Page 1 of 13
OR2.7 | Pelvi-acetabular Injury with Hemodynamic Instability — SDL Guide
Learning Objectives
- Describe the aetiopathogenesis and mechanism of injury of pelvic and acetabular fractures, including classification systems (Tile, Young-Burgess)
- Identify clinical features and investigations for pelvic ring disruption with emphasis on haemodynamic instability
- Outline the ATLS-based emergency management sequence including pelvic binder application, resuscitation, and haemorrhage control
- Explain the role of angioembolisation, pre-peritoneal pelvic packing, and definitive fixation in management
- Distinguish acetabular fracture patterns and their specific management approaches
INSTRUCTIONS
Pelvic fractures represent some of the most life-threatening musculoskeletal injuries encountered in trauma. High-energy mechanisms disrupt the rigid pelvic ring, tearing the rich venous plexus and potentially major arterial vessels, leading to massive retroperitoneal haemorrhage. A final-year student must recognise the haemodynamically unstable pelvis instantly, initiate emergency pelvic stabilisation with a binder or sheet, call the trauma team, and understand the sequence of life-saving interventions — from ATLS resuscitation to angioembolisation — before surgical fixation can even be considered.
References
- Maheshwari's Essential Orthopaedics, Ch on Pelvis and Acetabulum (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, Pelvic Injuries chapter (textbook)
- ATLS Advanced Trauma Life Support, 10th Edition — Musculoskeletal Trauma chapter (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 28-year-old motorcyclist arrives in the emergency department after a high-speed collision with a truck. He is pale, diaphoretic, and confused. Blood pressure is 70/40 mmHg despite two large-bore IVs running wide open. The paramedics applied a makeshift compression wrap around his pelvis. X-ray shows a widely open pubic symphysis and sacroiliac joint disruption on the right. You have minutes to make decisions that will determine whether he lives or dies. What do you do next, and in what order?
WHY THIS MATTERS
Pelvic ring fractures account for fewer than 5% of all fractures but carry a mortality approaching 10–20% in high-energy injuries, rising sharply when haemodynamic instability is present. The pelvis is the second most common site of life-threatening haemorrhage after the chest in blunt trauma polytrauma patients. As a final-year house officer, you may be the first doctor to assess such a patient, and your immediate actions — recognising pelvic instability, applying or confirming a pelvic binder, initiating ATLS resuscitation, and activating the trauma cascade — are literally life-saving. Additionally, missed acetabular fractures lead to post-traumatic osteoarthritis and long-term disability. Competency OR2.7 mandates that you understand both the emergency haemorrhage-control phase and the subsequent definitive fracture management.
RECALL
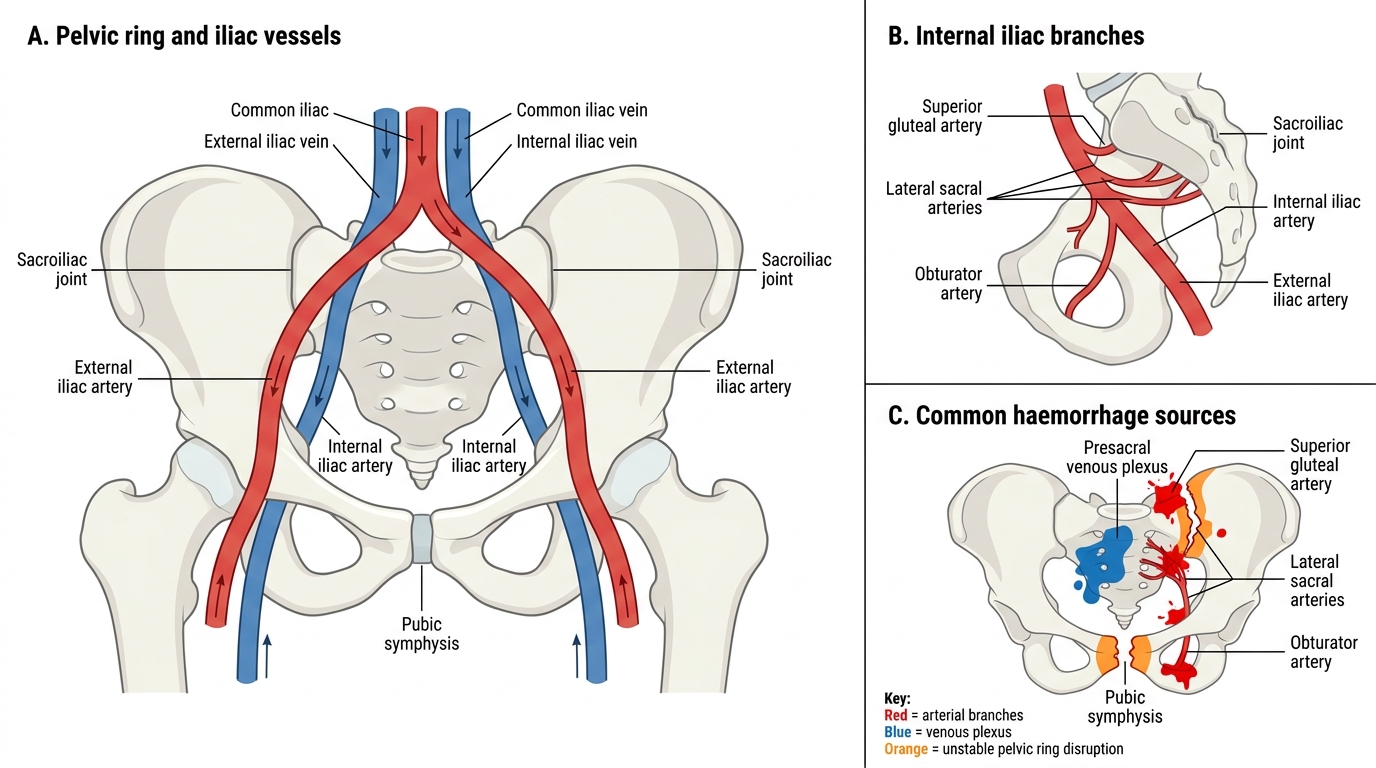
Recall your anatomy: the pelvic ring is formed by two innominate bones (each comprising ilium, ischium, and pubis) articulating anteriorly at the pubic symphysis and posteriorly with the sacrum via the sacroiliac joints. The posterior SI ligaments are the strongest ligamentous complex in the body, providing rotational and vertical stability. The internal iliac system — particularly the superior gluteal, lateral sacral, and obturator vessels — and the presacral venous plexus run in close proximity to the posterior pelvic ring. Remember your ATLS primary survey: A (Airway), B (Breathing), C (Circulation with haemorrhage control), D (Disability), E (Exposure). Pelvic haemorrhage falls under 'C'. Recall also that the retroperitoneal space can accommodate 3–4 litres of blood before tamponade occurs.
Aetiopathogenesis and Mechanism of Injury
Pelvic fractures result almost exclusively from high-energy trauma: motor vehicle collisions, pedestrians struck by vehicles, motorcycle crashes, falls from height, and industrial crush injuries. These forces exceed the remarkable tensile and compressive strength of the pelvic ring, disrupting one or more of its three articulations — the pubic symphysis, and the bilateral sacroiliac joints. The pattern of disruption depends directly on the direction, magnitude, and point of application of the force.
The pelvic ring behaves like a rigid circle: a break at one point requires either a second break or a ligamentous disruption elsewhere to permit displacement. This fundamental biomechanical principle explains why seemingly 'isolated' pubic rami fractures in young adults almost always have a posterior component on careful imaging. The posterior ring provides 60% of pelvic stability; its disruption — particularly of the posterior SI ligaments — predicts instability and haemorrhage.
Haemorrhage in pelvic fractures arises from three sources. The presacral venous plexus and the pelvic sidewall veins (low-pressure but high-volume) are responsible for approximately 85–90% of pelvic haemorrhage. Arterial injury — most commonly the superior gluteal artery, lateral sacral artery, or internal pudendal artery — accounts for 10–15% but produces faster, higher-pressure bleeding that is more amenable to angioembolisation. Finally, fracture-surface bleeding from cancellous bone contributes continuously. The retroperitoneal space acts as a tamponade until it is exhausted, at which point catastrophic haemodynamic collapse follows.
Acetabular fractures occur when a force is transmitted along the femoral axis into the acetabulum — classically in a knee-dashboard impact or a fall from height landing on the greater trochanter. The acetabulum is the articular socket formed by the confluence of all three innominate components, making acetabular fracture patterns complex and often requiring CT to delineate fully.
Pelvic Ring Anatomy and Haemorrhage Sources
Key force vectors and their fracture patterns:
| Mechanism | Direction | Typical Pattern |
|---|---|---|
| Lateral compression (LC) | Side impact | Ipsilateral pubic rami + posterior crush |
| Anteroposterior compression (APC) | Front-rear | Symphysis diastasis + SI joint opening |
| Vertical shear (VS) | Axial / fall | Hemipelvis displaces cranially — most unstable |
| Combined mechanism (CM) | Mixed | Variable, often APC + VS elements |
Classification Systems: Tile and Young-Burgess
Provided image
Two classification systems are clinically important because they guide management and communicate injury severity across the orthopaedic, emergency medicine, and general surgery teams. Correctly applying these classifications allows the treating team to predict haemorrhage risk, select the appropriate stabilisation strategy, and communicate urgency when requesting interventional radiology or surgical resources. The Tile classification stratifies injuries by the structural stability of the posterior pelvic ring, which is the primary determinant of haemorrhage potential and long-term pelvic mechanics. The Young-Burgess classification approaches the same injury population from a mechanism-of-injury perspective, grouping fractures by the direction and magnitude of the causative force, and is particularly valuable for predicting which associated injuries — bladder, urethral, neurological, abdominal — are most likely to co-exist with a given pelvic fracture pattern.
The Tile classification divides pelvic ring injuries into three main types based on the integrity of the posterior sacroiliac complex:
- Type A — Stable: the posterior ring is intact; these are typically avulsion fractures, iliac wing fractures, or isolated pubic rami fractures in the elderly. Haemorrhage is minimal.
- Type B — Partially stable: incomplete disruption of the posterior ring allowing rotational instability but maintaining vertical stability. Includes the 'open-book' injury (Type B1 — APC) where the pelvis springs open like a book, and the lateral compression injury (Type B2/B3). Haemorrhage moderate to severe.
- Type C — Unstable: complete disruption of the posterior ring producing both rotational AND vertical instability. Corresponds to vertical shear injuries. Haemorrhage severe, mortality highest.
The Young-Burgess classification uses mechanism to predict injury pattern and associated organ damage:
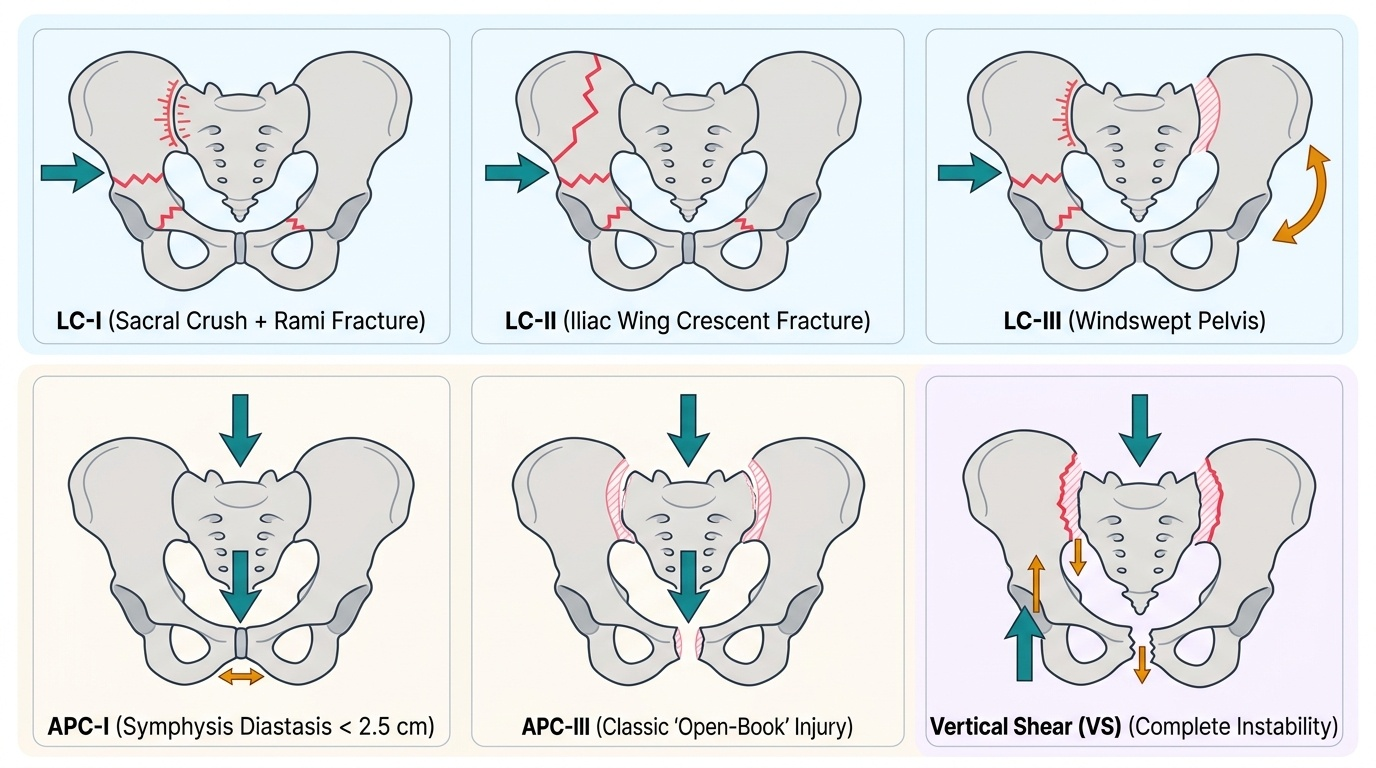
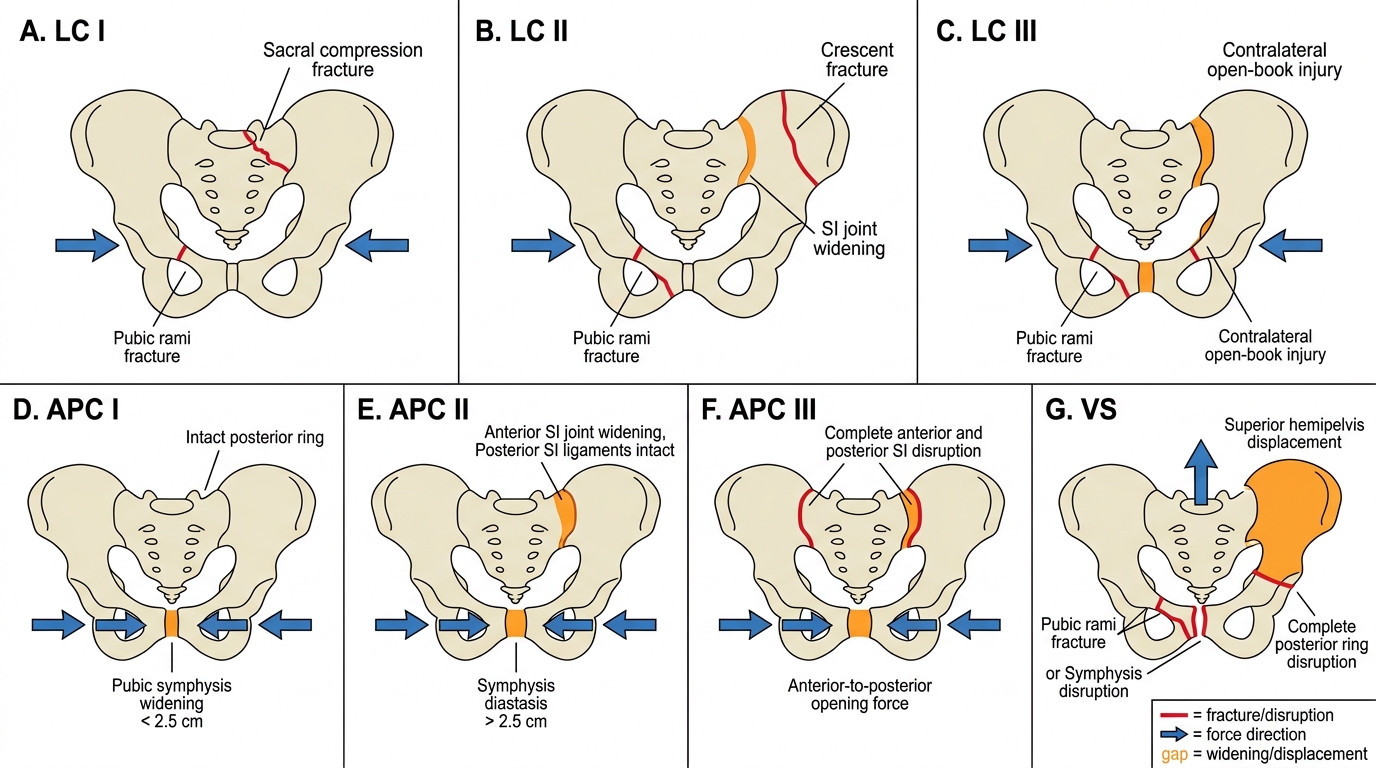
- Lateral Compression (LC) I/II/III: most common; pubic rami fracture + sacral crush (LC-I), iliac fracture (LC-II), or contralateral open-book (LC-III — windswept pelvis). Associated with bladder injury, head injury.
- Anteroposterior Compression (APC) I/II/III: symphysis diastasis progressing from minor (<2.5 cm, APC-I) to sacrotuberous/sacrospinous ligament rupture (APC-II) to complete SI joint disruption (APC-III). High-volume haemorrhage, urogenital injury, mortality highest in APC-III.
- Vertical Shear (VS): hemipelvis displaced cranially, all posterior stabilisers ruptured. Massive haemorrhage.
- Combined Mechanism (CM): elements of above.
Young-Burgess Pelvic Fracture Classification
For the acetabulum, the Judet-Letournel classification remains standard, distinguishing five elementary patterns (posterior wall, posterior column, anterior wall, anterior column, transverse) and five associated patterns (posterior wall + posterior column, transverse + posterior wall, T-type, anterior column + posterior hemitransverse, both-column). The both-column fracture — where the entire articular surface is detached from the axial skeleton — is the most complex and requires the most sophisticated reconstruction.
Clinical Features and Assessment
Clinical assessment of a pelvic injury begins within the ATLS framework during the primary survey. The haemodynamically unstable pelvis demands immediate recognition because delayed diagnosis is fatal. The physician must integrate history, vital signs, and a carefully performed physical examination while the trauma team activates simultaneously.
The hallmarks of significant pelvic fracture are pain in the pelvic girdle, groin, or lower back following high-energy trauma, combined with signs of haemorrhage. The patient may complain of inability to weight-bear, perineal pain, or difficulty voiding. In severe injuries, the patient is obtunded, pale, and in shock.
Physical examination principles for pelvic stability testing:
Manual pelvic compression and distraction ('spring test') was traditionally taught but is now DISCOURAGED as a routine bedside manoeuvre in the trauma bay because it can dislodge clot and worsen haemorrhage, and provides little additional information beyond what imaging will reveal. A single gentle lateral compression of the iliac crests by one examiner is permissible if initial imaging is unavailable; it should not be repeated. Inspect for:
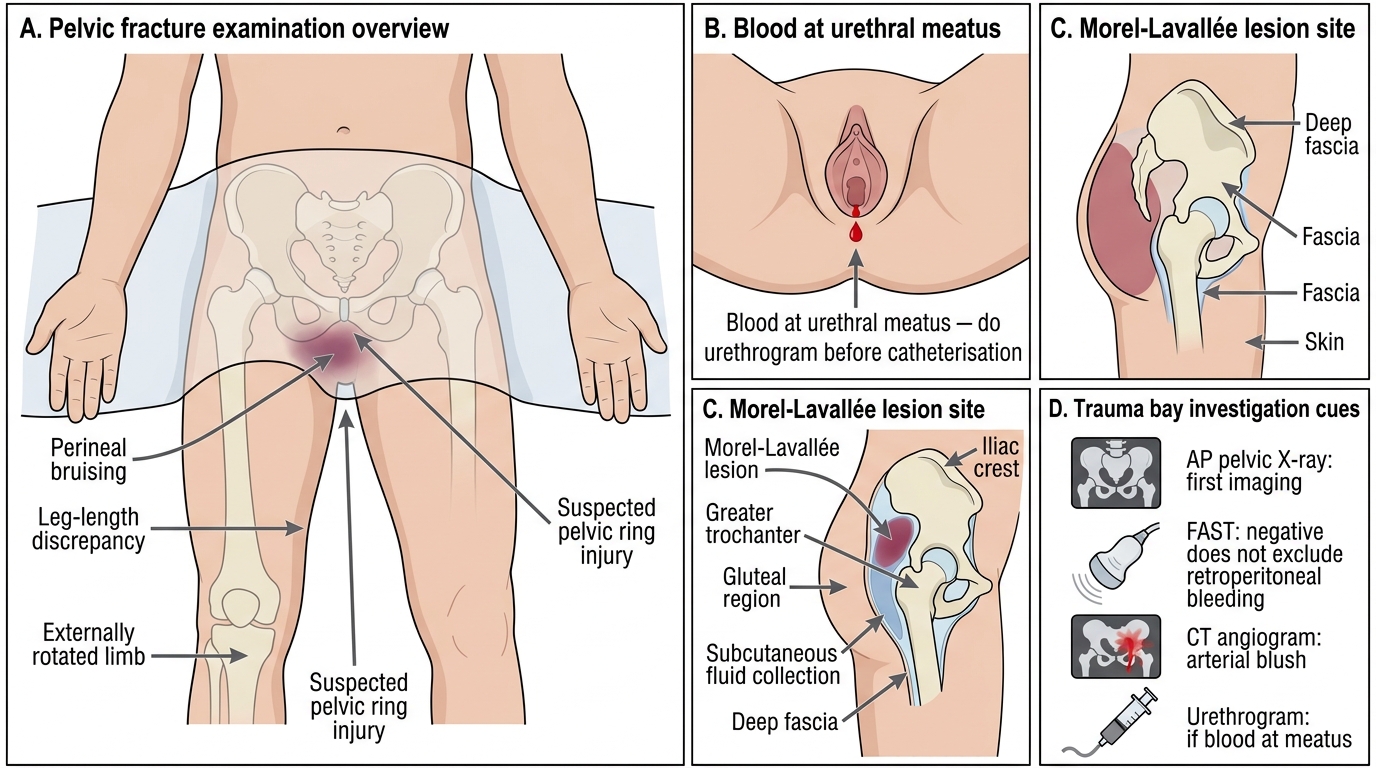
- Perineal and scrotal/labial bruising (Morel-Lavallée lesion — degloving injury of soft tissue over the greater trochanter, pelvis, or thigh)
- Leg-length discrepancy and external rotation (hemipelvis displaced cranially in VS injuries)
- Blood at the urethral meatus (urethral injury — do NOT catheterise until urology assessment)
- Rectal/vaginal laceration (open pelvic fracture — dramatically increases infection risk and mortality)
- Perineal lacerations or haematoma
- Lower limb neurology: sciatic nerve (L4-S3) exits through the greater sciatic notch and may be injured in posterior column acetabular fractures or sacral fractures; lumbosacral trunk injury causes foot drop
Haemodynamic assessment uses ATLS criteria:
- Class I: <750 mL loss, HR <100, normal BP, anxious
- Class II: 750–1500 mL, HR 100–120, normal BP, anxious
- Class III: 1500–2000 mL, HR 120–140, decreased BP, confused
- Class IV: >2000 mL, HR >140, BP <90, lethargic
A haemodynamically unstable patient is defined as systolic BP <90 mmHg not responding to 1 L crystalloid bolus and 2 units PRBC.
Clinical Examination Findings in Pelvic Fracture
Investigations in the trauma bay:
1. Pelvic X-ray AP — first imaging performed; identifies major ring disruption, symphysis diastasis (>2.5 cm = APC-II), sacral fractures
2. FAST (Focused Assessment with Sonography in Trauma) — detects intraperitoneal blood; a negative FAST does NOT exclude pelvic haemorrhage (retroperitoneal)
3. CT pelvis with IV contrast (CT angiogram) — definitive delineation of ring disruption, acetabular fractures, and active arterial extravasation ('blush' = active bleeding amenable to embolisation). Performed once patient is haemodynamically stabilised sufficiently for the scanner.
4. Urethrogram — if blood at meatus before catheterisation
5. Inlet and outlet X-ray views — supplement AP once acute phase controlled
6. Judet views (45° oblique) — for acetabular fractures to visualise anterior and posterior columns
SELF-CHECK
A 35-year-old male has pelvic fracture with BP 80/50 mmHg after 2 units PRBC. FAST is negative. What is the most appropriate immediate next step?
A. Emergency exploratory laparotomy
B. Apply a pelvic binder and activate damage-control resuscitation
C. CT angiogram of the pelvis immediately
D. Urgent open reduction internal fixation of the pelvis
Reveal Answer
Answer: B. Apply a pelvic binder and activate damage-control resuscitation
A haemodynamically unstable pelvic fracture with a NEGATIVE FAST (excluding intraperitoneal haemorrhage) should receive immediate pelvic binder application to reduce the pelvic volume and tamponade venous haemorrhage, combined with ATLS damage-control resuscitation (massive transfusion protocol). CT angiogram is performed only once the patient is sufficiently stabilised. Laparotomy is not indicated with a negative FAST. Definitive fixation is a delayed procedure after haemorrhage control.