Page 2 of 22
OR2.1 | Clavicle Fracture Management — SDL Guide (Part 2)
Management Principles
Provided image
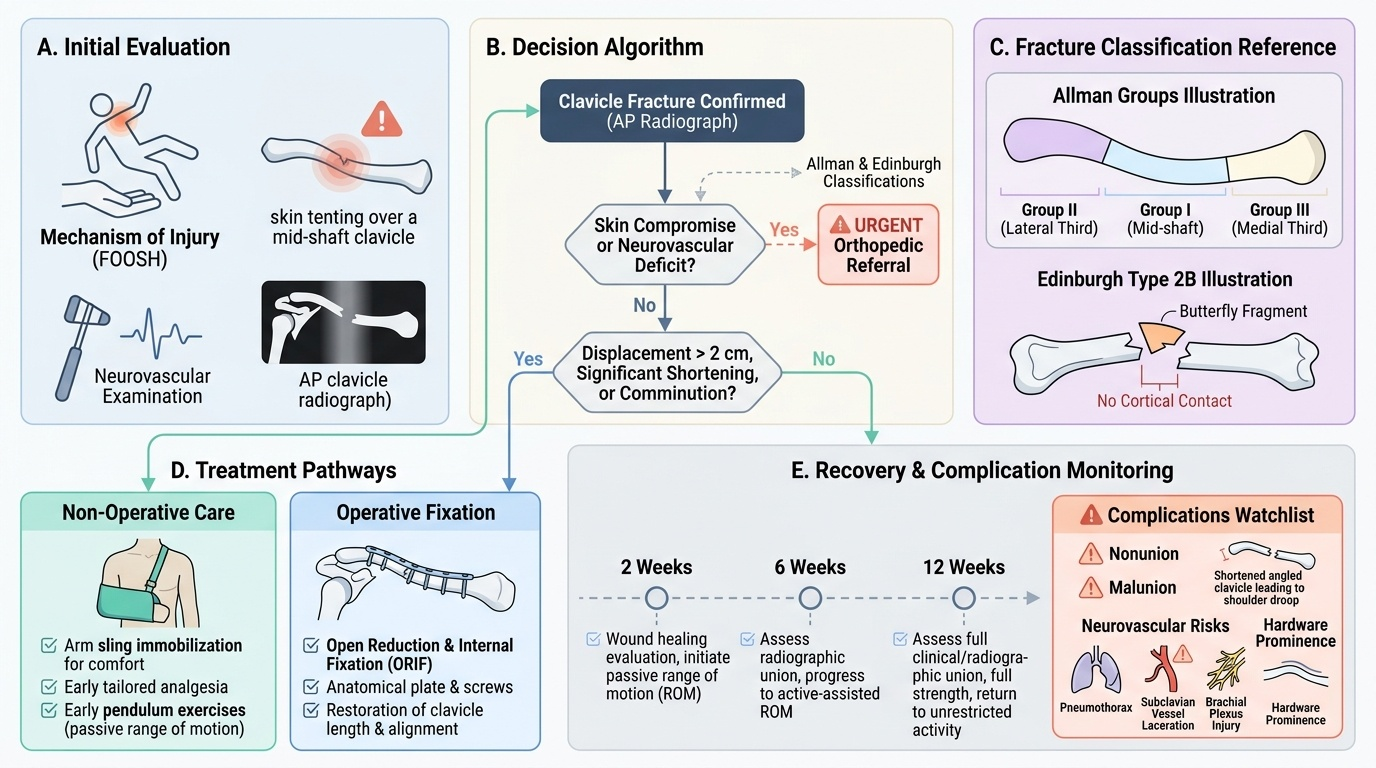
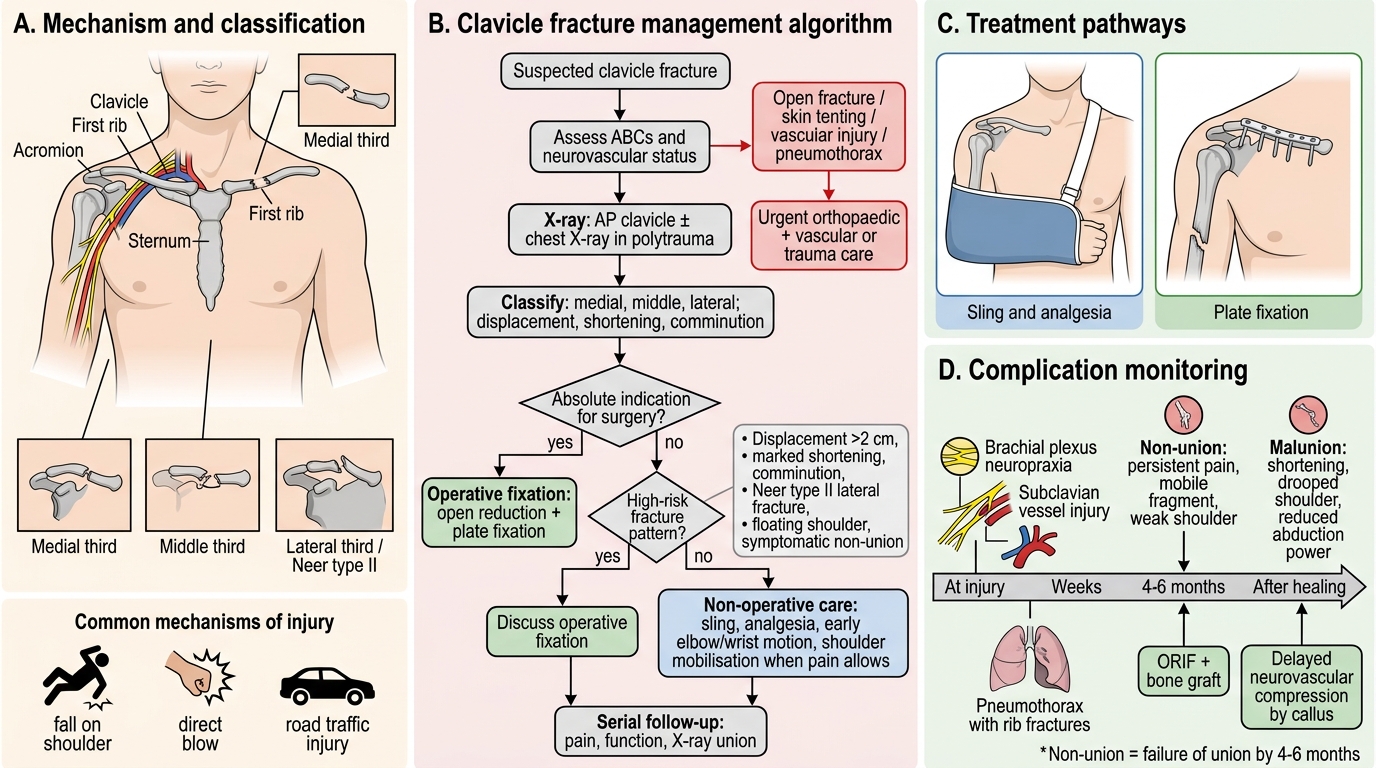
The management of clavicle fractures has evolved considerably since landmark randomised controlled trials -- notably the Canadian Orthopaedic Trauma Society (COTS) trial, 2007 -- demonstrated superior outcomes with plate fixation for displaced mid-shaft fractures. The key decision is whether a fracture can be expected to unite satisfactorily with non-operative care, or whether its pattern carries a high risk of non-union or malunion with functional deficit.
Non-operative management remains appropriate for undisplaced or minimally displaced mid-shaft fractures (shortening <2 cm, cortical contact preserved) and for most Group III fractures without neurovascular compromise. The standard immobilisation is a broad-arm sling for 3-6 weeks; a figure-of-eight bandage does not reduce displacement and causes axillary pressure sores, so it is largely abandoned. Active pendulum exercises begin at 2 weeks; formal physiotherapy follows at union (~6 weeks). Radiographic confirmation of union is expected at 6-8 weeks.
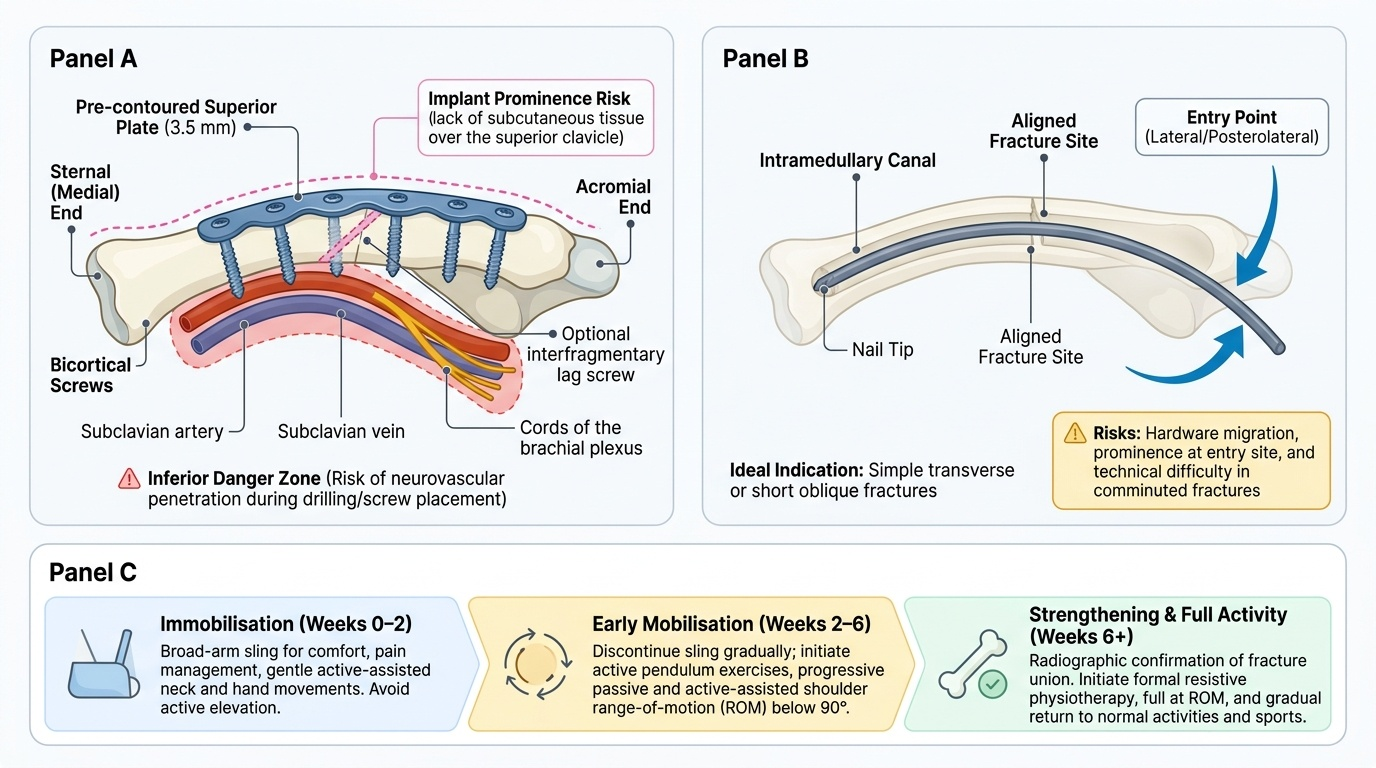
Operative indications for mid-shaft fractures include: shortening >=2 cm, complete displacement (no cortical contact), open fracture, skin tenting, bilateral clavicle fractures, floating shoulder (ipsilateral clavicle + scapula neck fracture), polytrauma, and symptomatic non-union. For Neer type II lateral third fractures, operative fixation (hook plate or coracoclavicular stabilisation) is preferred given the ~30-40% non-union rate. Plate-and-screw fixation using a pre-contoured 3.5 mm reconstruction plate on the superior surface gives robust fixation and allows early mobilisation. Intramedullary nailing is a less invasive alternative but carries higher rates of hardware prominence and nail migration.
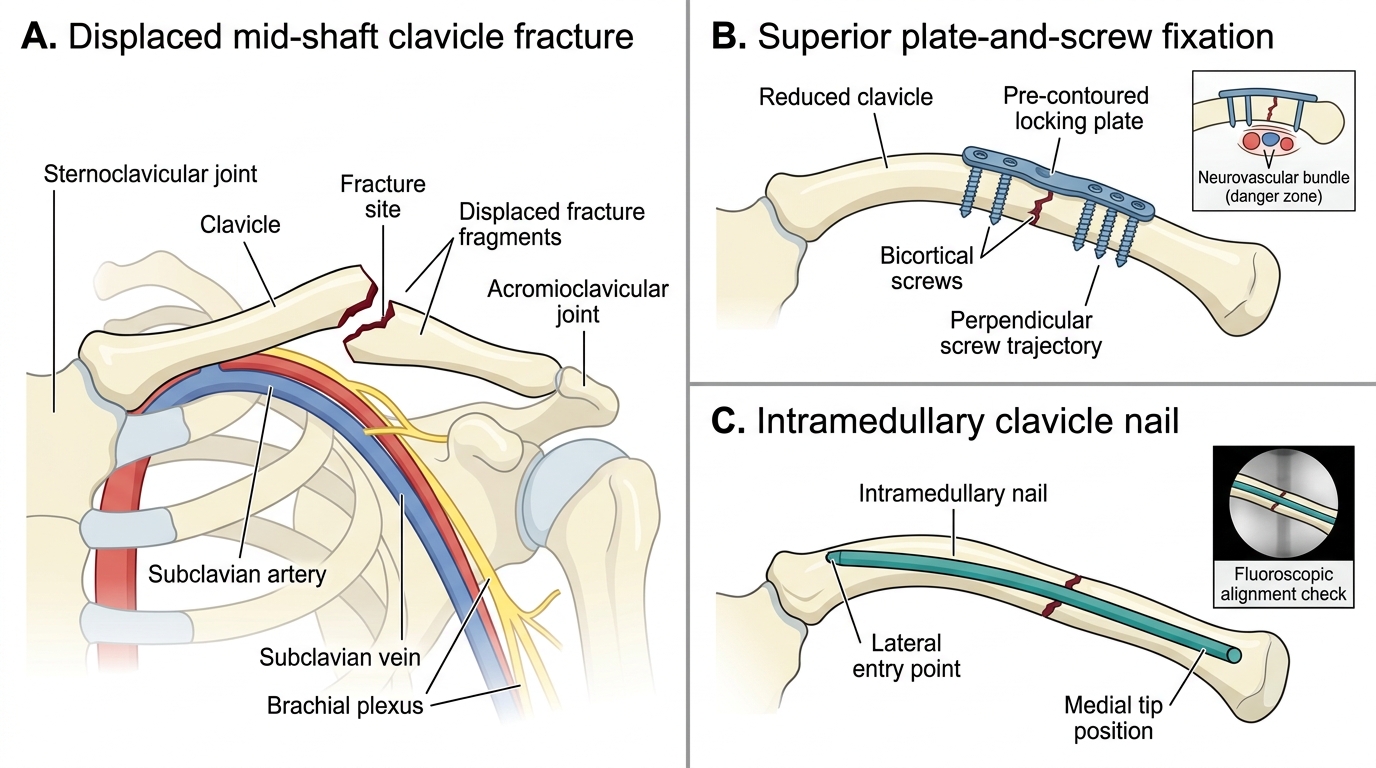
Operative Fixation of Mid-Shaft Clavicle Fracture
Physiotherapy protocol after fixation:
- 0-2 weeks: sling, pendulum only
- 2-6 weeks: progressive active-assisted range of motion
- 6+ weeks: strengthening after radiographic union confirmed
Complications
Provided image
Recognition of complications determines the functional outcome of clavicle fractures. Non-union is the most clinically significant complication, defined as failure of union by 4-6 months. Risk factors include displacement >2 cm, shortening, comminution, Neer type II, and smoking. Symptomatic non-union presents with persistent pain, a palpable mobile fragment, and reduced shoulder strength; treatment is open reduction, plate fixation, and bone grafting. Malunion with significant shortening causes a drooped shoulder and reduced shoulder abduction power; established malunion requires osteotomy and re-plating. At the time of injury, brachial plexus traction injury (usually neuropraxia, expected to recover) and subclavian vessel laceration (vascular emergency) may occur with high-energy fractures. Post-fracture callus can cause delayed neurovascular compression months after healing. Pneumothorax accompanies rib fractures in high-energy mechanisms; chest X-ray in polytrauma is mandatory. Post-operative risks include implant prominence (common with superior plating), hardware failure, infection, and refracture after implant removal.
Clavicle Fracture Management Algorithm
Self-Assessment: Case Review
Apply your knowledge to the following scenario. A 35-year-old construction worker sustains a right clavicle fracture in a fall from scaffolding. Radiograph shows a mid-shaft fracture with complete displacement, 2.8 cm shortening, and a butterfly fragment; the overlying skin is tented but intact. Neurological examination reveals weakness of wrist and finger extension on the right side. He is haemodynamically stable.
Working through this case: the fracture classification is Allman Group I (mid-shaft), Edinburgh type 2B (displaced, comminuted). The shortening of 2.8 cm and complete displacement meet the operative threshold (>=2 cm shortening, no cortical contact). Skin tenting adds urgency. The neurological finding -- weakness of wrist extension -- indicates a radial nerve deficit; however, note that the radial nerve runs in the radial groove of the humerus, not adjacent to the clavicle. Re-examine: at the shoulder, the axillary nerve is the nerve at risk from clavicle/proximal humerus injuries; the brachial plexus trunks traverse the costoclavicular space. A wrist drop in this setting raises the possibility of a concomitant humeral shaft injury or brachial plexus involvement rather than an isolated clavicle injury -- an urgent orthopedic assessment is required.
This case illustrates two key self-assessment points: (1) always re-examine the mechanism and the neurological deficit anatomically -- a 'wrist drop with a clavicle fracture' is anatomically incongruent and mandates a search for a second injury; (2) skin tenting escalates operative urgency regardless of neurovascular status.
Self-check questions:
1. What are the three strongest indications for operative fixation of a mid-shaft clavicle fracture?
2. Which nerve is at risk from a clavicle fracture itself (as opposed to a proximal humerus fracture)?
3. What is the non-union rate for Neer type II lateral third fractures managed conservatively?
4. What implant is specifically designed for Neer type II fixation?
CLINICAL PEARL
The 'shoulder droop test': compare the jugular notch to acromioclavicular joint distance bilaterally -- a >1.5-2 cm shortening versus the contralateral side is a strong indicator of significant displacement that may warrant operative fixation. Critically, a palpable radial pulse does NOT exclude subclavian or axillary artery injury -- assess the complete upper limb neurovascular status and compare with the uninjured side.
SELF-CHECK
Which of the following is the strongest evidence-based indication for operative fixation of a mid-shaft clavicle fracture?
A. Age over 40 years
B. Presence of a butterfly fragment alone
C. Shortening of >=2 cm with complete displacement (no cortical contact)
D. Dominant arm injured
Reveal Answer
Answer: C. Shortening of >=2 cm with complete displacement (no cortical contact)
Shortening >=2 cm with complete displacement is the strongest predictor of non-union and inferior functional outcomes when managed conservatively, as demonstrated by the COTS 2007 RCT. Butterfly fragments and dominant-limb involvement are relative factors; age alone is not an independent operative criterion.