Page 10 of 44
EN2.{3,5} | Otoscopy Tuning Fork Testing and Tympanic Membrane Assessment — SDL Guide (Part 2)
Tuning Fork Test Technique: Rinne, Weber, and ABC
The three tuning fork tests each test a different aspect of the auditory pathway, and together they form a bedside diagnostic battery that is remarkably powerful when performed correctly. The Rinne test interrogates the same ear's AC vs BC relationship, the Weber test uses the skull as a conductor to compare both cochleae simultaneously, and the ABC test benchmarks the patient's cochlear endurance against a known-normal examiner. Performing all three in sequence gives a complete bedside characterisation of the hearing loss type. The sequence matters: do Rinne first (it is the most specific for the type of loss), then Weber (which adds lateralisation information), then ABC (which confirms cochlear status). Each must be performed with precise technique to give valid results — an improperly performed Rinne (fork held too far from the meatus, or BC tested with the tines rather than the base) will give an invalid result regardless of how carefully it is interpreted.
RINNE TEST — comparing AC to BC in the SAME ear, one ear at a time:
The Rinne test compares air conduction (the normal route through outer and middle ear to cochlea) with bone conduction (direct vibration through the skull to the cochlea) in the ear being tested.
Technique:
1. Strike the 512 Hz tuning fork on the examiner's elbow (moderate force).
2. Place the vibrating fork base firmly on the mastoid process behind the ear being tested. Ask: 'Do you hear this?' Wait until the patient indicates they can no longer hear it, then immediately...
3. Move the fork (still vibrating) to 2–3 cm in front of the external meatus, tines facing the ear. Ask: 'Can you hear this now?' (or: 'Which is louder — the bone position or the air position?')
Interpretation:
- Rinne POSITIVE: AC heard after BC stops (or AC louder than BC). This means AC > BC. This is the NORMAL result — it is also the result in sensorineural hearing loss (SNHL), where both AC and BC are reduced, but AC remains greater than BC because the ossicular amplification mechanism is intact.
- Rinne NEGATIVE: BC heard after AC stops (or BC louder than AC). This means BC > AC. This is the result in CONDUCTIVE hearing loss — the outer or middle ear is blocking the AC route, so the direct BC route becomes relatively better.
- A simple way to remember: Positive Rinne = AC beats BC = Normal or SNHL. Negative Rinne = BC beats AC = Conductive loss.
WEBER TEST — assessing lateralisation of BC to identify which ear is affected:
The Weber test uses bone conduction alone and tests BOTH ears simultaneously by placing the fork on the midline skull.
Technique:
1. Strike the 512 Hz fork and place the base firmly on the midline of the skull (vertex, forehead, or lower midline of forehead/chin). Ensure firm bony contact.
2. Ask: 'Where do you hear the sound — in the middle, or more to one side?'
Interpretation:
- Weber central (not lateralised): Normal hearing bilaterally, or symmetrical hearing loss bilaterally.
- Weber lateralises TO the affected (worse) ear: CONDUCTIVE hearing loss in that ear. Reason: middle ear disease blocks external sounds from reaching the cochlea of the affected ear, but bone conduction remains intact. The cochlea of the affected ear is relatively quiet (no background environmental noise reaching it) compared to the normal ear, so the BC signal from the tuning fork appears louder in the affected ear — it is heard against a quieter background. This is the occlusion effect.
- Weber lateralises AWAY from the affected ear (to the better ear): SENSORINEURAL hearing loss in the worse ear. The cochlea of the affected ear is damaged and cannot respond well even to direct BC stimulation — the signal is heard better in the normal cochlea.
- Memorise: Conductive loss → Weber to the bad ear. SNHL → Weber to the good (better) ear.
ABC TEST (Absolute Bone Conduction / Schwabach's Test) — comparing patient's BC to examiner's BC:
The ABC test compares the patient's bone conduction to that of a known-normal examiner, giving an absolute assessment of cochlear function.
Technique:
1. Strike the fork and place the base on the patient's mastoid. When the patient can no longer hear it, immediately transfer the fork to the examiner's own mastoid.
2. If the examiner can still hear it, the patient's BC is reduced below normal.
Interpretation:
- ABC normal (equal to examiner): Cochlear function intact. Normal or conductive hearing loss.
- ABC reduced (patient cannot hear as long as the examiner): Cochlear or eighth nerve pathology — SENSORINEURAL hearing loss.
SELF-CHECK
A 40-year-old male with right ear discharge and right-sided hearing loss undergoes tuning fork tests. Rinne right ear: NEGATIVE (BC > AC). Weber: lateralises to the RIGHT ear. ABC: normal (equal to examiner). The most likely diagnosis is:
A. Right sensorineural hearing loss (cochlear pathology)
B. Right conductive hearing loss (middle ear pathology)
C. Bilateral sensorineural hearing loss
D. Left conductive hearing loss
Reveal Answer
Answer: B. Right conductive hearing loss (middle ear pathology)
The pattern — Rinne NEGATIVE right ear (BC > AC = conductive loss) + Weber lateralising TO the right (affected) ear (conductive loss lateralises to the bad ear) + ABC normal (cochlea intact) — is the classic pattern of RIGHT CONDUCTIVE hearing loss. Given the history of right ear discharge, this is consistent with CSOM causing conductive hearing loss. SNHL would give Rinne POSITIVE (AC > BC still), Weber lateralising AWAY from the affected ear, and REDUCED ABC. The distinction between these two patterns is the core clinical skill tested.
Interpreting Tuning Fork Tests: The Key Rules
The tuning fork test interpretation rules must be learnt as a set, not in isolation, because the value of the tests is in their combined pattern. No single test result is diagnostic alone — the three tests together characterise the hearing loss type with high reliability when performed correctly. It is also worth stating explicitly why these rules follow logically from the anatomy and physiology covered in the recall block: conductive loss spares the cochlea, so BC (which bypasses the blocked outer/middle ear and reaches the cochlea directly) is relatively enhanced — hence Rinne NEGATIVE and Weber to the affected ear. SNHL damages the cochlea itself, so BC is also impaired on the affected side — hence Rinne remains POSITIVE (ossicular mechanism intact, AC still > BC) but Weber goes to the better cochlea and ABC is reduced. Working from mechanism rather than rote memorisation means you will reconstruct the rules even if you briefly forget them under examination pressure. The summary table and the false-negative Rinne exception below are the most examination-critical elements of this entire SDL.
Provided image
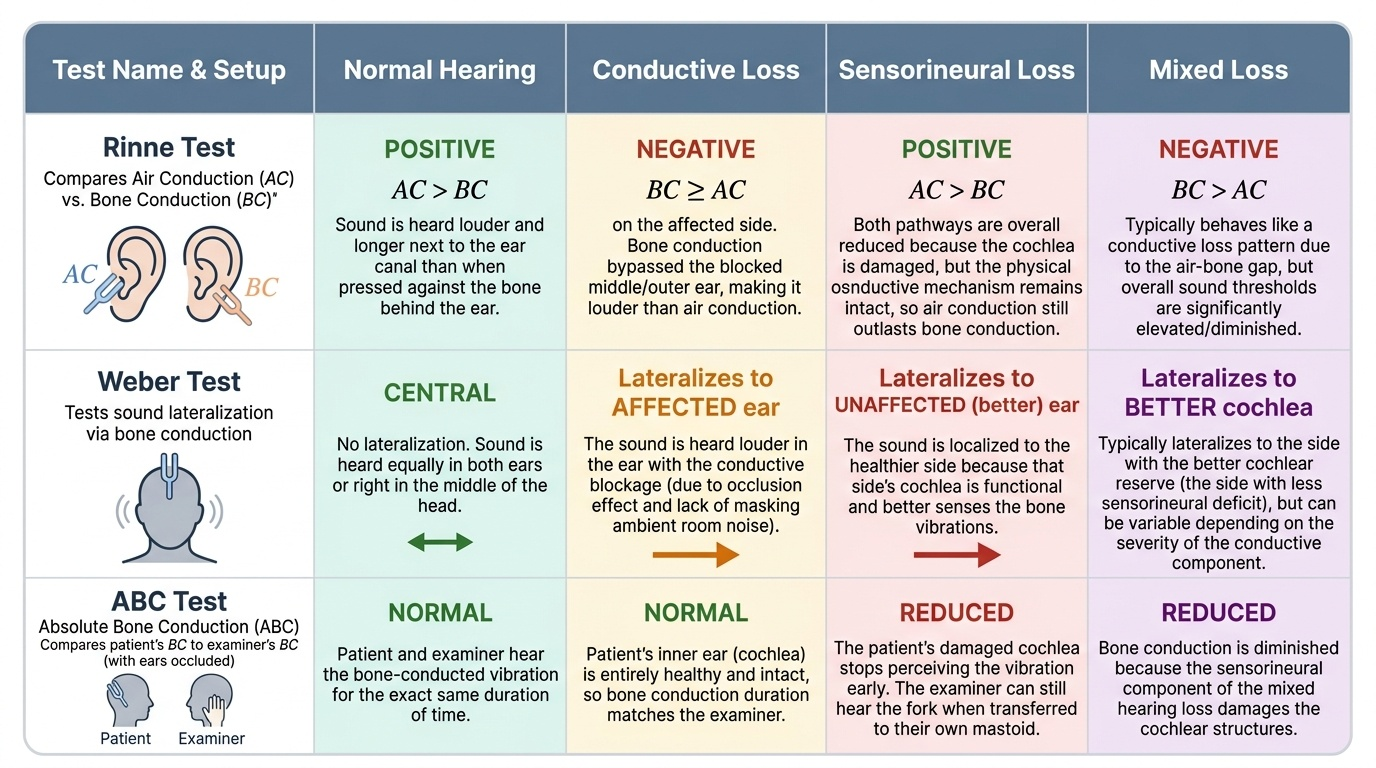
The three combined patterns and their interpretation:
Pattern 1 — Normal hearing:
- Rinne: POSITIVE bilaterally (AC > BC in both ears)
- Weber: CENTRAL (no lateralisation)
- ABC: Normal (equal to examiner)
Pattern 2 — Unilateral conductive hearing loss (e.g. right CSOM, right wax, right otitis media with effusion):
- Rinne: NEGATIVE on the affected (right) ear (BC > AC); POSITIVE on the normal (left) ear
- Weber: Lateralises TO the affected (right) ear
- ABC: Normal (cochlea is intact on both sides)
Pattern 3 — Unilateral sensorineural hearing loss (e.g. right acoustic neuroma, right SSHL, right Meniere's):
- Rinne: POSITIVE on the affected (right) ear (AC > BC — but BOTH are reduced; AC still wins because ossicular mechanism is intact)
- Weber: Lateralises AWAY from the affected ear — i.e. TO the LEFT (better) ear
- ABC: REDUCED on the affected side (cochlea damaged)
The false-negative Rinne (total/dead ear) — the critical exception:
When a patient has COMPLETE loss of cochlear function on one side (dead ear), a Rinne test appears to give a NEGATIVE result even though the cochlea is destroyed. Why? When the fork base is placed on the mastoid of the dead ear, the BC vibration crosses the skull and is perceived by the INTACT CONTRALATERAL cochlea. The patient reports hearing the bone-placed fork (from the contralateral cochlea), then stops hearing the air-placed fork (which cannot reach the contralateral cochlea by air). This mimics a negative Rinne (BC > AC) — falsely suggesting conductive loss when in fact the ear is dead (profound SNHL). This is the false-negative Rinne — it is also called Rinne negative in a dead ear or a 'false negative.' To exclude it, if the Rinne appears negative but otoscopy is normal (no structural cause for conductive loss), a masking test (Weber or formal audiometry with contralateral masking) is required.
Tympanic Membrane Assessment: Normal Findings and Abnormal Patterns
The tympanic membrane examination with the otoscope yields a specific set of findings that, when systematically recorded and interpreted, directly distinguish CSOM types, acute otitis media, otitis media with effusion, and other conditions. The most important interpretive distinction — safe vs unsafe TM — was introduced in the examination workflow SDL; here it is developed in clinical detail.
Normal TM appearance: pearly grey, semi-translucent, taut, with a bright cone of light reflex in the antero-inferior quadrant. The handle of malleus is visible through the TM as a yellowish-white streak. The pars flaccida is a small, slightly less tense area in the superior-most part of the TM above the malleolar folds. A normal TM is mobile on pneumatic otoscopy (Siegle's speculum).
Key abnormal TM findings and their significance:
| TM finding | Clinical significance |
|---|---|
| Central perforation (surrounded by intact pars tensa on all sides) | CSOM tubotympanic (safe) type — mucosa involved, no cholesteatoma |
| Attic perforation (in pars flaccida, superior) | CSOM atticoantral (unsafe) type — high risk of cholesteatoma, bone erosion, intracranial complications |
| Marginal perforation (reaching the annulus, no intact rim) | Also unsafe type — similar risk to attic perforation |
| Posterosuperior retraction pocket | Early/established cholesteatoma — especially if keratin debris visible |
| Bulging, red, loss of light reflex | ASOM — pus under pressure in the middle ear; myringotomy indicated at antero-inferior quadrant if no spontaneous rupture |
| Dull, retracted TM, absent or displaced light reflex | Eustachian tube dysfunction / secretory otitis media (glue ear) — TM sucks in due to negative middle ear pressure |
| Chalky white patches (calcification in TM) | Tympanosclerosis — sequela of repeated otitis media; may cause conductive hearing loss |
| Reduced mobility on pneumatic otoscopy | Fluid in middle ear (otitis media with effusion — 'glue ear') OR perforation (unrestricted movement) |
| Air-fluid level or bubbles visible through TM | Otitis media with effusion — fluid partially filling the middle ear |
Diagrammatic representation of TM findings (EN2.5 skill): The standard method is to draw a circle representing the TM, with a vertical line representing the handle of malleus, a small process anterosuperiorly (short process), and the umbo at the centre. The perforation is drawn as an opening of appropriate size and position. Annotate: 'R' or 'L' for the ear; 'safe/tubotympanic' or 'unsafe/atticoantral' for the type; 'central' or 'attic/marginal' for the perforation position.
CLINICAL PEARL
The Rinne test interpretation trap that catches every third student: Rinne POSITIVE does NOT mean 'better hearing' or 'normal hearing' — it means AC > BC, which is the result in BOTH normal hearing AND sensorineural hearing loss. A patient with profound sensorineural hearing loss will still have a Rinne POSITIVE because, even though both AC and BC are severely reduced, the ossicular chain is intact and continues to provide its mechanical advantage over direct skull BC. The only time Rinne becomes NEGATIVE (BC > AC) is when the ossicular/middle ear mechanism is impaired — i.e. conductive loss. So: 'Positive Rinne tells you the middle ear is working; it says nothing about the cochlea.' The cochlea's status is revealed by the ABC test and the Weber lateralisation.