Page 14 of 22
OR2.11 | Femoral Shaft Fracture and Fat Embolism Recognition — SDL Guide (Part 3)
Management of Fat Embolism Syndrome
The management of fat embolism syndrome is primarily supportive — there is no specific antidote to reverse the circulating fat emboli or the biochemical cascade. Early fracture fixation (especially intramedullary nailing) is the most effective preventive measure, as it reduces ongoing bone marrow fat release. Once FES is established, the following principles apply:
Respiratory support: supplemental oxygen to maintain SpO₂ >95% is the immediate intervention. Moderate-to-severe FES with PaO₂ <60 mmHg despite supplemental oxygen requires high-flow oxygen via non-rebreather mask; progressive respiratory failure (ARDS pattern) requires mechanical ventilation with lung-protective settings (low tidal volume 6 mL/kg ideal body weight, PEEP). Continuous pulse oximetry monitoring is mandatory.
Haemodynamic support: maintain euvolaemia; avoid both fluid overload (worsens pulmonary oedema) and hypovolaemia. Vasopressors may be needed in severe cases.
Pharmacological adjuncts: corticosteroids (methylprednisolone) have been used both as prophylaxis (before high-risk procedures) and in established FES to attenuate the inflammatory response, but their benefit is not definitively established in randomised controlled trials — they are used selectively. Heparin (unfractionate) has theoretical benefit in promoting lipase activity to clear fat globules, but is not standard therapy.
Specific monitoring: serial ABGs, chest radiograph, haematocrit, and platelet count; neurological observations hourly in the acute phase.
The natural history: mild FES resolves spontaneously over 3–7 days with supportive care. Severe FES with ARDS carries a mortality of 5–10% in specialised centres.
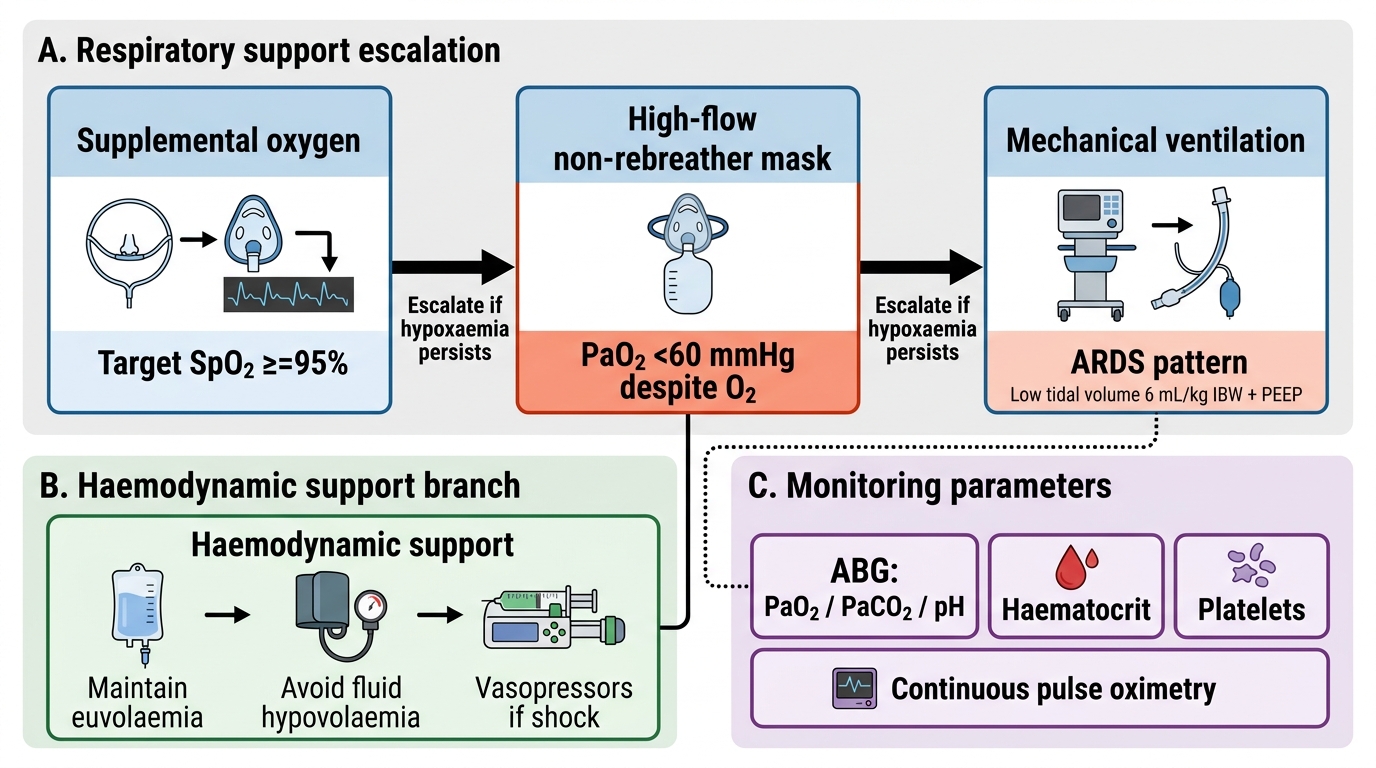
Management Algorithm for Fat Embolism Syndrome
SELF-CHECK
A patient develops fat embolism syndrome 36 hours after femoral shaft fracture fixation. Which combination of findings satisfies the Gurd major criteria for diagnosis?
A. Tachycardia 120/min, fever 38.8°C, and elevated ESR
B. Petechial rash over the chest and axillae, PaO₂ 55 mmHg, and sudden confusion
C. Lipuria, thrombocytopenia, and bilateral opacities on chest X-ray
D. Fat globules in sputum, retinal emboli, and elevated haematocrit
Reveal Answer
Answer: B. Petechial rash over the chest and axillae, PaO₂ 55 mmHg, and sudden confusion
The Gurd major criteria include: axillary/subconjunctival petechiae, hypoxaemia (PaO₂ <60 mmHg on FiO₂ 0.4 or room air), central nervous system depression, and pulmonary oedema. Option B includes the pathognomonic petechial rash, documented hypoxaemia (PaO₂ 55 mmHg), and CNS change (confusion) — three major criteria. Options A and C consist primarily of minor criteria. Diagnosis requires ≥1 major + ≥1 minor + laboratory evidence.
Self-Assessment — Femoral Shaft Fractures and Fat Embolism
Provided image
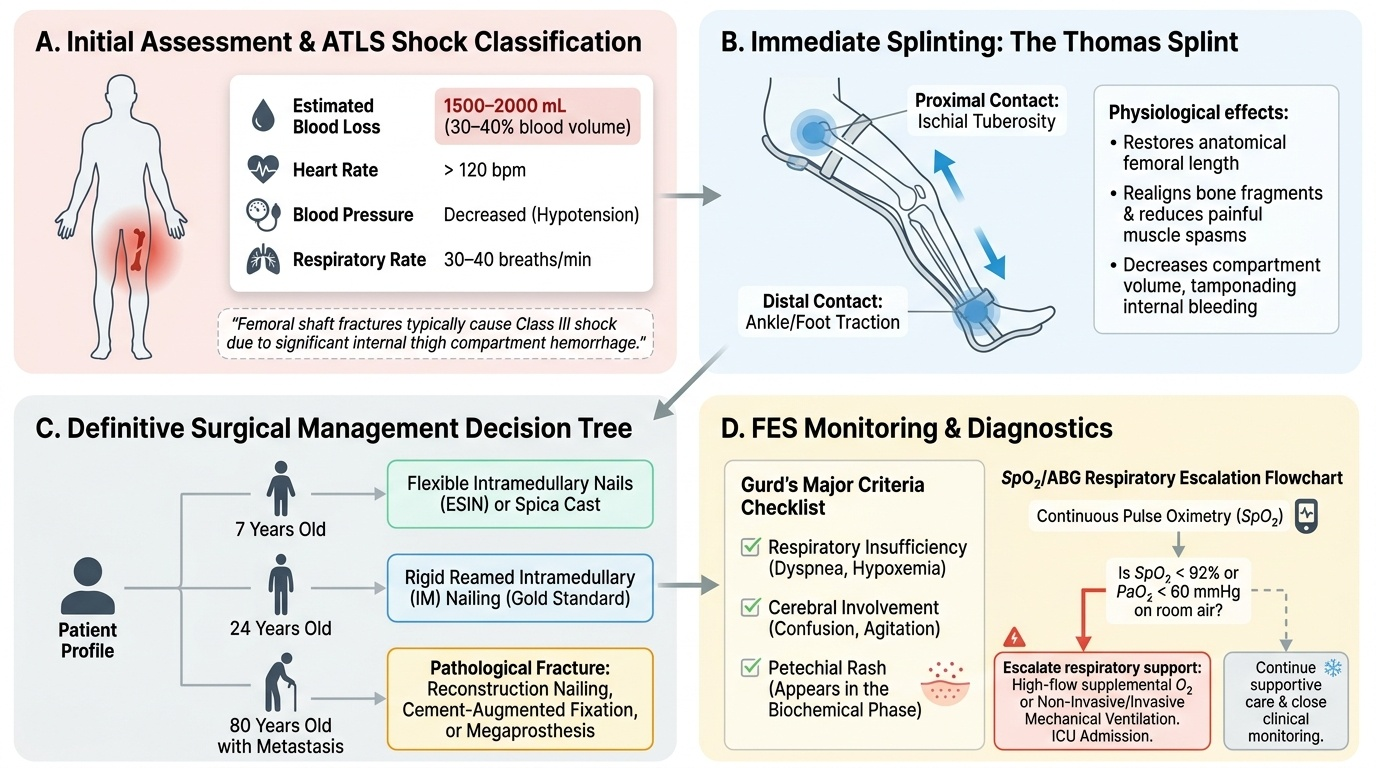
This self-assessment section consolidates the core concepts of femoral shaft fracture management and fat embolism syndrome. Work through the following structured questions to verify your understanding of the key clinical principles covered in this module. First, rehearse the ATLS haemorrhagic shock classification: what blood pressure, pulse rate, and estimated blood loss characterise Class III shock, and why does a femoral shaft fracture typically produce this class? Second, apply the Thomas splint principle: what biomechanical mechanism makes immediate splintage reduce blood loss, and what is the two-point contact at which the splint stabilises? Third, for fat embolism syndrome: list the three elements of the Gurd major criteria triad and state the pathophysiology phase (mechanical vs biochemical) in which the petechial rash appears. Fourth, for age-specific management: state the appropriate fixation method for a femoral shaft fracture in a 7-year-old child versus a 24-year-old adult versus an 80-year-old with a pathological fracture through a metastatic deposit. Fifth, state the essential monitoring parameter for FES and the oxygen saturation threshold that mandates escalation of respiratory support beyond supplemental oxygen.
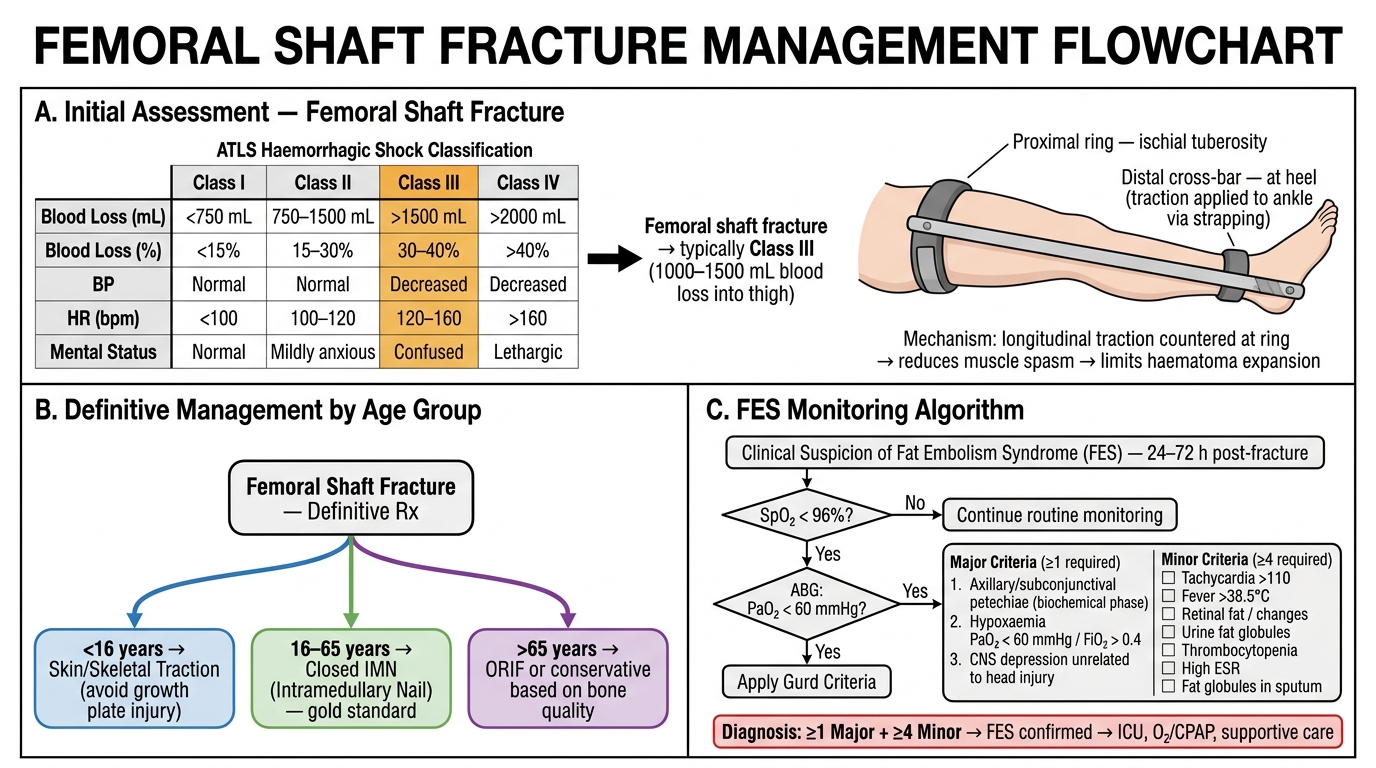
Femoral Shaft Fracture — Self-Assessment Summary: ATLS Classification, Thomas Splint, Age-Based Management, and FES Algorithm
CLINICAL PEARL
Two rules for femoral shaft fractures: (1) The blood loss into a closed femoral shaft fracture is invisible but real — 1–2 litres into the thigh muscle envelope. Any patient with a femoral fracture must be managed with the same resuscitation urgency as one with visible external haemorrhage. Apply a Thomas splint immediately, establish IV access, and start fluid replacement before completing the secondary survey. (2) The development of confusion, hypoxia, and petechiae at 24–72 hours after a femoral fracture is fat embolism syndrome until proven otherwise. The petechial rash on the upper chest, axillary folds, and conjunctivae is the clinical hallmark — look for it in every post-operative femoral fracture patient.