Page 2 of 13
OR2.7 | Pelvi-acetabular Injury with Hemodynamic Instability — SDL Guide (Part 2)
Emergency Management: Haemorrhage Control and Resuscitation
The management of haemodynamically unstable pelvic fractures is a race against time and requires simultaneous actions by a coordinated trauma team. The fundamental principle is the damage-control orthopaedics (DCO) concept: achieve rapid haemorrhage control by the least invasive means, resuscitate the patient, and perform definitive repair only once physiological parameters are restored.
Step 1: Activate ATLS primary survey + massive transfusion protocol (MTP). Simultaneously establish two large-bore IVs, begin high-flow oxygen, obtain type and crossmatch, and initiate the MTP — classically packed red blood cells, fresh frozen plasma, and platelets in a 1:1:1 ratio (permissive hypotension to systolic 80–90 mmHg until bleeding controlled; avoid crystalloid dilution of coagulation factors). The 'lethal triad' of hypothermia, acidosis, and coagulopathy kills pelvic trauma patients.
Step 2: Pelvic binder application. The pelvic binder is a circumferential compression device (commercial — SAM Pelvic Sling, T-POD — or improvised with a sheet) applied at the level of the greater trochanters (NOT the iliac crests). It compresses and internally rotates the hemipelvises, reducing pelvic volume by up to 40% and tamponading venous haemorrhage. It is most effective for APC-type 'open-book' injuries and less so for LC injuries (which are already compressed). It is a bridge to definitive haemorrhage control, not a definitive treatment.
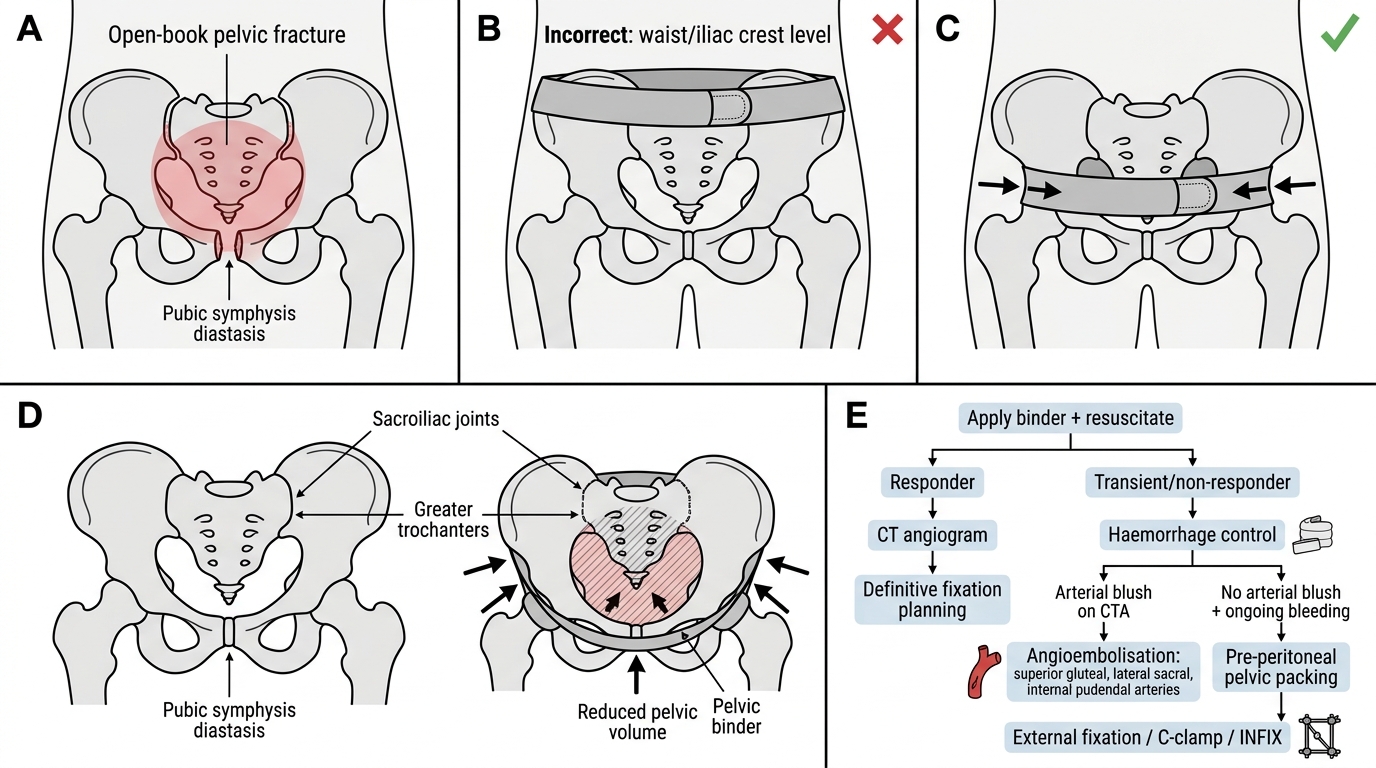
Pelvic Binder Placement and Haemorrhage Control in Open-Book Pelvic Fracture
Step 3: Determine haemorrhage control strategy. Once the binder is applied and resuscitation is ongoing, the clinical decision tree depends on the patient's response:
- Transient or non-responder → proceed to haemorrhage control:
- If CT angiogram shows arterial blush → angioembolisation by interventional radiology. Embolisation targets the bleeding vessel (commonly superior gluteal, lateral sacral, internal pudendal arteries) using coils or gelfoam. Success rate ~85–90% for arterial haemorrhage.
- If no arterial blush but ongoing haemorrhage → pre-peritoneal pelvic packing (PPP) via a small midline incision, packing the space of Retzius and bilateral paravesical spaces to compress venous plexus bleeding. This is increasingly performed as a complement or alternative to angioembolisation.
- External fixator (anterior pelvic 'C-clamp' or INFIX) provides rapid mechanical stabilisation in the resuscitation bay or operating room, reducing ring volume and providing provisional stability during damage control.
- Responder → stabilise, proceed to CT angiogram, plan definitive management.
Bladder injury (present in 10–20% of pelvic fractures): intraperitoneal rupture requires urgent surgical repair; extraperitoneal rupture is managed with catheter drainage. Urethral injury (5–10% of pelvic fractures) requires suprapubic catheter by urology — never forceful urethral catheterisation.
Step 4: Definitive fixation is performed when the patient is resuscitated (temperature >35°C, pH >7.35, coagulation normalised), typically 24–72 hours after injury. Options include:
- External fixation (provisional or definitive for anterior ring)
- Anterior plate fixation (symphyseal plating for symphysis diastasis)
- Percutaneous SI screws (standard for posterior ring fixation — minimally invasive)
- Open reduction internal fixation (ORIF) (for complex posterior ring disruptions)
Acetabular fracture management:
Acetabular fractures that are non-displaced (<2 mm) and mechanically stable can be managed conservatively with traction and touch-down weight-bearing. Displaced or unstable fractures, particularly those involving the posterior wall (risk of hip instability) or those with intra-articular fragments, require ORIF via Kocher-Langenbeck or ilioinguinal approaches. The surgical window is 5–7 days post-injury to allow haematoma organisation while avoiding fibrosis. Post-traumatic osteoarthritis remains the long-term concern, and total hip arthroplasty may be needed.
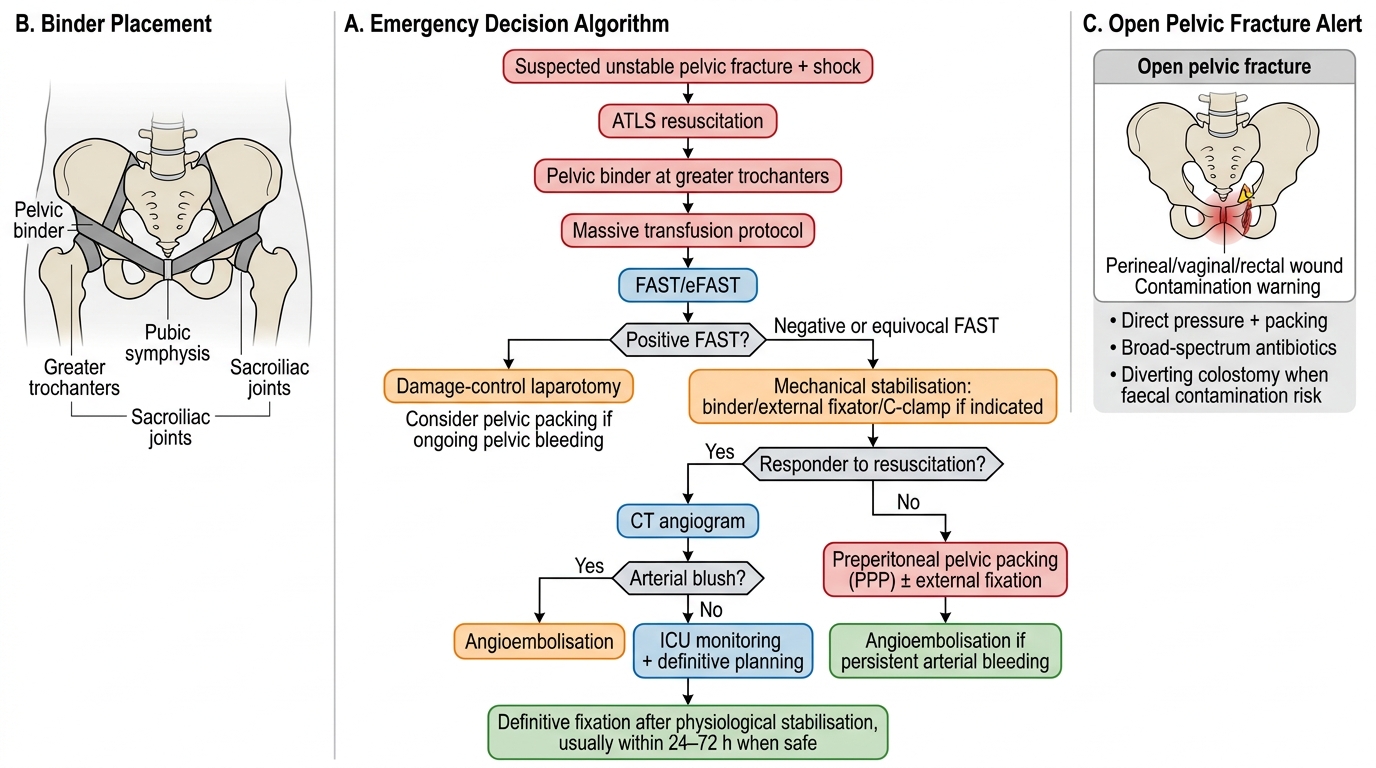
Management Algorithm for Unstable Pelvic Fracture
Open Pelvic Fractures and Special Complications
Open pelvic fractures — where a wound communicates with the fracture through the perineum, vagina, or rectum — represent a category of injury distinct in both mortality and management complexity from closed pelvic ring disruptions. Their lethality (30–50% mortality) stems from the combination of massive haemorrhage and faecal or urinary contamination of the pelvic retroperitoneum, which creates a nidus for polymicrobial infection that can progress rapidly to pelvic sepsis and multiorgan failure. The management principles therefore extend well beyond fracture haemostasis and stabilisation, requiring coordinated input from orthopaedic surgery, general surgery, gynaecology, urology, and the intensive care team. Early recognition — by identifying a perineal wound, vaginal or rectal laceration, or an open skin defect communicating with the fracture — is the house officer's most critical contribution, as the cascade of interventions depends on this diagnosis being made promptly.
Emergency steps for open pelvic fracture:
1. Control external haemorrhage with direct pressure and packing of perineal wounds
2. Diverting sigmoid colostomy to prevent faecal contamination (performed at the time of damage-control laparotomy if present)
3. Vaginal packing and gynaecological assessment for vaginal lacerations
4. Bladder and urethral assessment
5. Thorough wound debridement — emergency antibiotics within 1 hour (piperacillin-tazobactam or cephalosporin + metronidazole) + tetanus prophylaxis. The old 6-hour rule is obsolete; current evidence mandates antibiotics as early as possible, ideally within 1 hour of injury.
6. Serial washouts and delayed primary closure
Morel-Lavallée lesion is a closed degloving injury where the skin and subcutaneous tissue separate from the underlying deep fascia, creating a fluid-filled cavity filled with blood, lymph, and necrotic fat. It occurs over the greater trochanter, pelvis, and proximal thigh. If unrecognised, it becomes a nidus for infection; treatment is aspiration, sclerotherapy, or surgical debridement before fixation.
Neurological injury in pelvic fractures: the lumbosacral trunk (L4-L5) and sacral nerve roots (S1-S3) are at risk in posterior ring disruptions. Sacral fractures, particularly Denis zone III (transforaminal, through the sacral foramina) may injure bowel, bladder, and sexual function permanently. Assessment of perianal sensation, anal tone, and bladder function is mandatory.
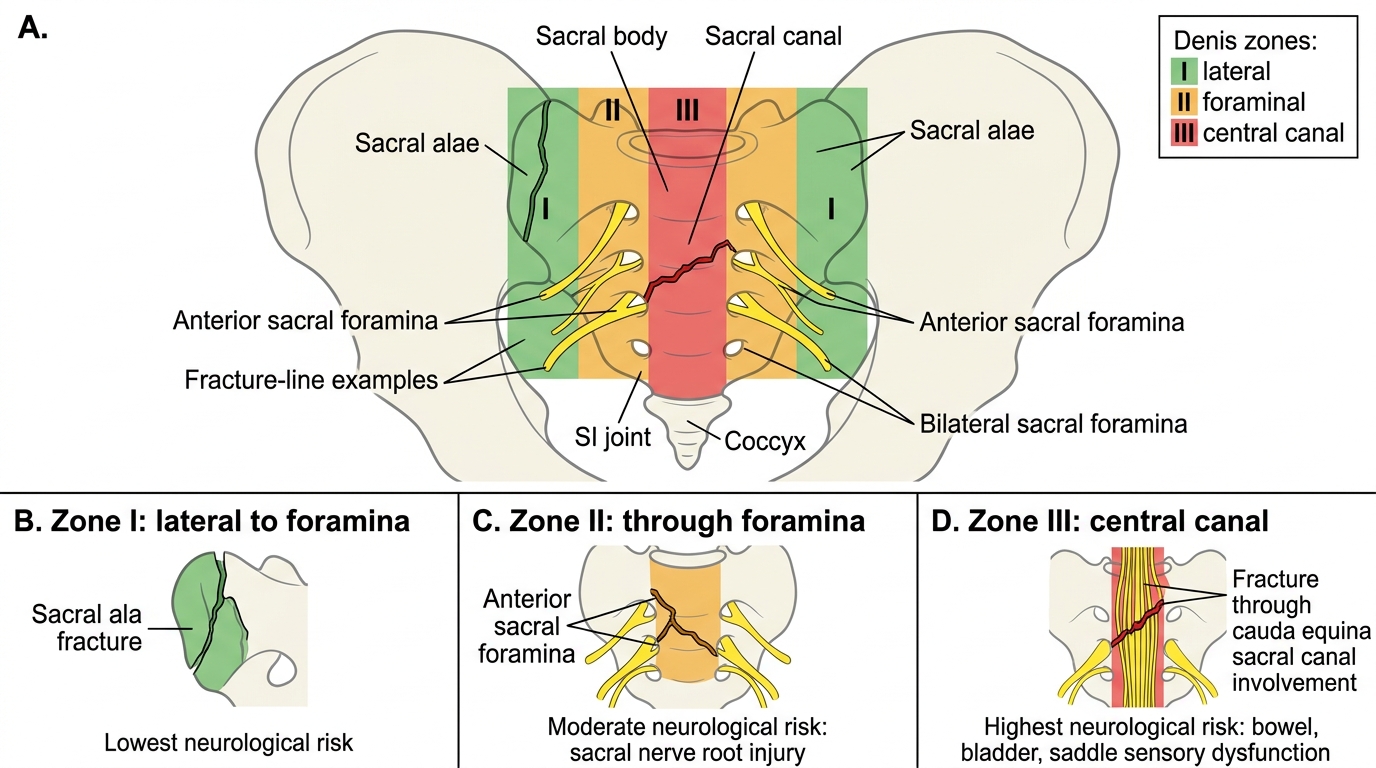
Denis Sacral Fracture Zones and Neurological Risk
SELF-CHECK
In a Young-Burgess APC-III pelvic fracture, which specific finding on X-ray confirms the diagnosis and predicts high haemorrhage risk?
A. Unilateral pubic rami fracture with posterior sacral crush
B. Symphysis diastasis >2.5 cm with complete SI joint disruption and posterior ligament rupture
C. Iliac wing fracture with intact posterior ring
D. Transverse acetabular fracture with femoral head dislocation
Reveal Answer
Answer: B. Symphysis diastasis >2.5 cm with complete SI joint disruption and posterior ligament rupture
APC-III is defined by symphysis diastasis >2.5 cm PLUS complete disruption of both anterior AND posterior SI ligaments, resulting in a widely open pelvis with no residual posterior stability. This is the highest-haemorrhage APC variant because the pelvis cannot tamponade venous bleeding and the internal iliac vessels are maximally stretched and torn. Option A describes LC-I; Option C describes an isolated wing fracture; Option D is an acetabular injury pattern.
Self-Assessment: Key Principles in Pelvic and Acetabular Injury
Having completed this module on pelvic and acetabular injuries, it is time to consolidate your understanding of the critical decision points that separate safe from unsafe practice. Trauma examiners in final MBBS consistently test whether a candidate can move from pattern recognition — correctly classifying an injury by mechanism and stability — to an immediate, prioritised management plan that accounts for haemodynamic status, imaging findings, and associated injuries. A student who can name all the Young-Burgess types but cannot describe why the pelvic binder must sit at the greater trochanters rather than the iliac crests, or who does not know that a negative FAST does not exclude retroperitoneal pelvic haemorrhage, will fail a trauma viva. Work through the questions below without referring back to the text. For each question, reason through the mechanism of injury, haemodynamic implications, classification, and management sequence before checking the explanation.
Key questions to consolidate your learning:
- Can you name all three haemorrhage sources in pelvic fractures and their approximate contributions?
- Can you place a pelvic binder correctly, at the right anatomical level, from memory?
- Can you state why a negative FAST does NOT exclude pelvic haemorrhage?
- Can you differentiate an APC-II from an APC-III injury on plain X-ray and explain the management difference?
- Can you describe the indications for angioembolisation vs pre-peritoneal packing?
- Can you state the current antibiotic timing guidance for open pelvic fractures (and why the 6-hour rule is obsolete)?
- Can you outline when acetabular fractures require ORIF vs conservative management?
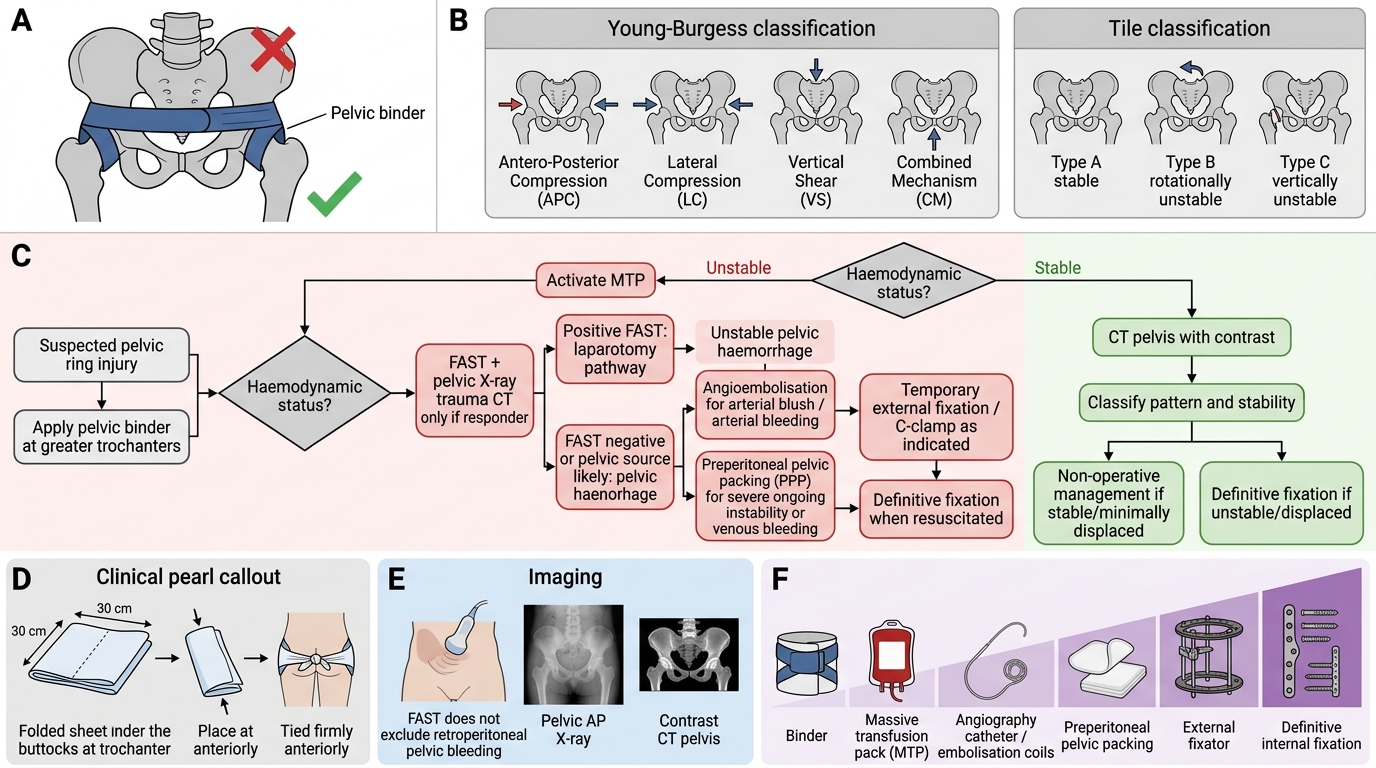
Pelvic Ring Injury Management Algorithm
Reflect on any concept where you hesitated. Return to the relevant section before your next clinical encounter. Pelvic trauma is unforgiving of knowledge gaps at the bedside.
CLINICAL PEARL
The pelvic binder must be placed at the level of the greater trochanters, not the iliac crests — placing it too high compresses the abdomen and impedes respiration without reducing pelvic volume. In a sheet application emergency, fold the sheet to ~30 cm width, slide under the patient at the buttock level, and tie firmly. Once applied, do NOT repeatedly test pelvic stability by compression or distraction — each 'spring test' risks clot disruption and can convert a tamponaded venous bleed into a catastrophic re-bleed. Another critical trap: a FAST-negative result does NOT exclude pelvic haemorrhage — retroperitoneal blood is invisible to FAST. When the FAST is negative in a haemodynamically unstable trauma patient, pelvic haemorrhage until proven otherwise.