Page 2 of 8
OR6.1 | Degenerative Low Back and Neck Pain — SDL Guide (Part 2)
Physical Examination and Investigations
A systematic physical examination approach, followed by targeted imaging, allows accurate localisation of compressive spinal pathology and guides management decisions including the urgency of intervention. The examination of a patient presenting with neck or back pain should integrate inspection, palpation, range of motion, neurological assessment, and specific provocative tests. The history and examination findings should always be synthesised first to generate a working anatomical diagnosis, because imaging frequently reveals degenerative changes in asymptomatic individuals — particularly in adults over 40 years — and over-reliance on imaging without clinical correlation leads to misattribution and inappropriate surgery.
Examination for cervical spondylosis:
Inspection and palpation: Midline tenderness, cervical muscle spasm, restricted and painful cervical movement (especially extension and lateral rotation). Spurling's test (axial compression with lateral flexion toward the symptomatic side) exacerbates foraminal nerve-root pain — a positive test is specific for cervical radiculopathy.
Neurological examination: In cervical radiculopathy — segmental motor weakness, dermatomal sensory loss, and depressed reflexes in the affected root. In cervical myelopathy — upper motor neurone signs below the lesion (hypertonia, brisk reflexes, extensor plantar response, clonus), Romberg's sign, positive Lhermitte's, Hoffmann's sign (flicking the middle finger nail → reflex flexion of the thumb and index finger = UMN sign in the upper limb).
Examination for lumbar disc disease:
Gait and posture: Antalgic gait (leaning away from the side of disc herniation), lumbar list, loss of lumbar lordosis, restricted spinal flexion.
SLR and its variants: Described under clinical presentation above. Note the femoral stretch test (patient prone, knee flexed — exacerbates L3/L4 root pain in the anterior thigh) for upper lumbar disc lesions.
Neurological assessment: Power (MRC scale), sensation, and reflexes in the L4, L5, and S1 myotomes and dermatomes. The ankle jerk (S1) and knee jerk (L4) should always be compared bilaterally.
Investigations:
Plain radiographs (X-ray): Disc space narrowing, osteophyte formation (lipping), sclerosis of end-plates, and subluxation are visible on AP and lateral views. X-rays are useful for screening spondylolisthesis and for identifying vertebral collapse (osteoporosis/tumour). They do NOT show soft-tissue disc herniation or cord/root compression.
MRI (magnetic resonance imaging): The investigation of choice for all soft-tissue spinal pathology. It directly images the intervertebral discs (T2 bright signal = water content — loss = degeneration), the neural canal, nerve roots, cord, and surrounding soft tissues without ionising radiation. MRI is mandatory for cauda equina syndrome (emergency), progressive neurological deficit, and failed conservative management. Sagittal T2-weighted images show disc herniation, cord signal change (myelomalacia in severe myelopathy), and root compression.
CT myelography: When MRI is contraindicated (pacemaker, severe claustrophobia), CT with intrathecal contrast provides excellent canal imaging. CT alone is useful for ossification of the posterior longitudinal ligament (OPLL) in the cervical spine.
Nerve conduction studies (NCS) and EMG: Useful to confirm radiculopathy, distinguish it from peripheral neuropathy, and identify the level and severity of root dysfunction. Most useful when clinical and imaging findings are discordant.
Inflammatory markers (ESR, CRP, Rheumatoid factor, HLA-B27): If inflammatory cause (ankylosing spondylitis, infective discitis) is suspected.
Bone scan / PET-CT: For suspected metastatic disease or multi-level Paget's disease.
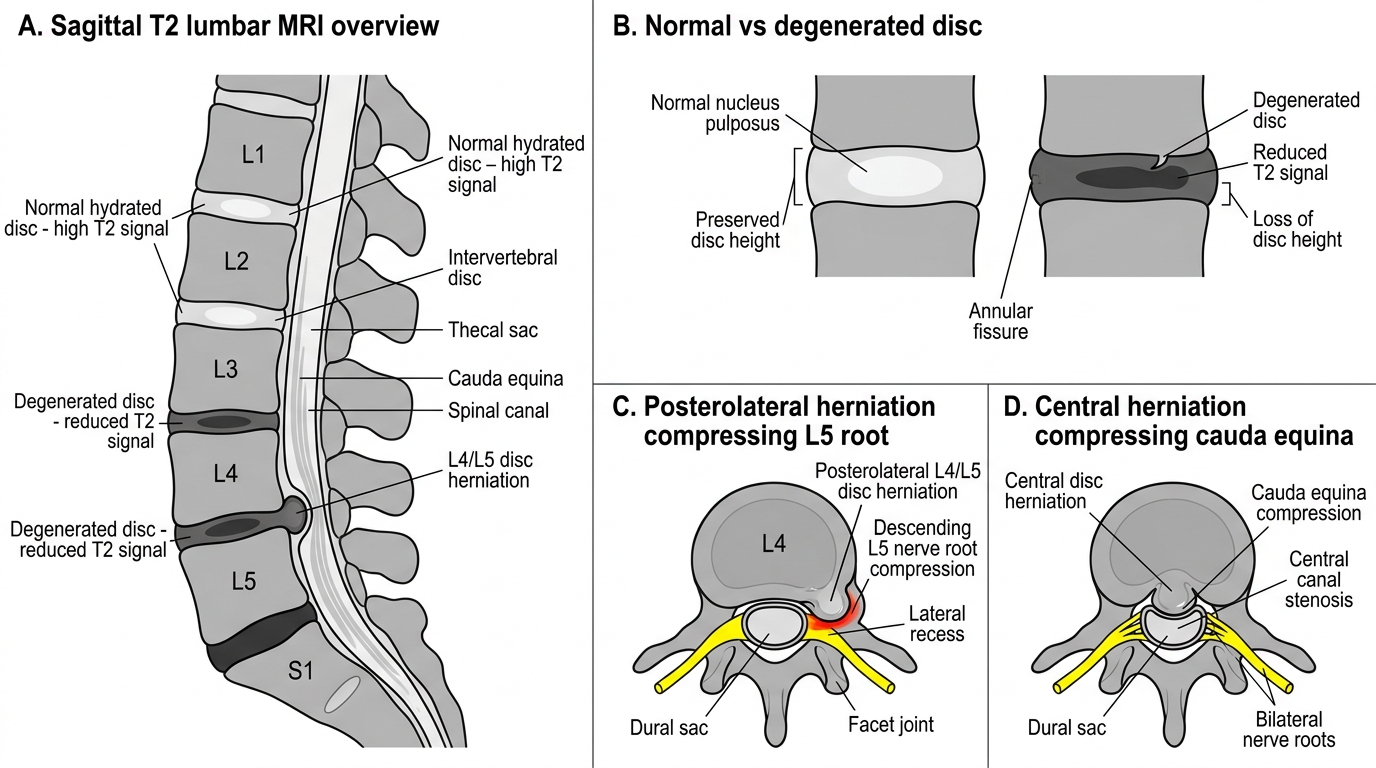
MRI Features of Lumbar Disc Degeneration and Herniation
SELF-CHECK
A 55-year-old woman presents with bilateral leg stiffness, unsteady gait, and difficulty buttoning her shirt for three months. She denies significant neck pain. On examination: bilateral brisk knee and ankle jerks, bilateral extensor plantar responses, and a positive Hoffmann's sign in both hands. What is the most likely diagnosis, and what is the investigation of choice?
A. Lumbar spinal stenosis; X-ray lumbar spine
B. Cervical myelopathy; MRI cervical spine
C. Bilateral cervical radiculopathy; nerve conduction study
D. Ankylosing spondylitis; HLA-B27 testing
Reveal Answer
Answer: B. Cervical myelopathy; MRI cervical spine
The clinical picture — bilateral upper motor neurone signs (brisk reflexes, extensor plantars, Hoffmann's sign), bilateral leg spasticity, and upper-limb fine motor difficulty — localises the lesion to the cervical cord (upper motor neurone lesion above L1). The absence of significant neck pain is characteristic of cervical myelopathy, which often presents insidiously with gait and dexterity symptoms before pain. MRI cervical spine is the investigation of choice: it reveals cord compression, canal stenosis, and cord signal change (myelomalacia on T2). Lumbar stenosis causes neurogenic claudication (lower limb pain on walking, relieved by sitting), NOT upper motor neurone signs. NCS would not diagnose cord compression.
Management: Conservative and Surgical Principles
The management of degenerative spine disorders follows a stepwise principle: the large majority of patients with cervical radiculopathy, lumbar radiculopathy, and acute PID improve with conservative (non-operative) management over weeks to months, because the herniated nuclear material is subject to resorption and the inflammatory radiculopathy resolves spontaneously. Surgery is reserved for those who fail adequate conservative management or — critically — for those who present with features mandating emergency surgery. The decision to operate should always weigh the natural history of the condition, the severity and duration of symptoms, the neurological status, and the surgical risk. Understanding this spectrum — from simple analgesia to emergency decompression — is a core clinical competency for every final-year student.
Conservative management (applicable to cervical spondylosis, lumbar spondylosis, and non-emergency PID):
Analgesia and anti-inflammatory drugs:
- NSAIDs (naproxen, diclofenac) are the cornerstone of acute pain management, reducing both nociceptive and inflammatory components
- Paracetamol for mild-moderate pain; weak opioids (tramadol, codeine) for breakthrough pain — used sparingly and short-term
- Neuropathic adjuvants (gabapentin, pregabalin, amitriptyline) are added when radicular neuropathic pain is prominent and NSAIDs alone are insufficient
- Oral corticosteroids (short tapering course of prednisolone) can be useful in acute, severe radiculopathy to reduce peridiscal inflammation
Physiotherapy and activity modification:
- Active physiotherapy — core-strengthening exercises, lumbar stabilisation, and cervical isometric exercises reduce recurrence rates; bed rest is NOT recommended (it prolongs recovery)
- Cervical soft collar may be used short-term for comfort in acute cervical radiculopathy, but prolonged collar use leads to deconditioning of neck musculature
- Lumbar support / posture correction — ergonomic advice, avoidance of provocative postures (prolonged flexion, heavy lifting)
- Traction — controversial; cervical traction may provide short-term relief for radiculopathy; lumbar traction has limited evidence
Epidural steroid injections:
- Transforaminal or interlaminar epidural injections of corticosteroid (methylprednisolone or triamcinolone) provide targeted anti-inflammatory effect around the compressed root; useful as a bridge while awaiting natural recovery, or to allow physiotherapy; effect is temporary (weeks to months) and does not alter long-term outcomes
- Facet joint injections for facet arthropathy in lumbar spondylosis
Indications for surgical referral — elective:
- Failure of 6-12 weeks of adequate conservative management with persistent, disabling radicular pain
- Progressive neurological deficit (worsening motor weakness) despite conservative treatment
- Cervical myelopathy (any grade) — myelopathy does NOT improve spontaneously; surgical decompression halts progression and may allow partial recovery of function
Surgical management:
Cervical spine:
- Anterior cervical discectomy and fusion (ACDF) — the most common procedure for cervical radiculopathy and myelopathy; the disc and compressing osteophytes are removed through an anterior approach, and the segment is fused (with bone graft ± plate)
- Cervical laminoplasty or laminectomy — posterior decompression for multi-level myelopathy or when OPLL makes anterior surgery hazardous; laminoplasty preserves motion (hinge technique)
- Cervical disc arthroplasty (total disc replacement) — motion-preserving alternative to ACDF at single or double levels in younger patients
Lumbar spine:
- Microdiscectomy / discectomy — the definitive surgical treatment for lumbar PID with radiculopathy failing conservative management; a small posterior or posterolateral approach removes the herniated disc fragment, decompressing the nerve root; 85-90% success rate for sciatica relief
- Laminectomy / decompressive surgery — for lumbar spinal stenosis; removes the hypertrophied ligamentum flavum and osteophytes compressing the canal; relieves neurogenic claudication
- Spinal fusion (posterolateral or PLIF/TLIF) — added to decompression when significant instability or spondylolisthesis is present; instrumented with pedicle screws and rods
Cauda equina syndrome — emergency surgery:
Surgical decompression (emergency MRI → emergency posterior decompression laminectomy and discectomy, typically within 24-48 hours of onset of bladder/bowel dysfunction) is the treatment. The urgency is graded by the presence of complete versus incomplete cauda equina syndrome:
- Incomplete CES (sensory/motor deficit present but bladder/bowel not completely lost): decompression within 24-48 hours offers the best chance of recovery
- Complete CES (complete urinary retention, complete saddle anaesthesia): emergency decompression as soon as possible; however, outcome for bladder recovery is guarded even with prompt surgery
The most important lesson: never delay MRI, never wait for the morning list when cauda equina syndrome is clinically suspected.
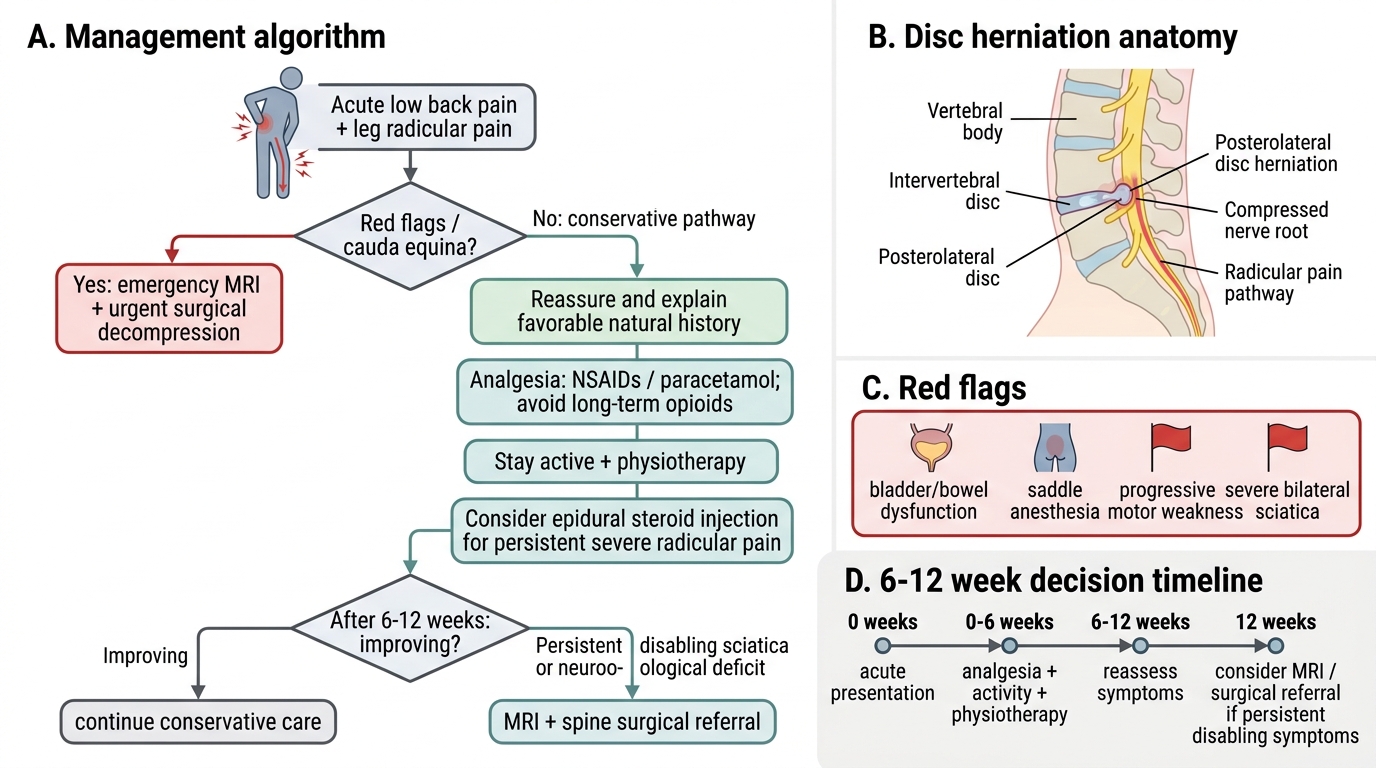
Lumbar Disc Herniation With Radiculopathy: Management Algorithm
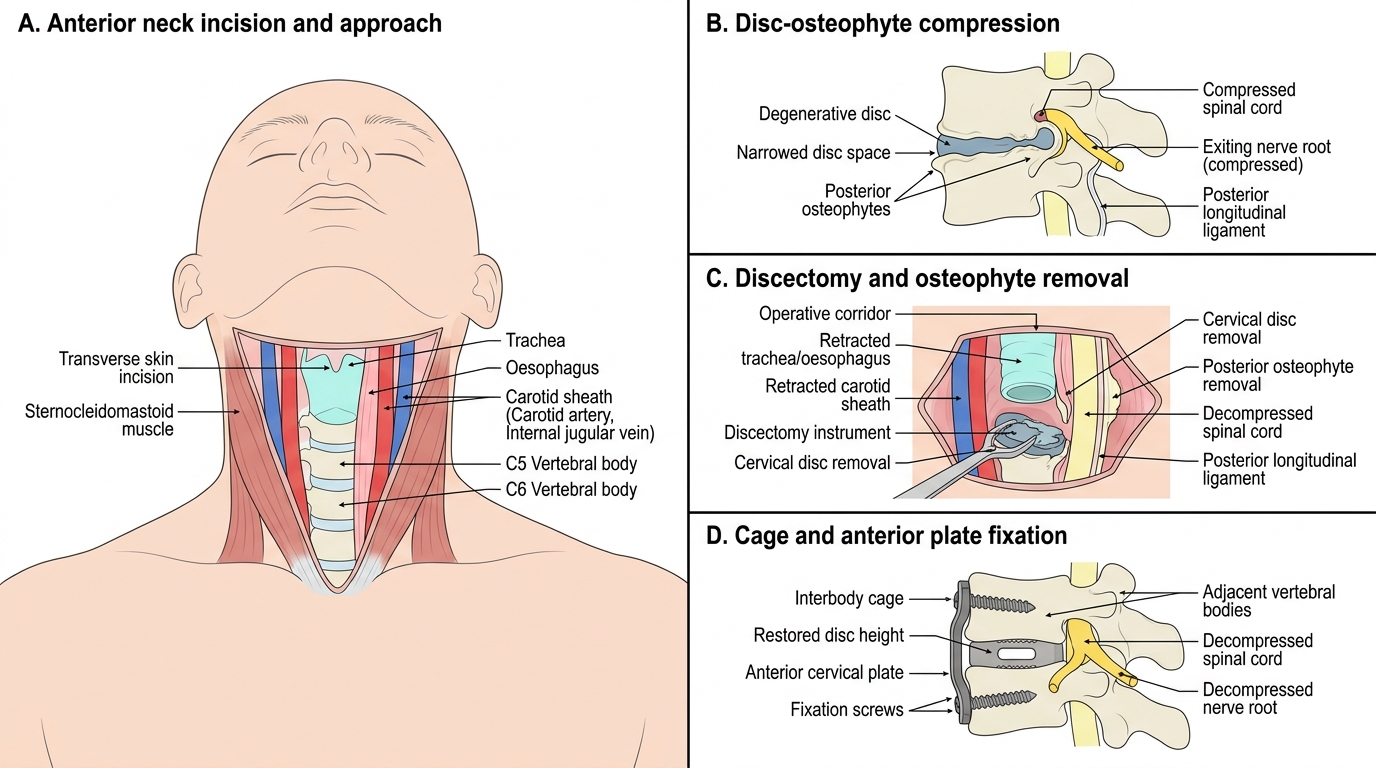
Anterior Cervical Discectomy and Fusion Approach
SELF-CHECK
A 32-year-old woman develops acute low back pain with right-sided sciatica after lifting a heavy object. She is given NSAIDs and physiotherapy. After 8 weeks she reports 50% improvement in her leg pain but still has moderate sciatica. She has no motor deficit, a normal bladder, and SLR positive at 60° on the right. What is the most appropriate next step?
A. Immediate discectomy — she has had 8 weeks of sciatica
B. Continue conservative management with physiotherapy and reassure for up to 12 weeks total
C. Emergency MRI and neurosurgical referral today
D. Prescribe long-term opioid analgesia and stop physiotherapy
Reveal Answer
Answer: B. Continue conservative management with physiotherapy and reassure for up to 12 weeks total
The natural history of lumbar disc herniation with radiculopathy is favourable: the majority of patients experience significant improvement within 6-12 weeks of conservative management. This patient is improving (50% better at 8 weeks), has NO neurological deficit, and has a normally functioning bladder — there is no emergency indication. The appropriate next step is to continue conservative management with physiotherapy, optimise neuropathic pain adjuvants if needed, and consider epidural steroid injection. Surgical referral (elective) would be appropriate if she fails to improve adequately by 12 weeks, or sooner if motor deficit develops or bladder dysfunction occurs. Emergency surgery is only for cauda equina syndrome — not present here.
Self-Assessment: Integrating the Knowledge
This section presents two consolidated clinical scenarios designed to test your integration of the OR6.1 competency across the full clinical reasoning arc — from cause enumeration to examination, imaging, and management decisions. Work through them before reading the explanatory notes.
Scenario A — The Emergency:
A 45-year-old male lorry driver presents at 11 PM with a 24-hour history of acute severe low back pain radiating bilaterally down both legs. He had developed difficulty initiating urination 6 hours ago and now admits to constant dribbling of urine. He reports numbness in the perineum and inner thighs, which he describes as "as though I have been sitting on ice". Examination reveals bilateral extensor hallucis longus weakness (3/5 bilaterally), absent ankle jerks bilaterally, reduced perianal sensation, and lax anal sphincter tone on digital rectal examination. SLR is positive bilaterally at 40°.
What is the diagnosis? What is the single most important next investigation and why? What is the management and its timing?
This presentation is classic cauda equina syndrome from a large central disc herniation, most likely at L4/L5 or L5/S1. The diagnostic triad is: saddle-area anaesthesia (inner thighs, perineum) + bladder/bowel dysfunction + bilateral motor/sensory deficit in the lower limbs. The single most important investigation is emergency MRI lumbosacral spine — it directly images the disc herniation, the degree of cauda equina compression, and rules out other causes (tumour, abscess). Management: emergency surgical decompression — urgent posterior laminectomy and discectomy within 24-48 hours of symptom onset. Any delay in bladder/bowel dysfunction beyond 24-48 hours is associated with permanent dysfunction even with surgery. The house officer must alert the orthopaedic/neurosurgical registrar immediately — this is not a case for the morning elective list.
Scenario B — The Chronic Presentation:
A 58-year-old woman presents with a 2-year history of bilateral leg pain that comes on after walking 300 metres and is relieved by sitting down and leaning forward. She has no rest pain and no bladder symptoms. Examination in the clinic reveals normal power, sensation, and reflexes bilaterally; she has a mildly reduced lumbar range of motion. Peripheral pulses are present and equal bilaterally.
What is the most likely diagnosis? How does it differ from vascular claudication? What investigations and management would you offer?
This is neurogenic claudication secondary to lumbar spinal stenosis. The key differentiating feature from vascular claudication is positional relief — the shopping-trolley sign (leaning forward) relieves neurogenic claudication by flexing the spine and increasing the canal diameter, whereas vascular claudication is relieved by simply stopping walking (regardless of position). Peripheral pulses are normal (ruling out arterial insufficiency). Investigations: MRI lumbosacral spine will confirm canal stenosis. Management: conservative initially (physiotherapy, NSAIDs, walking aids with forward flexion); if disabling, epidural steroid injection provides temporary relief; definitive treatment is decompressive laminectomy of the affected levels.
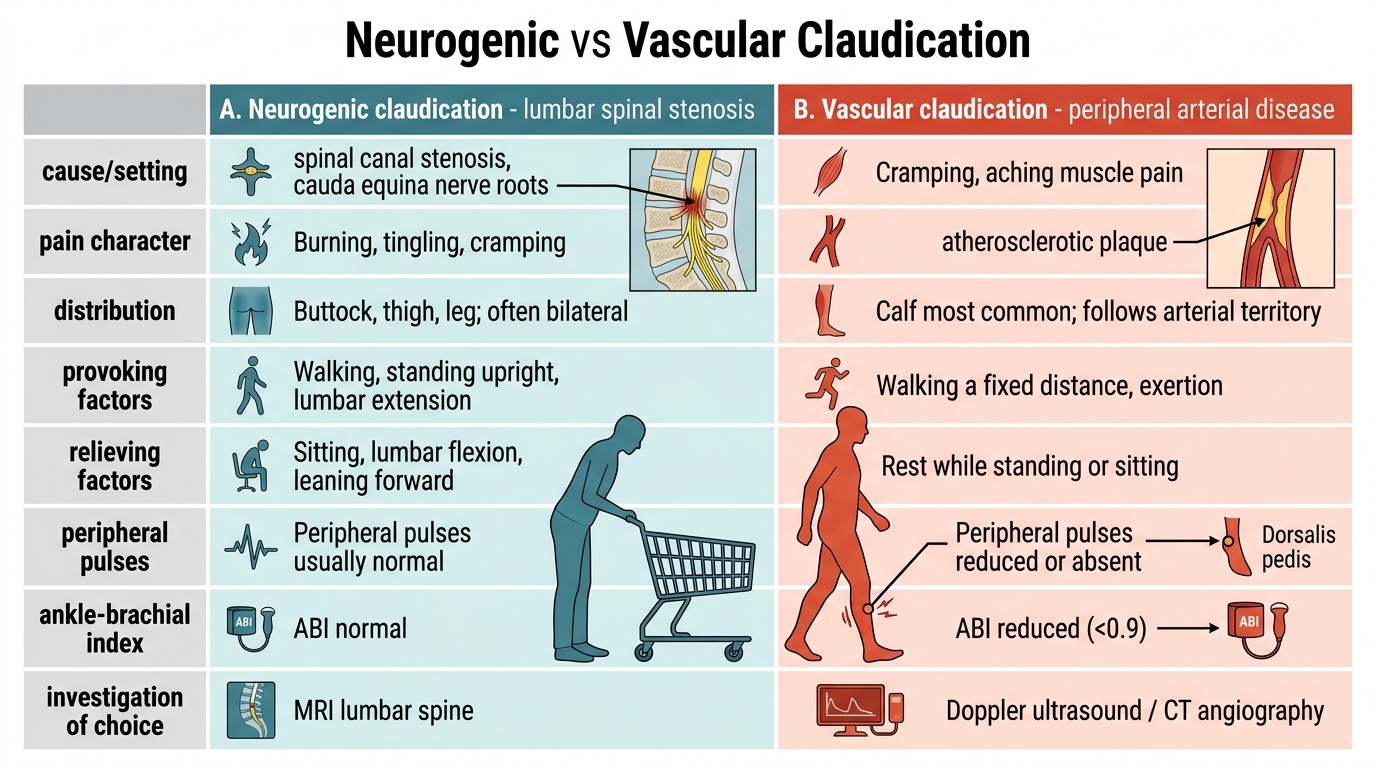
Neurogenic vs Vascular Claudication
CLINICAL PEARL
Three clinical pearls that save patients:
- The saddle test saves bladders. In any patient with acute low back pain and new urinary symptoms, always examine perineal sensation. Saddle anaesthesia + urinary dysfunction = cauda equina syndrome = emergency MRI now. This test takes 30 seconds and its omission constitutes medicolegal negligence.
- Myelopathy does not hurt — until it is serious. Cervical myelopathy characteristically presents with leg stiffness and hand clumsiness rather than neck pain. Any patient >50 years with bilateral leg stiffness, gait instability, or deteriorating handwriting needs a neurological examination and cervical MRI — do not attribute these to "old age" without ruling out surgically correctable cord compression.
- Imaging age, not pain. MRI of the lumbar spine in asymptomatic adults over 40 years commonly shows disc bulges, osteophytes, and signal changes that are entirely coincidental findings. Always correlate imaging with the specific clinical level indicated by the dermatomal/myotomal deficit and the provocative tests. Treating the MRI rather than the patient leads to unnecessary surgery and poor outcomes.