Page 1 of 22
OR2.1 | Clavicle Fracture Management — SDL Guide
Learning Objectives
- Describe the common mechanisms of clavicle fracture and the anatomical basis for displacement at each third
- Identify the clinical features and imaging findings that establish the diagnosis and guide management
- Classify clavicle fractures using the Allman system and understand how classification drives treatment decisions
- Outline non-operative and operative management options and their indications
- Recognise and manage neurovascular and pulmonary complications of clavicle fractures
INSTRUCTIONS
The clavicle is the most commonly fractured bone in the body, accounting for approximately 5% of all fractures presenting to emergency departments. As a final-year student about to enter clinical rotations, you will encounter clavicle fractures in casualty, fracture clinics, and on the wards. Understanding the anatomy of displacement, the Allman classification, and the evidence-based shift toward operative fixation for displaced mid-shaft fractures will equip you to participate meaningfully in management decisions from day one.
References
- Maheshwari's Essential Orthopaedics, 5th ed., Ch 20 -- Fractures of the Shoulder Girdle (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, 10th ed., Ch 29 -- Injuries of the Shoulder (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 22-year-old motorcyclist is brought to the emergency department after a high-speed collision. He is conscious, holding his left arm across his chest, and reports severe left shoulder pain. On inspection there is visible deformity with a prominent bony step at the mid-clavicle, swelling, and skin tenting. He cannot abduct the arm. A plain anteroposterior (AP) radiograph of the shoulder girdle confirms a displaced mid-shaft clavicle fracture with shortening of 2.5 cm and a butterfly fragment. How will you manage this injury, and which features make operative fixation appropriate?
WHY THIS MATTERS
The clavicle serves as the only bony link between the axial skeleton and the upper limb, and fractures here affect the whole shoulder mechanism. Mid-shaft fractures (Allman Group I) are by far the most common and have undergone a significant management revolution in the last two decades: evidence now supports operative fixation for substantially displaced or shortened fractures because non-operative treatment carries a clinically meaningful non-union rate and poorer functional outcomes in this subset. Understanding the anatomy of displacement, the complications relevant to the subclavian vessels and brachial plexus, and the indications for urgent surgery versus elective versus conservative management is essential clinical knowledge for every doctor who covers a casualty.
RECALL
Before proceeding, recall from your anatomy studies that the clavicle articulates medially with the manubrium (sternoclavicular joint) and laterally with the acromion (acromioclavicular joint). The subclavian vessels and the brachial plexus traverse the costoclavicular space deep to the mid-clavicle. The trapezius elevates the proximal fragment; the pectoralis major and the weight of the upper limb displace the distal fragment downward and medially. Also recall the two major methods of fracture management: non-operative (immobilisation with a sling or figure-of-eight bandage) and operative (plate-and-screw fixation or intramedullary nailing).
Anatomy and Mechanism of Injury
Provided image
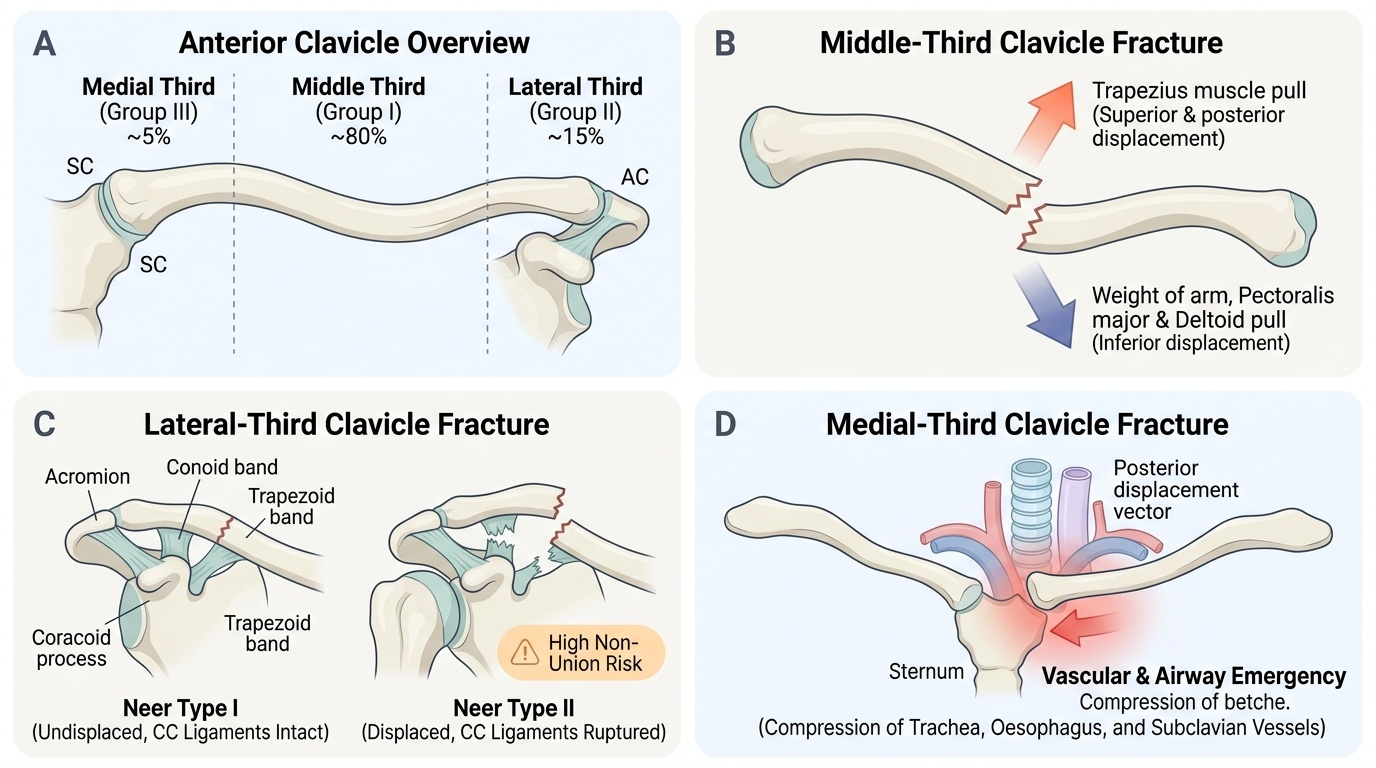
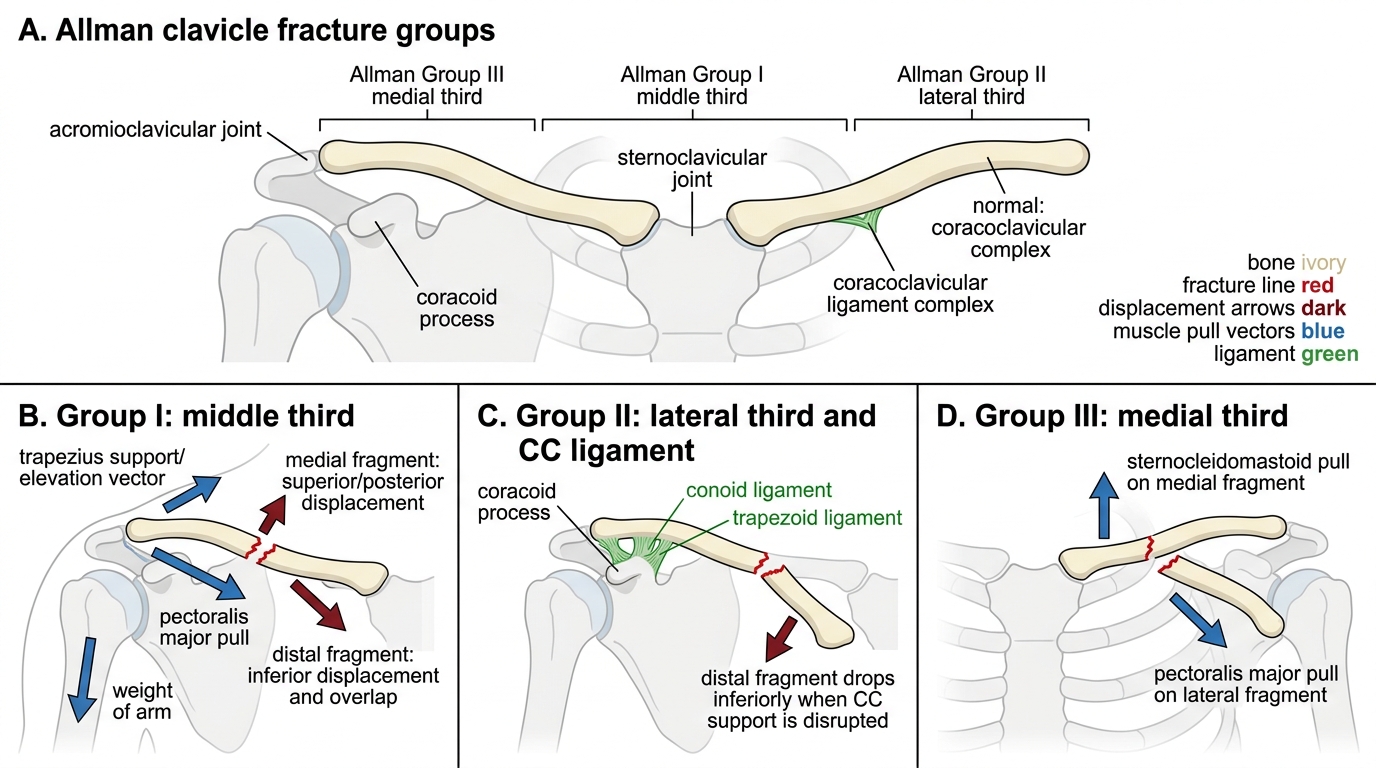
The clavicle is an S-shaped bone whose middle third -- being the narrowest and least protected -- accounts for roughly 80% of all clavicle fractures. The lateral third accounts for approximately 15% and the medial third for around 5%. Understanding how each fracture displaces requires knowledge of the muscular and ligamentous attachments. At the mid-shaft the trapezius pulls the medial fragment upward and posteriorly, while the weight of the arm, combined with the pull of the pectoralis major and deltoid, drops the distal fragment downward and shortens the overall clavicular length. This classic deformity creates the visible step that allows a bedside diagnosis in many cases. At the lateral third, the coracoclavicular ligaments (conoid and trapezoid) anchor the proximal fragment to the coracoid, while the distal fragment displaces inferiorly -- these ligaments are intact in undisplaced lateral third fractures (Neer type I) but disrupted in displaced ones (Neer type II), which behave more like acromioclavicular joint disruptions and carry a higher non-union risk. Medial third fractures are rare because the robust costoclavicular ligament limits displacement; however, posterior dislocation of the medial fragment is a vascular emergency because it can compress the trachea, oesophagus, or subclavian vessels. The two dominant mechanisms are a direct blow to the shoulder (fall on an outstretched arm or contact sport) and, less commonly, direct impact over the clavicle itself.
Allman Classification of Clavicle Fractures
- Mid-shaft (Allman Group I): ~80%; trapezius elevates medial fragment, arm weight depresses distal fragment
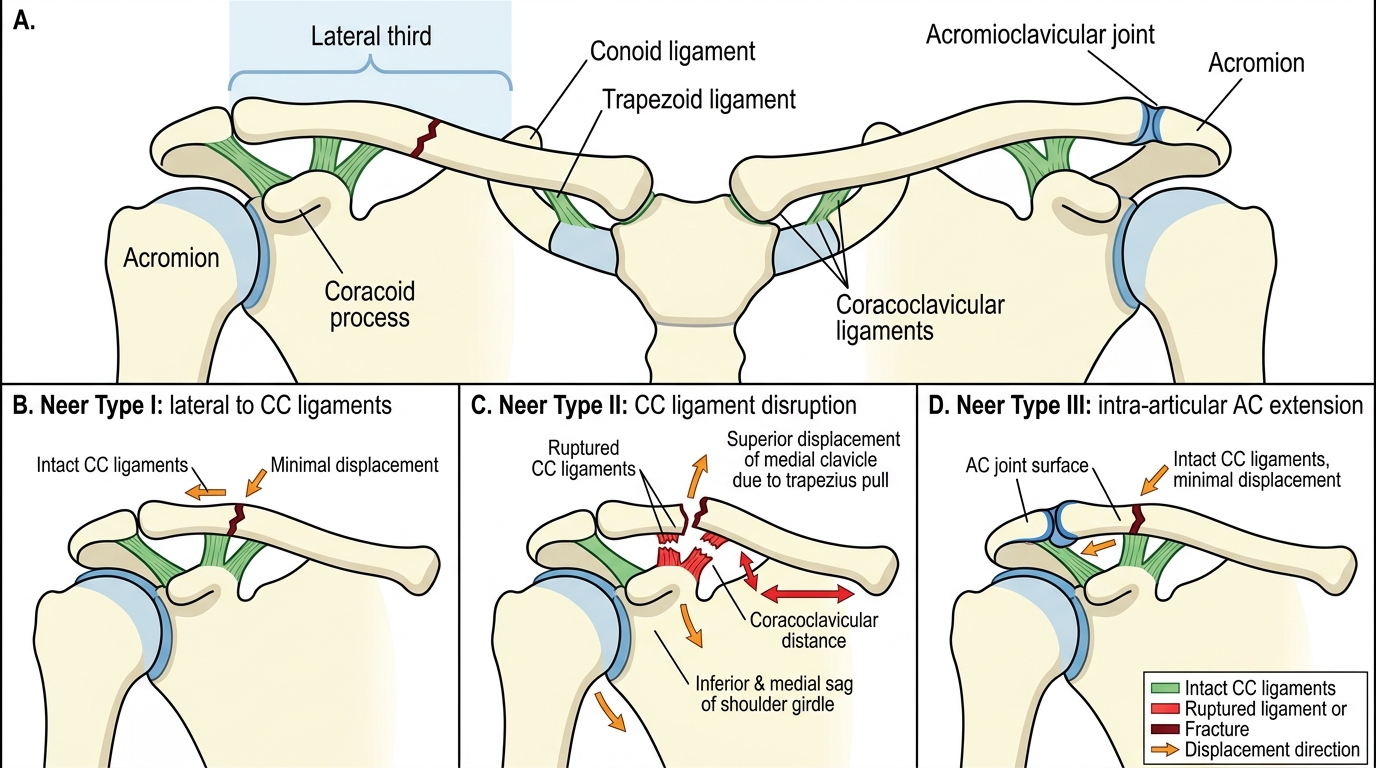
- Lateral third (Allman Group II / Neer types I-III): ~15%; non-union risk increases in displaced (Neer type II) because coracoclavicular ligaments are ruptured
- Medial third (Allman Group III): ~5%; posterior displacement can threaten mediastinal structures
Pathological Anatomy and Fracture Classification
The Allman classification (1967), updated by Neer for the lateral third, remains the standard system in clinical use. Allman divided clavicle fractures by location into three groups: Group I (middle third), Group II (lateral third), and Group III (medial third). The Neer subclassification of Group II fractures is clinically important because it stratifies non-union risk: Neer type I (minimal displacement, coracoclavicular ligaments intact), Neer type II (displaced, ligaments disrupted -- highest non-union risk, up to 30-40%), and Neer type III (intra-articular, extending into the acromioclavicular joint). For mid-shaft fractures, the Edinburgh classification by Robinson provides further prognostic granularity, subdividing by displacement and comminution into types 2A (undisplaced/minimal) and 2B (displaced). In terms of fracture morphology, the key descriptor for management is shortening of >=2 cm and complete displacement (no cortical contact), as these are the strongest evidence-based predictors of non-union when managed non-operatively. Open fractures and skin tenting (impending skin compromise) are additional indications for early surgery. Comminution increases instability and is relevant to implant selection.
Neer Classification of Lateral Third Clavicle Fractures
| Group | Location | Key feature | Non-union risk |
|---|---|---|---|
| I (mid-shaft) | Middle third | Trapezius elevates proximal fragment | ~2% undisplaced; ~15% displaced >=2 cm |
| II Neer I | Lateral third, ligaments intact | Minimal displacement | Low |
| II Neer II | Lateral third, ligaments ruptured | Displaced, coracoclavicular gap widened | 30-40% |
| III | Medial third | Posterior dislocation = emergency | Low |
Clinical Examination and Imaging
Provided image
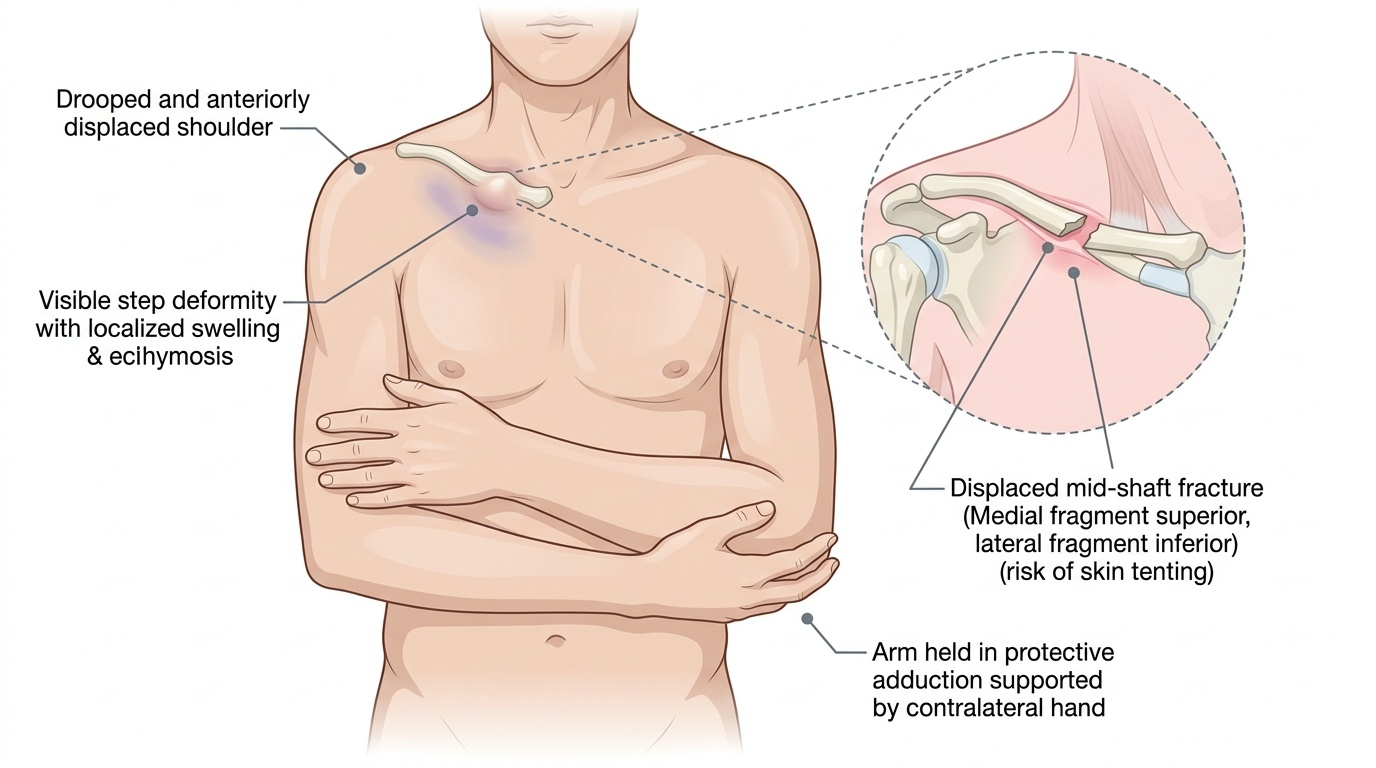
The clinical evaluation of a suspected clavicle fracture begins with a rapid trauma assessment in the high-energy setting, ensuring haemodynamic stability before focusing on the limb. The patient classically supports the injured arm across the chest with the contralateral hand (protective adduction), and the shoulder droops downward and anteriorly. Inspection reveals localised swelling, ecchymosis, and often a visible bony step or prominence at the fracture site. Skin tenting -- where the bone end pushes acutely against the overlying dermis -- must be noted as it mandates urgent surgical attention to prevent skin breakdown. Palpation elicits point tenderness; crepitus may be felt but should not be actively elicited. A complete neurovascular examination of the upper limb is mandatory: assess radial, ulnar, brachial, and axillary pulses; check capillary refill; and test sensation and power in the median, radial, ulnar, musculocutaneous, and axillary nerve distributions. Brachial plexus injury, though uncommon, occurs in high-energy fractures and must not be missed. Chest auscultation and percussion should screen for pneumothorax in high-energy mechanisms, particularly with associated rib fractures.
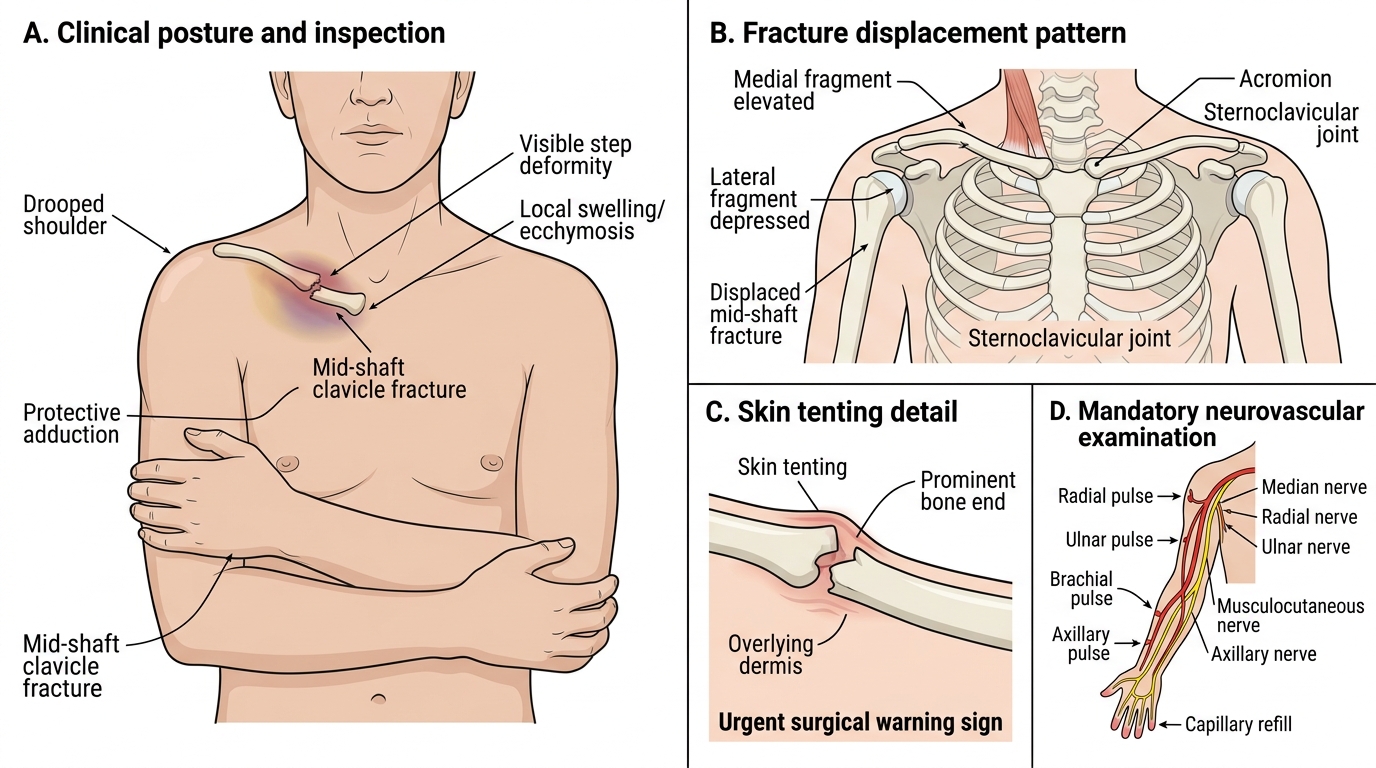
Clinical Signs of Displaced Mid-Shaft Clavicle Fracture
Standard radiographs:
- AP clavicle (not AP shoulder -- the whole clavicle must be visible)
- 15-degree cephalad (Zanca) view: best for lateral third fractures
- CT with 3D reconstruction: for comminuted, medial third, or pre-operative planning
- Measure shortening on AP: >2 cm compared to contralateral side is a key operative threshold
SELF-CHECK
A 28-year-old cyclist falls on the point of the shoulder. Radiograph shows a lateral third clavicle fracture with widening of the coracoclavicular space. Which Neer type is this, and what is its significance?
A. Neer type I -- ligaments intact, conservative management appropriate, low non-union risk
B. Neer type II -- coracoclavicular ligaments disrupted, high non-union risk (~30-40%), often requires fixation
C. Neer type III -- intra-articular, requires arthroscopic assessment
D. Allman Group III -- medial third, posterior dislocation likely
Reveal Answer
Answer: B. Neer type II -- coracoclavicular ligaments disrupted, high non-union risk (~30-40%), often requires fixation
Widening of the coracoclavicular space indicates disruption of the conoid and trapezoid ligaments -- this is the defining feature of Neer type II. The medial fragment is tethered to the coracoid while the lateral fragment displaces inferiorly, creating an unstable injury with a 30-40% non-union rate when managed conservatively. Neer type I fractures have intact ligaments; type III are intra-articular.