dislocated femoral head slips back into the acetabulum. This is Ortolani positive: the hip was dislocated and is now being reduced. The classic teaching mnemonic is 'O for Out to In' (the head moves back IN to the socket on abduction).
Barlow's test is the converse: with the hip flexed at 90°, the examiner applies posterior pressure with the thumb, attempting to push the femoral head posteriorly out of the acetabulum while adducting the hip. A positive Barlow sign is a palpable (not audible) 'clunk' of dislocation as the head exits the socket. The mnemonic is 'B for Back' (the head goes back OUT of the socket on adduction and posterior pressure). In an established dislocation, Barlow may be negative (the head is already out and cannot be further displaced), while Ortolani will be positive.
Galeazzi's sign (also called Allis' sign) is used in infants aged 3–6 months and older, when Ortolani and Barlow signs typically become negative as the hip becomes progressively 'fixed' in the dislocated position. With the infant supine, both hips and knees flexed to 90° and feet flat, the examiner observes the knee heights from the side. Apparent shortening of one femur — manifesting as a lower knee on the affected side — constitutes a positive Galeazzi sign and indicates a dislocated hip on that side.
In older children who have begun to walk, the untreated dislocated hip produces a characteristic Trendelenburg gait (lurching toward the affected side during the stance phase of gait, reflecting ineffective gluteus medius function because the greater trochanter migrates superiorly and reduces the muscle's lever arm). Bilateral DDH produces the classic 'waddling gait'. Restricted hip abduction in flexion — normally approximately 70–80° in a neonate — is the single most consistent finding across all age groups.
Ortolani Test: Positive Reduction Sign
SELF-CHECK
A 6-week-old infant is brought for routine review. On examination you flex both hips to 90° and note that the right knee appears lower than the left when viewed from the side. Which clinical sign does this represent, and what does it indicate?
A. Positive Ortolani sign — the hip can be reduced by abduction
B. Positive Barlow sign — the hip can be provoked to dislocate
C. Positive Galeazzi sign — apparent femoral shortening due to ipsilateral hip dislocation
D. Negative Trendelenburg sign — normal gluteus medius function
Reveal Answer
Answer: C. Positive Galeazzi sign — apparent femoral shortening due to ipsilateral hip dislocation
The Galeazzi (Allis) sign is elicited by flexing both hips and knees to 90° with feet flat and comparing knee heights. Apparent shortening of one femur (lower knee on the affected side) indicates femoral shortening from a dislocated hip on that side. By 6 weeks the Ortolani and Barlow signs are becoming less reliable as the hip stiffens in the dislocated position; Galeazzi remains positive. A Trendelenburg sign requires the child to stand on one leg and is not applicable at 6 weeks.
DDH: Imaging and Age-Based Investigation
Imaging selection in DDH is critically age-dependent, determined by the state of ossification of the femoral head and acetabulum. Understanding this is a frequent examination question and a practical clinical necessity.
Before 4–6 months of age, the femoral head is entirely cartilaginous and cannot be visualised on plain radiographs. Ultrasound is therefore the investigation of choice in this age group. The Graf classification of neonatal hip ultrasound (the most widely used system) measures two angles: the alpha angle (bony roof angle, reflecting the depth of the bony acetabulum — normal ≥60°) and the beta angle (cartilaginous roof angle). A Graf Type I hip (alpha ≥60°) is normal; Type IIa (50–59°, infant <3 months) may be physiologically immature; Type IIb and beyond indicate progressive dysplasia requiring treatment. Dynamic ultrasound also allows real-time assessment of hip stability during Barlow provocation, providing information unavailable on a static radiograph.
After 4–6 months of age (and certainly after 6 months), the femoral head ossification centre begins to appear, making plain radiography (anteroposterior pelvis) the primary imaging modality. Standard radiographic lines are drawn to quantify dysplasia: Hilgenreiner's line (horizontal through both triradiate cartilages), Perkin's line (vertical through the lateral acetabular margin), and the acetabular index (angle between Hilgenreiner's line and a line from the triradiate cartilage to the bony acetabular rim — normal <30° at birth, <20° at 2 years). In a normal hip the femoral head ossification centre lies in the inferomedial (safe) quadrant formed by these lines; dislocation displaces it superolaterally.
MRI is used for pre-operative planning in complex cases and to assess soft-tissue interposition (hypertrophied ligamentum teres, inverted labrum, or psoas tendon creating the hourglass constriction) that would prevent closed reduction.
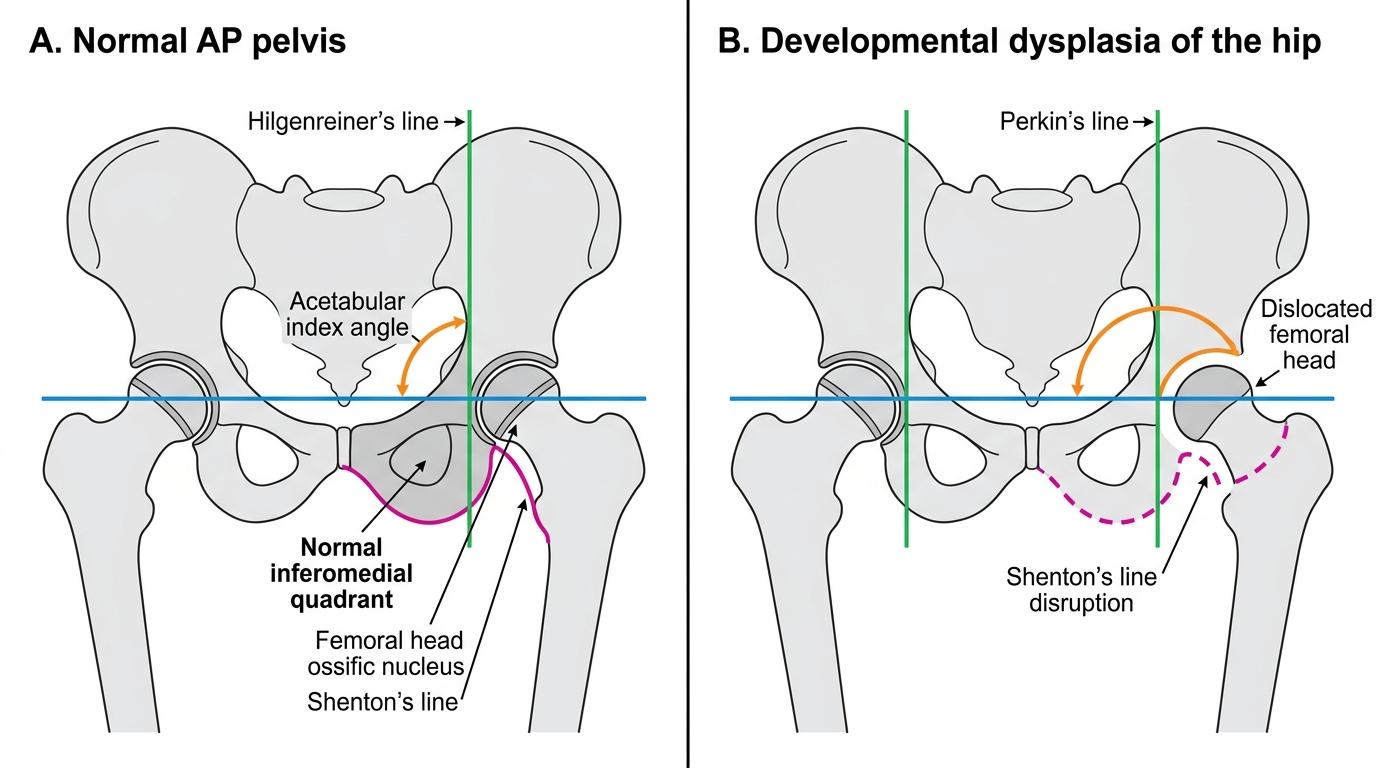
AP Pelvis Landmarks in DDH