Page 13 of 22
OR2.11 | Femoral Shaft Fracture and Fat Embolism Recognition — SDL Guide (Part 2)
Fat Embolism Syndrome — Pathophysiology and Gurd Criteria
Fat embolism syndrome (FES) is a systemic clinical syndrome that develops when fat droplets enter the systemic circulation — most commonly after long bone fractures (especially femoral shaft), major orthopaedic procedures (intramedullary nailing, joint arthroplasty), and rarely non-traumatic conditions such as pancreatitis and sickle cell crisis. The pathophysiology involves two phases. In the mechanical phase, bone marrow fat globules (size >8 µm) are forced into disrupted intramedullary venous sinusoids at the time of fracture or during intramedullary manipulation; they traverse the pulmonary capillaries directly (or via a patent foramen ovale) to reach the systemic circulation. In the biochemical phase, circulating free fatty acids (liberated by lipase action on fat globules) trigger endothelial inflammation, microvascular injury, and surfactant destruction, leading to non-cardiogenic pulmonary oedema and dysfunction resembling acute respiratory distress syndrome (ARDS).
The clinical syndrome typically manifests 24–72 hours after the precipitating event. The classical triad: (1) Respiratory compromise — hypoxia (PaO₂ <60 mmHg on room air), tachypnoea, and progressive dyspnoea; (2) Neurological signs — confusion, agitation, drowsiness, rarely focal deficits; (3) Petechial rash — the pathognomonic feature, appearing on the conjunctivae, anterior axillary folds, and upper chest/neck, caused by fat emboli in dermal capillaries.
The Gurd and Wilson criteria provide the standard diagnostic framework, requiring at least one major criterion plus at least one minor criterion plus laboratory evidence:
Major criteria:
- Axillary or subconjunctival petechiae
- Hypoxaemia (PaO₂ <60 mmHg; FiO₂ 0.4)
- Central nervous system depression (disproportionate to hypoxaemia)
- Pulmonary oedema on chest radiograph
Minor criteria:
- Tachycardia >110/min
- Pyrexia >38.5°C
- Emboli in the retina (fat globules, retinal exudates/haemorrhage)
- Fat in urine (lipaemia, lipuria)
- Sudden unexplained drop in haematocrit or platelet count
- Increasing erythrocyte sedimentation rate (ESR)
- Fat globules in sputum
Laboratory evidence: fat macroglobulinaemia
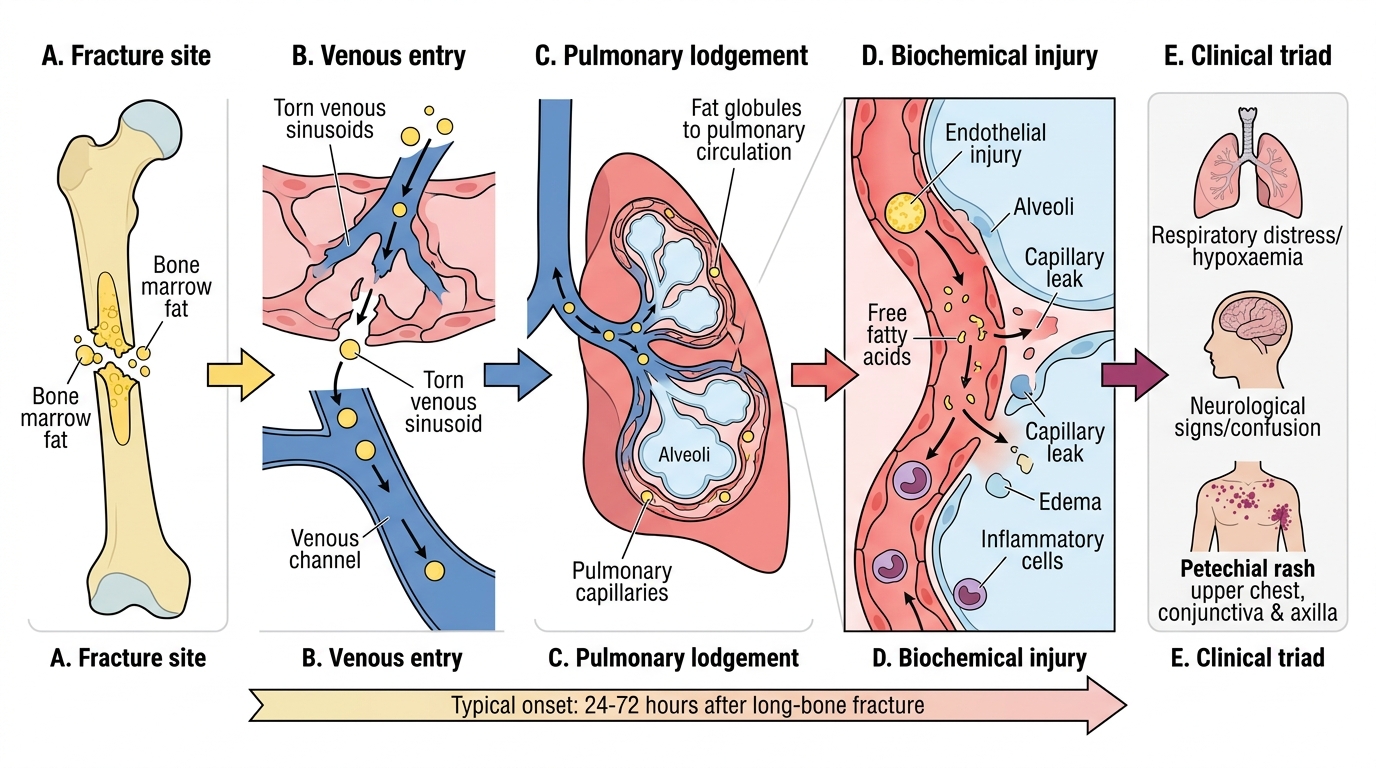
Pathophysiology of Fat Embolism Syndrome
Investigation and Imaging
For the femoral shaft fracture itself, plain radiography of the full femur including the hip (AP and lateral views) and the knee joint is mandatory. The radiograph defines the fracture level, pattern, and any comminution or segmental configuration. The hip and knee views are essential because associated hip dislocation (rare) or distal fracture (segmental pattern) will change the surgical approach entirely. CT is rarely needed for the shaft itself but may be required for the periarticular extensions or associated pelvic injuries.
For suspected fat embolism syndrome: chest radiograph may show bilateral diffuse alveolar opacities (white-out, indistinguishable from ARDS), although the chest X-ray may be normal in early FES. Pulse oximetry should be monitored continuously; arterial blood gas (ABG) is the definitive respiratory assessment — PaO₂ <60 mmHg on room air is diagnostic criteria. High-resolution CT chest (HRCT) shows bilateral ground-glass opacification. Bronchoalveolar lavage may reveal fat-laden macrophages (>5% of macrophages containing lipid), though this is not universally available. A full blood count typically shows anaemia and thrombocytopenia; coagulation screen may show a consumptive coagulopathy pattern.
Neuroimaging with CT/MRI brain is indicated when neurological symptoms are disproportionate to hypoxaemia; MRI may show scattered petechial haemorrhages in the deep white matter and watershed zones in severe FES.
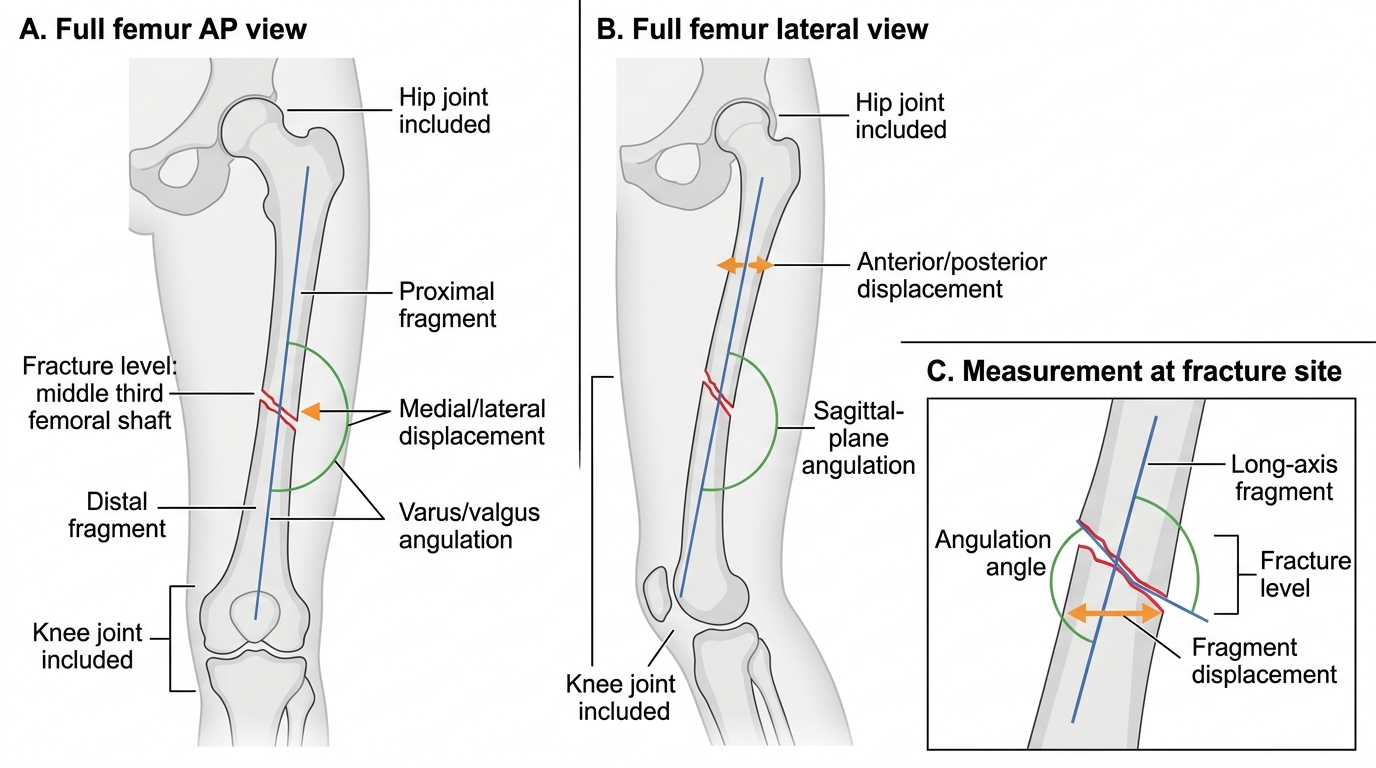
Required Radiographic Views for Femoral Shaft Fracture
Management of Femoral Shaft Fractures — All Age Groups
The definitive management of femoral shaft fractures in adults has been transformed by intramedullary nailing (IMN), now the gold standard for virtually all closed and most open femoral shaft fractures in adults. The antegrade nail is inserted through the piriformis fossa or greater trochanteric tip, is locked proximally and distally, and provides immediate stability that allows early weight-bearing and rehabilitation. The advantages over earlier methods — skin or skeletal traction, external fixation, and open plating — are well established: lower infection rate, shorter hospital stay, earlier rehabilitation, and superior biomechanical stability. Early definitive fixation (within 24 hours in haemodynamically stable patients) reduces the risk of fat embolism syndrome, pulmonary complications, and the morbidity of prolonged immobilisation.
Age-specific management principles:
- Neonates: Femoral shaft fractures from birth trauma are managed with skin traction (Gallows traction in infants <18 months, where both legs are suspended vertically) or a Pavlik harness; remodelling is excellent and perfect anatomical reduction is not required.
- Children (2–10 years): Traction (skin traction, then hip spica casting) is appropriate for younger children. Flexible (elastic) intramedullary nailing (FWIN/Nancy nails) is increasingly used for children aged 5–11 years; it avoids the complications of open growth plates.
- Adolescents (>11 years): Standard reamed locked intramedullary nails, similar to adults, are used once the proximal femoral physis is closing.
- Elderly: Standard IMN in most cases; if pathological fracture, the underlying pathology (metastasis, Paget's) dictates whether adjuvant surgery (cemented nail, prosthesis) or systemic oncology treatment is also required.
- Damage control situations: In the haemodynamically unstable multiply injured patient, temporary external fixation ('damage control orthopaedics') stabilises the fracture rapidly with minimal anaesthetic time; definitive IMN is deferred 3–5 days until the patient's physiological parameters are corrected.
Open femoral shaft fractures require Gustilo-Anderson grading, emergency intravenous antibiotics within 1 hour of presentation (cephalosporin ± aminoglycoside for Grade III), tetanus prophylaxis, thorough surgical debridement, and either definitive IMN or external fixation depending on contamination grade.
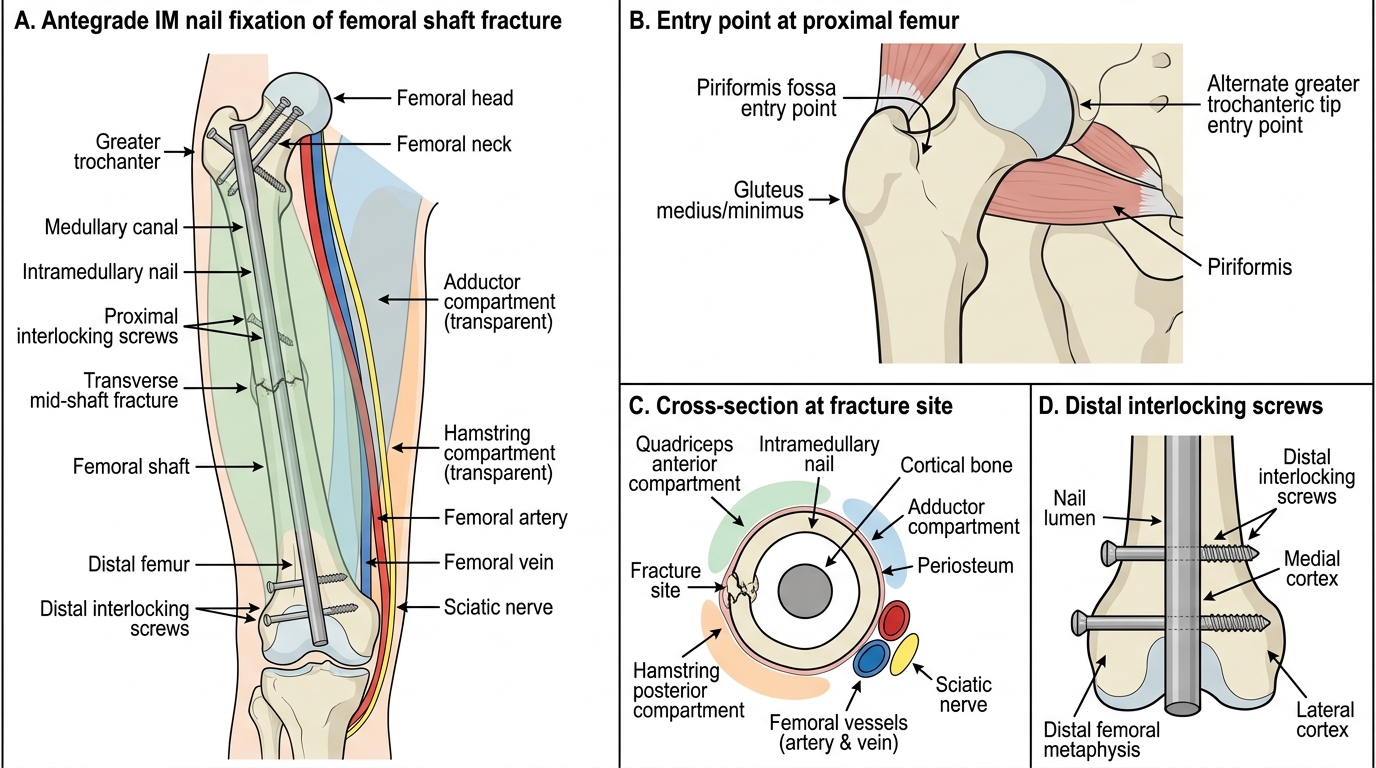
Antegrade Intramedullary Nailing of Femoral Shaft Fracture