Page 12 of 22
OR2.11 | Femoral Shaft Fracture and Fat Embolism Recognition — SDL Guide
Learning Objectives
- Describe the aetiopathogenesis, clinical features, and classification of femoral shaft fractures across all age groups
- Outline the blood loss estimation for femoral shaft fractures and the principles of initial resuscitation
- Explain the pathophysiology, Gurd criteria, and management of fat embolism syndrome (FES)
- Compare operative fixation methods for femoral shaft fractures — intramedullary nail, external fixation, and plating — with their indications
- Identify complications of femoral shaft fractures and recognise their clinical presentations
INSTRUCTIONS
Fracture of the femoral shaft is one of the most serious musculoskeletal injuries encountered in clinical practice. The femur is the strongest, most vascular bone in the body; its fracture liberates up to 1–2 litres of blood into the thigh and releases bone marrow fat into the systemic circulation, creating two independent threats to life: haemorrhagic shock and fat embolism syndrome. This module provides the clinical framework to assess, resuscitate, and initiate management of femoral shaft fractures in patients of all ages, from the newborn delivered by obstructed labour to the elderly patient with osteoporosis who falls from standing height.
References
- Maheshwari's Essential Orthopaedics, Ch 28 (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, 10th ed, Ch 28 (textbook)
- Ebnezar's Textbook of Orthopaedics, 5th ed (textbook)
- ATLS Student Manual, 10th ed (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 22-year-old man arrives by ambulance after a road traffic accident. His BP is 90/60 mmHg, pulse 120/min, and his left thigh is visibly shortened and externally rotated, with a tense thigh swelling and pallor of the overlying skin. You establish IV access and start fluid resuscitation. Twenty-four hours after surgical fixation with an intramedullary nail, the nursing staff notes that his oxygen saturation has dropped to 88% on room air, his temperature is 38.6°C, and he is confused and anxious. On examination, you see petechiae scattered across his upper chest and conjunctivae. What complication has developed, and what criteria will you use to confirm the diagnosis?
WHY THIS MATTERS
Femoral shaft fractures are a paradigm case for understanding polytrauma management. In India, road traffic accidents are the leading cause of these fractures in young adults, and the combination of volume loss, fat embolism risk, and the complexity of definitive fixation makes them a test of every doctor's basic emergency skills: recognition of haemorrhagic shock, fluid resuscitation, splinting, safe pain management, and — uniquely — the ability to recognise fat embolism syndrome in the post-operative period, when it is most frequently confused with pulmonary embolism or hospital-acquired pneumonia. Paediatric femoral fractures add another dimension, including non-accidental injury vigilance.
RECALL
Recall the anatomy of the femoral shaft: the femoral diaphysis extends from the lesser trochanter to the femoral condyles. The femoral artery descends along the anteromedial thigh, enters the adductor canal (subsartorial canal), and exits as the popliteal artery at the adductor hiatus; it is rarely injured in mid-shaft femoral fractures (the bone is surrounded by thick muscle) but may be involved with penetrating injuries or distal fractures. The femoral nerve (L2–L4) lies lateral to the femoral artery in the femoral triangle. The femoral shaft has three surfaces (anterior, posteromedial, posterolateral) and is supplied by the nutrient artery, a branch of the perforating vessels of the profunda femoris. The femoral vein accompanies the artery.
Aetiopathogenesis and Classification Across Age Groups
Femoral shaft fractures require considerable force in young adults because the diaphysis is a strong, thick-cortex bone surrounded by powerful muscle groups. In the young adult population, road traffic accidents and falls from height dominate; in older adults, low-energy falls on osteoporotic bone may suffice; in neonates, femoral shaft fracture during difficult vaginal delivery — especially breech extraction — is a well-recognised though rare complication; in children, non-accidental injury must always be considered when the mechanism does not fit the fracture pattern. Pathological fractures through bone weakened by metastatic disease, primary bone tumour, osteomyelitis, or Paget's disease are a distinct category — any fracture with a disproportionately low-energy mechanism or pre-fracture pain requires radiographic scrutiny for an underlying lesion.
The fracture can occur at any level of the shaft but is most common at the junction of the middle and distal thirds where the bone's bending stiffness is least. Fracture patterns include transverse (direct blow), oblique (combined loading), spiral (twisting), comminuted (high energy, multiple fragments), and segmental (two fracture levels creating a floating fragment). Comminuted and segmental fractures carry the greatest risk of blood loss and the greatest fixation challenge.
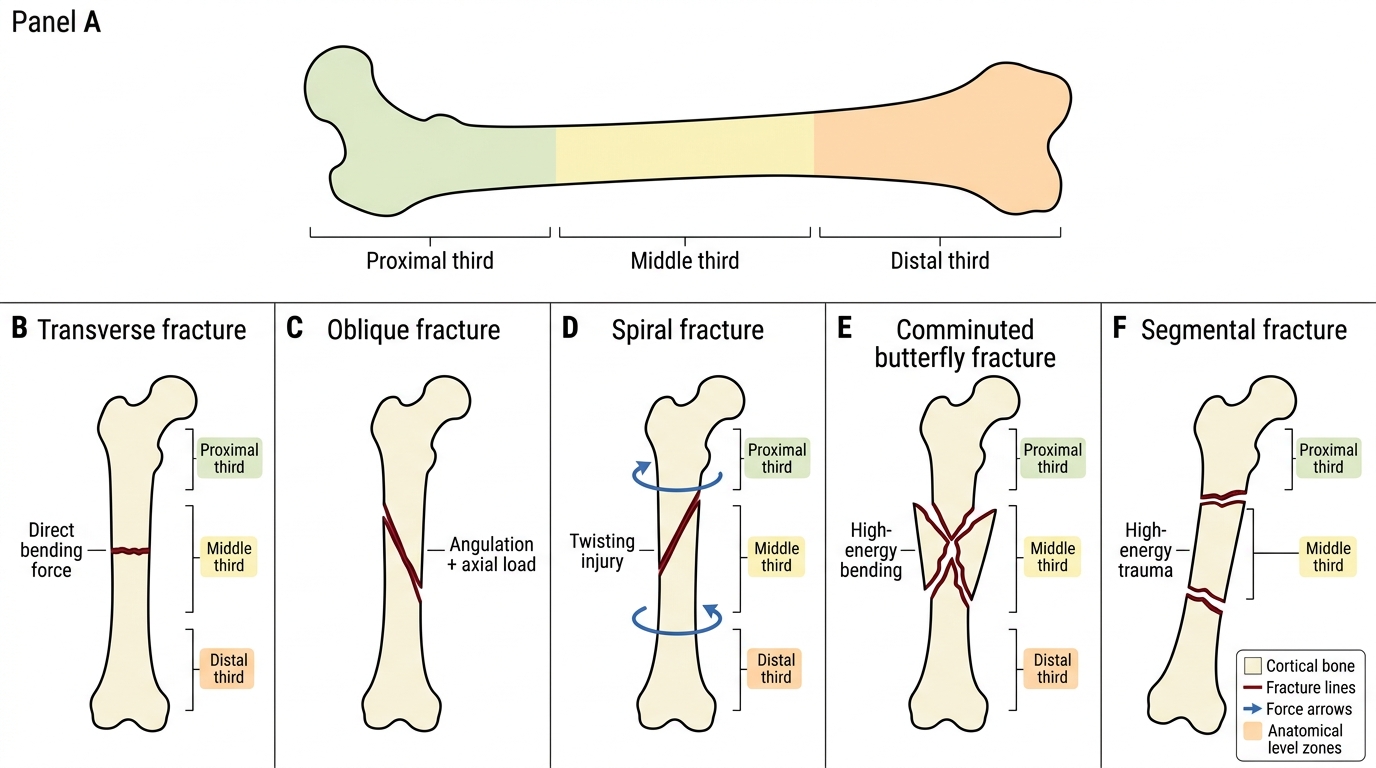
Femoral Shaft Fracture Patterns
Blood Loss and Haemorrhagic Shock Recognition
Provided image
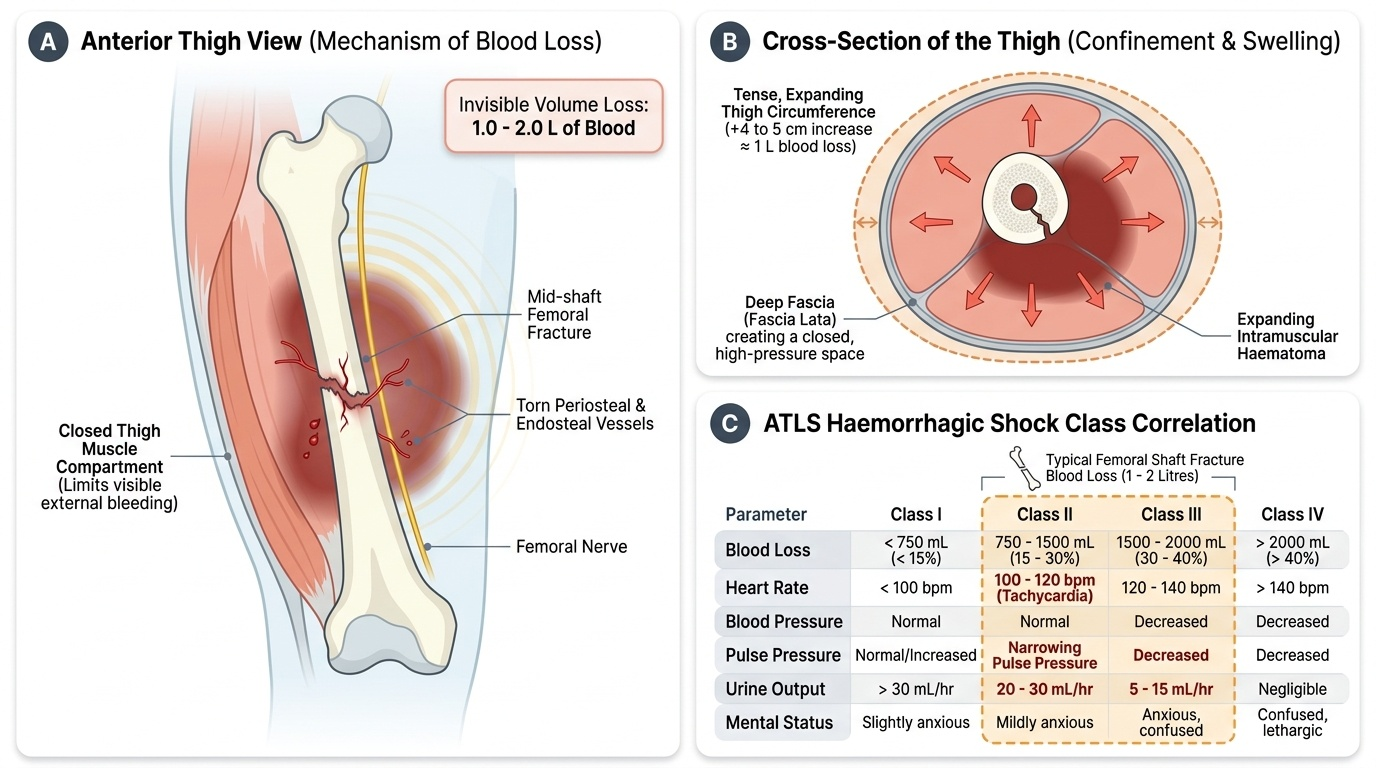
The femur is the most vascular long bone in the body. A closed femoral shaft fracture can be associated with a blood loss of 1–2 litres into the thigh (occasionally more in comminuted fractures or elderly patients) as the torn periosteum and endosteal vessels bleed freely into the thigh musculature. This volume loss, which is invisible on external inspection, is sufficient to produce Class II–III haemorrhagic shock (ATLS classification) — defined by progressive tachycardia, narrowing pulse pressure, and declining urine output. In a multiply injured patient with concurrent pelvic, abdominal, or chest injuries, the total volume loss may be immediately life-threatening.
The thigh swelling produced by haematoma is an important clinical sign: a tense, expanding thigh circumference increase of 4–5 cm over baseline represents approximately 1 litre of blood. External signs include shortening of the limb (proximal migration of the distal fragment under muscle pull), abnormal angulation, and pathological external rotation. The femur is innervated by the femoral nerve and periosteum; fracture is intensely painful, contributing to splinting and reflex vasoconstriction. Pain control (femoral nerve block or parenteral opioid) is both humanitarian and physiologically beneficial — reducing the sympathetic stress response.
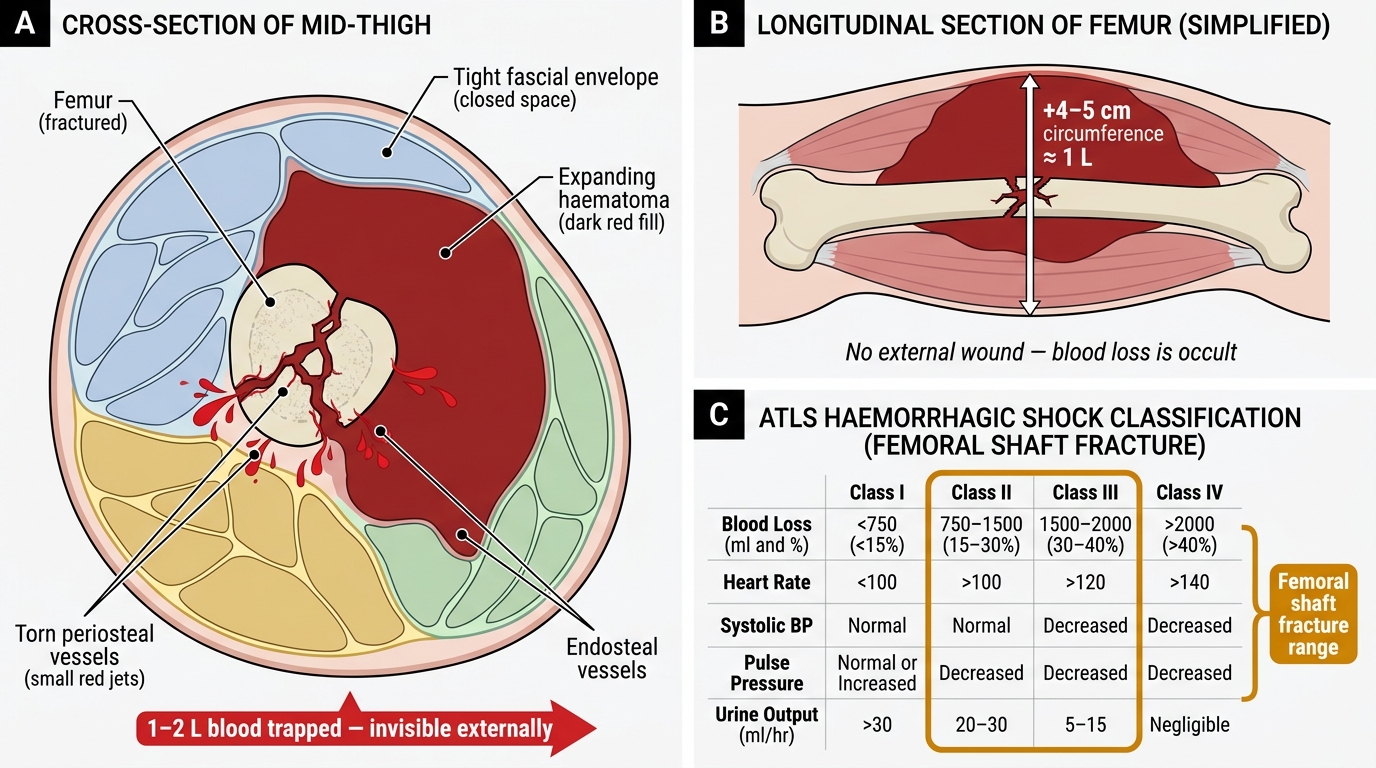
Blood Loss in Femoral Shaft Fracture: Compartment Haematoma and ATLS Shock Correlation
Clinical Features and Initial Assessment
The clinical presentation of a femoral shaft fracture is rarely subtle. The patient presents in pain with an inability to bear weight or move the affected limb. On inspection, the thigh appears shortened (2–6 cm of visible shortening from proximal fragment riding up under gluteal muscle pull), swollen, and externally rotated (the pull of the iliopsoas rotates the proximal fragment). Crepitus and abnormal mobility may be apparent but should not be elicited deliberately. Any wound in the vicinity must be assumed to communicate with the fracture until proven otherwise — constituting an open fracture with its antibiotic-timing implications. In proximal third fractures, the pull of iliopsoas on the proximal fragment causes it to flex, abduct, and externally rotate; middle third fractures show overlapping fragments; distal third fractures flex the distal fragment under the pull of the gastrocnemius, creating a risk of popliteal vessel compression.
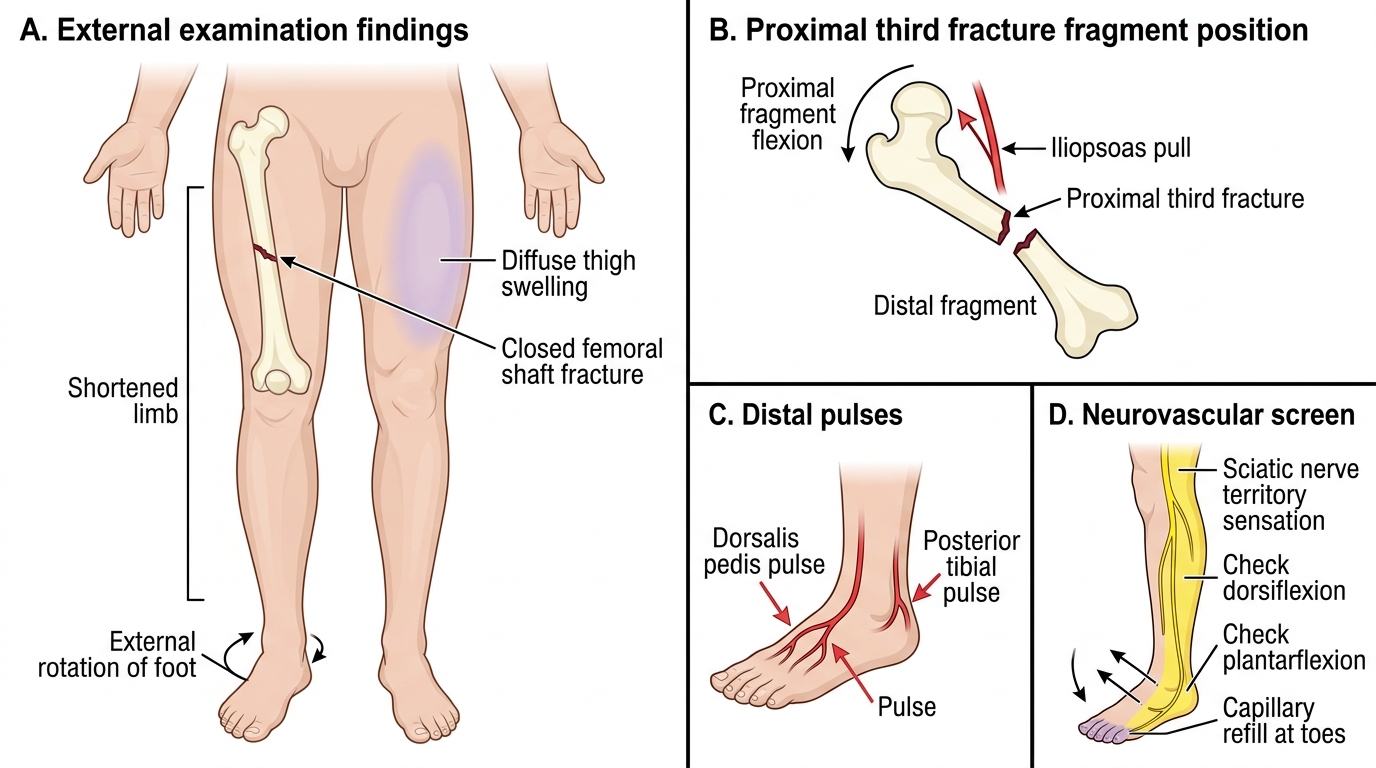
External Examination of Femoral Shaft Fracture
PRIMARY SURVEY (ATLS ABCDE): airway and breathing are rarely compromised by an isolated femoral fracture, but if the patient is polytraumatised, these must be confirmed first. Circulation is the critical step: assess BP, pulse rate, capillary refill, and mental status (GCS). Establish two large-bore IV lines; initiate resuscitation with crystalloid (isotonic saline or Ringer's lactate) while blood is being cross-matched. Immobilise the fracture in a Thomas splint (emergency) or traction splint to reduce pain and decrease ongoing blood loss into the thigh.
Neurovascular examination: assess dorsalis pedis and posterior tibial pulses, capillary refill, sensation in the feet (sciatic distribution below the knee), and motor power (dorsiflexion/plantarflexion). Document findings before and after splintage.
SELF-CHECK
A 25-year-old man with a closed mid-shaft femoral fracture after a road traffic accident has BP 95/65 mmHg, pulse 118/min, and is anxious but responsive. According to ATLS classification, what class of haemorrhagic shock is this, and what is the estimated blood loss?
A. Class I shock — blood loss <750 mL
B. Class II shock — blood loss 750–1500 mL
C. Class III shock — blood loss 1500–2000 mL
D. Class IV shock — blood loss >2000 mL
Reveal Answer
Answer: C. Class III shock — blood loss 1500–2000 mL
Class III haemorrhagic shock (blood loss 1500–2000 mL, 30–40% of blood volume) is characterised by BP <100 mmHg, pulse >120/min, altered mental status (anxiety, confusion), and decreased urine output. A femoral shaft fracture can account for 1–2 L of blood loss into the thigh. The blood pressure drop to 95/65 and pulse of 118 place this firmly in Class III, requiring immediate fluid resuscitation and urgent surgical planning.