Page 1 of 8
OR6.1 | Degenerative Low Back and Neck Pain — SDL Guide
Learning Objectives
- Enumerate at least eight common causes of low back pain, distinguishing mechanical, degenerative, inflammatory, infective, neoplastic, referred, and metabolic categories
- Describe the pathological basis of cervical spondylosis and differentiate cervical myelopathy from cervical radiculopathy in terms of clinical features and dermatomal patterns
- Explain the pathogenesis and clinical presentation of prolapsed intervertebral disc (PID) including sciatica, dermatomal distribution at L4/L5/S1, and the significance of the straight leg raise (SLR) test
- Identify the red-flag features of cauda equina syndrome and explain why it constitutes a surgical emergency
- Outline the principles of conservative and surgical management for cervical spondylosis, lumbar spondylosis, and prolapsed intervertebral disc
INSTRUCTIONS
Degenerative spine disorders are among the most common musculoskeletal complaints encountered in general medical practice; low back pain alone is the leading global cause of years lived with disability. As a final-year student entering clinical rotations, you will encounter patients with neck and back pain in virtually every clinical setting — the outpatient orthopaedic clinic, the emergency department, and the medical ward. This module integrates your anatomical knowledge of the vertebral column with the pathological processes of disc degeneration and spondylosis to produce a clinically actionable understanding of these conditions. Critically, you will learn to recognise cauda equina syndrome — a time-sensitive emergency whose delayed diagnosis causes irreversible bladder, bowel, and lower-limb deficits. The competency addressed (OR6.1) requires you to both enumerate causes and demonstrate clinical reasoning across the full diagnostic and management spectrum.
References
- Maheshwari J. Essential Orthopaedics, 5th ed. Ch 20 — The Spine (textbook)
- Apley AG, Solomon L. Apley & Solomon's System of Orthopaedics and Trauma, 10th ed. Ch 18 — The Spine (textbook)
- Ebnezar J. Textbook of Orthopaedics, 4th ed. Ch on Degenerative Spinal Disorders (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 48-year-old construction worker presents to the casualty department at 2 AM unable to pass urine for eight hours. He has had chronic low back pain for years, but overnight developed bilateral leg weakness, tingling in both inner thighs and perineum ('as if sitting on a numb cushion'), and is now dribbling incontinence. He is terrified. His SLR is positive bilaterally. The on-call house officer sends him for an MRI lumbosacral spine and phones the orthopaedic registrar. Why the urgency? Because this constellation — saddle anaesthesia, acute urinary retention, bilateral sciatica, and motor weakness — is cauda equina syndrome until proven otherwise, and a delay of even a few hours in surgical decompression converts a recoverable deficit into permanent incontinence and paraplegia. Tonight, the knowledge you build here is the clinical reflex that may save this patient's continence — and his dignity.
WHY THIS MATTERS
Low back pain is the single most prevalent musculoskeletal disorder worldwide, affecting up to 80% of people at some point in their lives and accounting for more disability-adjusted life years than any other condition. Neck pain is similarly ubiquitous, ranking fourth globally. As a clinician you need a structured approach: the ability to enumerate the full differential (so you do not miss a sinister cause), to clinically localise a disc herniation (so you don't over-investigate), and to recognise the handful of red-flag features that mandate emergency imaging and surgery. The degenerative conditions — cervical spondylosis, lumbar spondylosis, and prolapsed intervertebral disc — account for the large majority of presentations, but the skill is in knowing when an apparently routine back-pain patient is actually an emergency. This module gives you both the diagnostic breadth and the emergency discrimination.
RECALL
Before proceeding, orient yourself with these prior-knowledge anchors:
- Vertebral column anatomy: 7 cervical, 12 thoracic, 5 lumbar vertebrae; each intervertebral disc consists of a central nucleus pulposus (gelatinous, 80% water in youth) surrounded by the fibrous annulus fibrosus; posterior to the discs run the spinal cord (to ~L1-L2) and below that the cauda equina (nerve roots L2-S5 + coccygeal root).
- Dermatomes relevant to lumbar disc herniation: L4 — medial calf and foot; L5 — lateral calf and dorsum of foot (big toe); S1 — lateral border of foot and small toe. The L4/L5 disc compresses the L5 root; the L5/S1 disc compresses the S1 root.
- SLR (Lasègue's sign): with the patient supine, passive flexion of the extended leg at the hip stretches the sciatic nerve (L4-S1 roots); if this reproduces radicular leg pain below the knee at <70° of elevation, it is a positive SLR — sensitive but not specific for disc herniation at L4/L5 or L5/S1.
- Cervical nerve roots: C5-T1 emerge via intervertebral foramina; C5-C6 disc disease commonly compresses C6 (deltoid/biceps/thumb) and C6-C7 compresses C7 (triceps/middle finger).
Causes of Low Back Pain — A Structured Enumeration
Low back pain is a symptom, not a diagnosis, and its causes span an enormous range from the utterly benign to the immediately life-threatening. Understanding the full differential is the first step toward asking the right questions and ordering the right investigations. The traditional classification separates causes by tissue of origin and by pathological mechanism, because these two axes together predict the tempo, character, and associated features of the pain. Mechanical (non-specific) low back pain — arising from muscles, ligaments, and facet joints without nerve compression or structural deformity — accounts for approximately 85% of cases; however, the clinician's responsibility is to confidently exclude the remaining 15%, which include surgically correctable nerve compression, inflammatory arthritis, infection, and malignancy before attributing pain to a mechanical cause.
Degenerative / structural causes:
- Lumbar spondylosis — disc space narrowing, osteophyte formation, and facet arthritis secondary to age-related intervertebral disc degeneration
- Prolapsed intervertebral disc (PID) — herniation of nucleus pulposus through the annulus fibrosus, compressing an adjacent nerve root (radiculopathy) or the cauda equina
- Lumbar spinal stenosis — narrowing of the spinal canal or lateral recesses by hypertrophied ligamentum flavum, osteophytes, and facet hypertrophy; classically causes neurogenic claudication
- Spondylolisthesis — anterior slip of one vertebra on the one below, most commonly at L4/L5 or L5/S1
Inflammatory causes:
- Ankylosing spondylitis — HLA-B27-associated seronegative spondyloarthropathy; insidious onset in young men, morning stiffness >1 h, improves with exercise
- Rheumatoid arthritis (primarily cervical spine — atlantoaxial instability; lumbar less common)
- Psoriatic spondylitis, reactive arthritis (other seronegative spondyloarthropathies)
Infective causes:
- Pyogenic vertebral osteomyelitis / discitis — Staphylococcus aureus most common; acute onset, fever, point tenderness, elevated inflammatory markers
- Tuberculous spondylitis (Pott's disease) — indolent onset, predilection for lower thoracic/thoracolumbar junction, cold abscess formation, anterior wedging leading to gibbus (kyphotic deformity); do not confuse the indolent TB tempo with the acute presentation of pyogenic infection
Neoplastic causes:
- Secondary metastatic deposits — the spine is the most common site of skeletal metastasis; breast, prostate, lung, kidney, thyroid ('BPT + LK' mnemonic); age >50, unremitting pain worse at night/supine, known malignancy = red flags
- Multiple myeloma — diffuse osteoporotic vertebral collapse in older patients; serum protein electrophoresis diagnostic clue
- Primary bone tumours (osteosarcoma, chordoma — rare, mostly young patients)
Metabolic / endocrine causes:
- Osteoporotic vertebral compression fractures — common in post-menopausal women; sudden-onset severe back pain after minimal or no trauma; multiple thoracolumbar fractures produce kyphosis
- Osteomalacia, Paget's disease
Referred pain (no spinal pathology):
- Abdominal aortic aneurysm (pulsatile mass, bruit, severe tearing back pain in older men — surgical emergency)
- Retroperitoneal pathology: pancreatitis, renal calculus, ureteric colic, retroperitoneal haemorrhage
- Pelvic pathology: endometriosis, ovarian cysts, pelvic inflammatory disease
Mechanical / musculoligamentous (non-specific, no nerve compression):
- Acute muscular strain, ligament sprain
- Poor posture, occupational overload (heavy lifting, prolonged sitting)
- Facet joint arthropathy
IMMANENT NOTE: Red-flag causes (the 'TUNA' screen) — Tumour, iUnfection, Neurological compromise (cauda equina), Ankylosing spondylitis/inflammatory — demand immediate investigation.
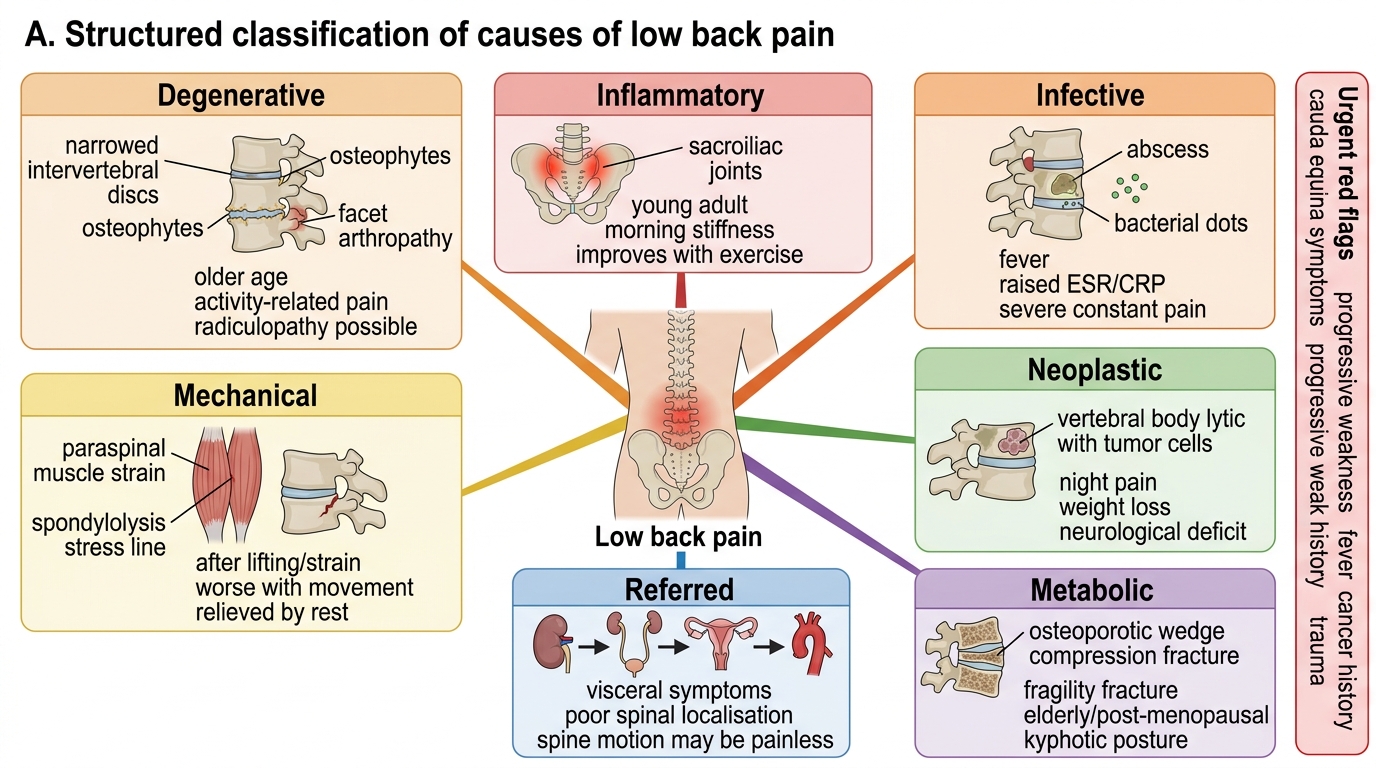
Classification of Causes of Low Back Pain
Clinical Presentations: Cervical Spondylosis, Lumbar Spondylosis, and PID
The clinical syndrome that a patient presents with depends on which structure is compressed (nerve root vs spinal cord vs cauda equina), at which spinal level, and with what severity. A clinician who can accurately match symptoms to anatomy can localise the lesion before the radiologist confirms it — and can prioritise which cases need emergency intervention.
Cervical radiculopathy — nerve root compression in the neck:
Patients characteristically describe a sharp, burning, electric-shock-like pain radiating from the neck down the arm in a dermatomal distribution, often worse with neck extension or lateral flexion toward the symptomatic side (which narrows the foramina). Associated features include paraesthesiae (tingling, numbness in the same dermatomal territory), and motor weakness in the myotome supplied by the compressed root. Common level-specific patterns:
- C5 root (C4-C5 disc): shoulder abduction weakness (deltoid), reduced biceps reflex, lateral shoulder/upper arm sensory loss
- C6 root (C5-C6 disc): biceps/brachioradialis weakness, reduced brachioradialis reflex, thumb and index-finger paraesthesiae
- C7 root (C6-C7 disc): triceps weakness, reduced triceps reflex, middle-finger paraesthesiae
- C8 root (C7-T1 disc): intrinsic hand muscle weakness, little-finger paraesthesiae
Cervical myelopathy — cord compression (a more sinister presentation):
Patients present with bilateral leg spasticity (stiff, clumsy gait, difficulty walking), upper limb clumsiness (difficulty with fine motor tasks — buttoning, writing), and urinary symptoms (urgency, frequency). Examination reveals upper motor neurone signs below the level of compression: increased tone, brisk reflexes, extensor plantar response (Babinski sign), clonus. In the hands, the inverted supinator reflex (tapping the brachioradialis reflex with the wrist in supination elicits finger flexion rather than brachioradialis contraction) is a classical sign of C5-C6 cord compression. Lhermitte's sign — an electric-shock sensation down the spine on neck flexion — also indicates cervical myelopathy. Critically: myelopathy is not painful in the early stages — the patient often presents to a neurologist for gait disturbance before an orthopaedic surgeon for neck pain.
Lumbar spondylosis and neurogenic claudication:
Pain is typically bilateral, starts in the buttocks, and radiates into both thighs and calves on walking or prolonged standing (extension narrows the spinal canal). The key differentiating feature from vascular claudication is the positional nature: bending forward (shopping-trolley sign), sitting, or cycling relieves symptoms (these postures flex the lumbar spine and increase canal diameter). Peripheral pulses are normal. The walking distance is variable and depends on how much the patient leans forward.
PID and sciatica — lumbar radiculopathy:
Sciatica is the term for radicular pain from lumbar nerve root compression — characteristically described as a sharp, burning, or shooting pain that begins in the lower back and radiates through the buttock and down the posterior or postero-lateral aspect of the leg to the foot, below the knee. Because sciatica follows a specific dermatomal pattern, the clinician can often predict the disc level from the distribution:
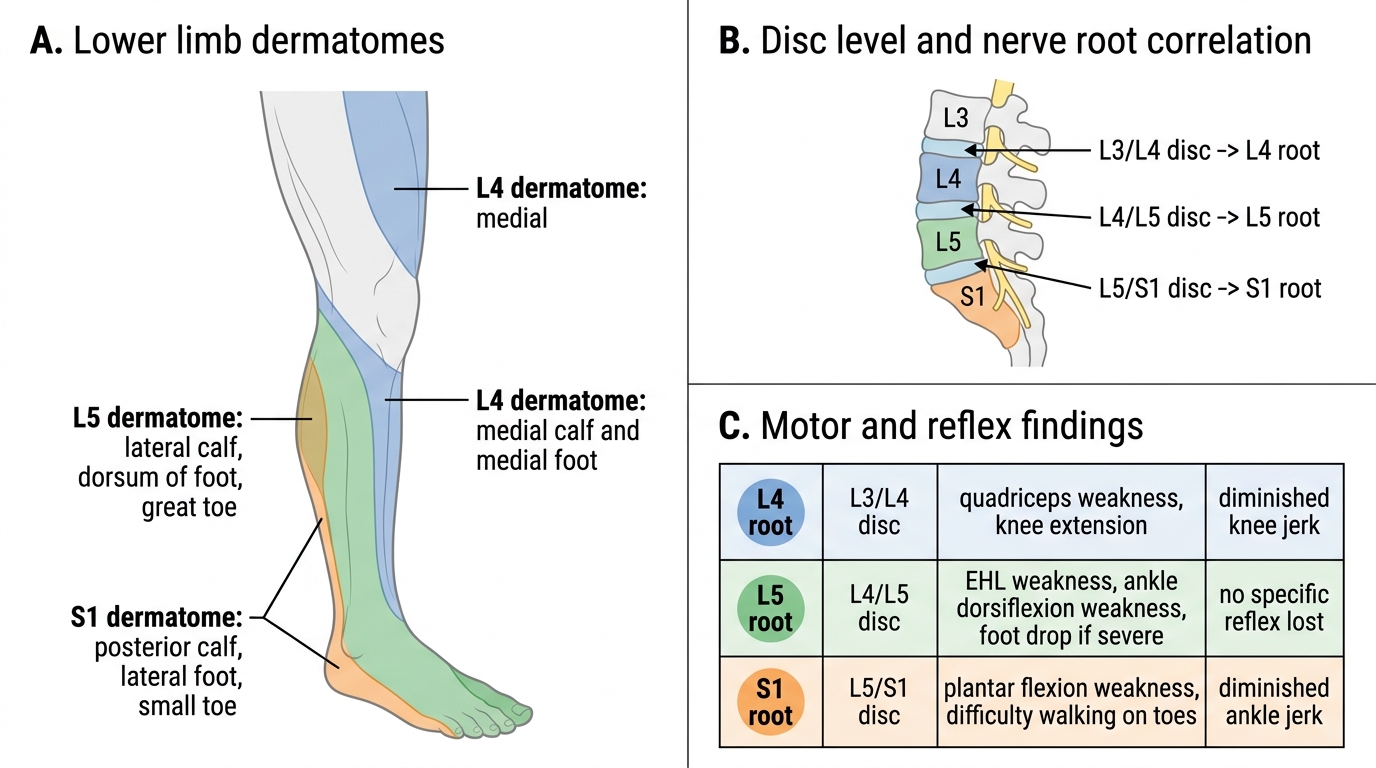
L4, L5, and S1 Lower Limb Dermatomes and Disc Correlation
- L4 root (L3/L4 disc): anterior thigh → medial calf → medial border of foot; weakness of knee extension (quadriceps); diminished knee jerk
- L5 root (L4/L5 disc): lateral calf → dorsum of foot → great toe; weakness of great-toe extension (extensor hallucis longus — EHL), ankle dorsiflexion (foot drop if severe); no specific reflex lost (tibialis posterior reflex occasionally)
- S1 root (L5/S1 disc): posterior thigh → posterior calf → lateral border of foot → small toe; diminished ankle jerk (most reliable reflex loss in lumbar disc disease); weakness of plantar flexion (walking on toes)
The straight leg raise (SLR) test is performed with the patient supine: the examiner slowly raises the extended leg passively; a positive test reproduces the patient's radicular pain (below the knee) at <70° of elevation. Dorsiflexion of the foot at the point of pain (Bragard's sign) increases sciatic nerve tension and intensifies the pain, confirming a true positive. The contralateral (crossed) SLR — pain in the symptomatic leg when the opposite leg is raised — has lower sensitivity but higher specificity for disc herniation.
Cauda equina syndrome — a surgical emergency (RED FLAGS):
Compression of the cauda equina (nerve roots L2-S5 in the lumbar canal, typically at L4/L5 or L5/S1 by a massive central disc herniation) produces a characteristic cluster of findings that constitute an absolute surgical emergency. The five red-flag features are:
1. Saddle anaesthesia — numbness/loss of sensation over the perineum, inner thighs, buttocks, and anus (the area that would contact a saddle): this is the most specific sign of cauda equina involvement
2. Acute urinary retention or overflow incontinence — loss of detrusor control; the patient cannot initiate micturition or dribbles incontinence
3. Loss of bowel control — faecal incontinence or inability to voluntarily contract the anal sphincter
4. Bilateral sciatica or bilateral lower-limb weakness — compression of multiple roots bilaterally
5. Rapidly progressive neurological deficit — worsening over hours
Any single one of these five features in a patient with back pain mandates emergency MRI and urgent neurosurgical/orthopaedic review. Delay beyond 24-48 hours from symptom onset is associated with permanent bladder and bowel dysfunction. This cannot be over-emphasised: a patient with saddle anaesthesia and urinary retention is an orthopaedic emergency even if their leg pain has resolved.
Pathological Basis of Degenerative Spine Disease
Intervertebral disc degeneration is a universal ageing phenomenon, but the rate, severity, and anatomical distribution of degeneration determine whether a person develops clinical spondylosis, a prolapsed disc, or remains asymptomatic. Understanding the pathological cascade is essential because it explains why certain clinical features develop in a predictable sequence, and why the same underlying process manifests differently in the cervical versus lumbar spine.
The primary event in disc degeneration is desiccation of the nucleus pulposus: with ageing, proteoglycan content falls, water-binding capacity drops (from ~80% water in youth to ~70% by the sixth decade), and the disc loses height and compliance. This height loss has two mechanical consequences: first, the annulus fibrosus — now bearing abnormal hoop stresses — develops circumferential and radial tears; second, the facet joints (which are true synovial joints) are subjected to increased load and develop secondary osteoarthritis (facet hypertrophy, osteophyte formation, synovial thickening). The net result at the segment level is a structurally compromised motor unit — reduced disc height, facet arthritis, and often hypertrophy of the ligamentum flavum — that can encroach on the spinal canal, lateral recesses, and intervertebral foramina.
Cervical spondylosis is the term applied when this degenerative cascade produces symptomatic pathology in the cervical spine (C3-C7, most commonly at C5-C6 and C6-C7 levels). Three mechanisms produce clinical symptoms:
1. Foraminal encroachment by uncovertebral (Luschka's joint) osteophytes or posterior disc bulge compresses an exiting nerve root → cervical radiculopathy (dermatomal arm pain ± sensory loss ± weakness)
2. Central canal narrowing by posterior osteophytes and/or hypertrophied ligamentum flavum compresses the cervical cord → cervical myelopathy (the more serious consequence)
3. Neck pain itself from facet arthritis, disc pain, and muscular guarding
Lumbar spondylosis follows the identical pathological sequence in the lumbar spine. The load-bearing lumbar segments (L3-L4, L4-L5, L5-S1) degenerate preferentially. Lumbar radiculopathy from foraminal osteophytes or lateral disc bulge can mimic PID; central canal stenosis produces neurogenic claudication (bilateral buttock-thigh-calf pain on walking, relieved by sitting or forward flexion — the posture that opens the lumbar canal).
Prolapsed intervertebral disc (PID) is a specific event superimposed on the background of disc degeneration: a sudden increase in intradiscal pressure (acute flexion, heavy lift, cough, sneeze) causes the nucleus pulposus to herniate through the weakened annulus fibrosus. Posterolateral herniation — the most common direction, because the posterior longitudinal ligament is thick centrally — compresses the descending nerve root in the lateral recess before it exits via the foramen (e.g. L4/L5 herniation compresses the L5 root; L5/S1 compresses the S1 root). Central herniation can compress the cauda equina.
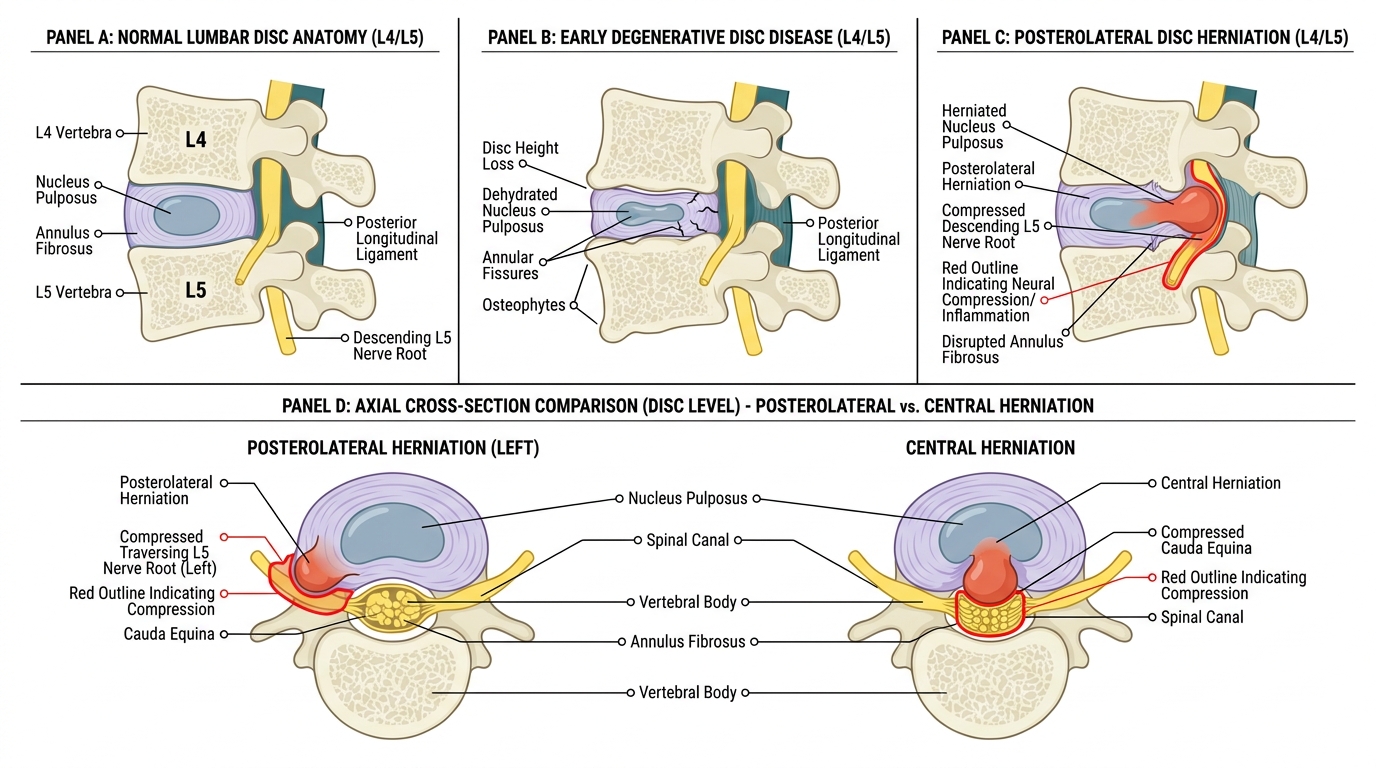
Lumbar Disc Degeneration and Herniation Patterns
SELF-CHECK
A 35-year-old man with acute low back pain reports shooting pain from his right buttock down the lateral aspect of his right calf to the dorsum of his foot and great toe. On examination, he has weakness of right great-toe extension and right ankle dorsiflexion; the ankle jerk is present and normal. SLR is positive on the right at 45°. Which nerve root is most likely compressed, and at which disc level?
A. L4 root; L3/L4 disc
B. L5 root; L4/L5 disc
C. S1 root; L5/S1 disc
D. L4 root; L4/L5 disc
Reveal Answer
Answer: B. L5 root; L4/L5 disc
The dorsum-of-foot and great-toe distribution, combined with weakness of great-toe extension (extensor hallucis longus) and ankle dorsiflexion, is the classical L5 root pattern. The L5 root exits below the L5 vertebra after crossing the L4/L5 disc, which is the level that herniated disc material compresses it posterolaterally. The intact ankle jerk is consistent with L5 involvement (the ankle jerk is mainly S1). An L4 root lesion at L3/L4 would affect the medial calf and diminish the knee jerk; S1 at L5/S1 would affect the posterior calf/lateral foot and diminish the ankle jerk.