Page 1 of 23
EN4.3 | Acute Suppurative Otitis Media — SDL Guide
Learning Objectives
- Elicit and document a structured history in a patient presenting with features of ASOM, identifying the stage of disease
- Describe the clinical features and otoscopic findings at each stage of ASOM
- Choose appropriate investigations for ASOM including tuning-fork tests, tympanometry, and culture
- Describe the principles of medical and surgical management of ASOM, including the indication and correct quadrant for myringotomy
INSTRUCTIONS
Acute suppurative otitis media is the most common cause of ear pain in children and a frequent presentation in paediatric out-patient practice across India. Understanding its staged progression — from Eustachian tube dysfunction through to suppuration and potential complication — allows you to match your management to the pathophysiological stage. This module is especially important because undertreated or mismanaged ASOM is the commonest precursor of chronic suppurative otitis media (CSOM), a major cause of preventable childhood hearing impairment.
References
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th edition, Ch 5 (Diseases of Middle Ear) (textbook)
- Hazarika P — Textbook of ENT and Head and Neck Surgery, 3rd edition, Ch 8 (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th edition, Vol 2 (Otology) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 11 PM and a frantic mother brings her 4-year-old son to your emergency room. He has been crying inconsolably for 3 hours with severe right ear pain, pulling at the ear repeatedly. He had a cold and runny nose 5 days ago that seemed to be getting better, but tonight he developed a fever of 39.2°C and became inconsolable. He has not eaten all evening. On otoscopy you see a bright red, bulging tympanic membrane with complete loss of the cone of light and the handle of the malleus is barely visible. What is happening in the middle ear at this moment, what stage has this child reached, and what is your immediate management decision?
WHY THIS MATTERS
Acute suppurative otitis media (ASOM) is the commonest bacterial infection of the middle ear and one of the most frequent diagnoses in paediatric practice worldwide. In India, it carries added significance because of overcrowded living conditions, high rates of upper respiratory tract infections, nutritional deficiencies affecting mucosal immunity, and limited access to follow-up care — all of which increase the risk of progression from ASOM to chronic middle ear disease. ASOM is the single most common reason for antibiotic prescription in children under five years globally. For you as a clinician, ASOM matters because it is common (you will see it in every practice setting), it is staged (management must match the pathological stage), missed or undertreated ASOM can cause acute complications such as mastoiditis, meningitis, and facial palsy as well as chronic consequences including CSOM and permanent conductive hearing loss, and the myringotomy — a simple surgical procedure with a specific safe quadrant — can provide immediate pain relief and drainage when needed. Competency EN4.3 requires you to be able to take a full history, describe clinical findings, choose investigations, and describe management principles at SH level.
RECALL
Before examining ASOM, recall the relevant anatomy from your Year-1 studies. The Eustachian tube connects the nasopharynx to the middle ear cleft and has three critical functions: ventilation (maintaining equal air pressure on both sides of the tympanic membrane), drainage of middle ear secretions into the nasopharynx, and protection from nasopharyngeal pathogens and sound pressure. In adults it is 35–37 mm long and angles downward at about 45° from horizontal; in children under 7 years it is shorter (approximately 17–18 mm), more horizontal, and floppier — all of which explain why ASOM is so much more common in children. The tympanic membrane (eardrum) is divided into four quadrants by imaginary lines through the handle of the malleus (vertical) and the umbo (horizontal): anterosuperior, anteroinferior, posterosuperior, and posteroinferior. The cone of light is the triangular reflection in the anteroinferior quadrant, visible on otoscopy in a healthy ear. Recall also that the middle ear contains the three ossicles (malleus, incus, stapes) and is bounded above by the tegmen tympani and below by the floor overlying the jugular bulb — anatomy that determines the safe site for myringotomy.
Clinical Presentation of ASOM
The clinical presentation of ASOM is dominated by four cardinal features that reflect the underlying pathological stage: otalgia (ear pain), fever, hearing loss, and — in later stages once the tympanic membrane perforates spontaneously or is opened by myringotomy — otorrhoea (ear discharge). Eliciting a precise, structured history is the first and most important step in meeting EN4.3, and the key questions are organised around these four features alongside essential background context. Otalgia in ASOM is characteristically severe, throbbing, and unilateral; in young children who cannot verbalise pain it manifests as inconsolable crying, ear tugging, head rolling, and refusal to feed — recognising these non-verbal signs is a clinical skill in itself. The relationship between the onset of URTI symptoms and the ear pain is diagnostically significant: most ASOM episodes occur 3–7 days after the start of a cold or pharyngitis, as resolving nasal mucosal inflammation triggers Eustachian tube oedema and dysfunction. The pattern of sudden cessation of pain followed by the appearance of discharge is pathognomonic of spontaneous tympanic membrane perforation — students must recognise this temporal sequence rather than misinterpreting the discharge as worsening disease.
History of presenting illness — key questions:
- Duration and character of ear pain: severe, throbbing, unilateral; wakens children at night; did the pain suddenly cease and discharge appear (spontaneous perforation)?
- Fever: usually moderate to high (38.5–40°C); preceded by or concurrent with upper respiratory symptoms
- Discharge: if present — onset, character (watery vs mucopurulent vs frankly purulent), odour (CSOM discharge is more often offensive)
- Hearing loss: mild to moderate conductive type during active disease; young children may not complain directly
- Preceding URTI: recent cold, rhinitis, or sore throat — critical to establish the Eustachian route
- Recurrence: previous episodes suggest Eustachian tube dysfunction; raise the question of grommet insertion
- Age: ASOM peaks at 6–12 months and 4–7 years; bilateral ASOM under 2 years is more severe
- Associated red flags: vertigo (labyrinthine involvement), facial weakness (facial nerve involvement), post-auricular pain or swelling (mastoiditis)
Predisposing factors to document:
- Crèche or nursery attendance (increased respiratory pathogen exposure)
- Breastfeeding status (breast milk provides passive immunity; bottle-fed supine position introduces milk into the Eustachian orifice)
- Parental smoking (impairs mucociliary clearance)
- Immunodeficiency, cleft palate, Down syndrome (increased susceptibility)
- Winter season (URTI incidence highest)
On general examination: the child is typically pyrexial, irritable, and in pain. The mastoid region must be inspected and palpated for tenderness, oedema, or erythema — their presence raises the suspicion of mastoiditis.
Anatomy and Pathophysiology: Why the Middle Ear Gets Infected
ASOM arises when a combination of Eustachian tube dysfunction and upper respiratory mucosal infection allows nasopharyngeal pathogens to colonise the normally sterile middle ear cleft. Understanding the mechanism requires appreciating the Eustachian tube as both the route of infection and the primary defensive barrier. In adults, the tube is long (35–37 mm), narrow, and angles steeply downward — it is difficult for pathogens to ascend against gravity and the mucociliary escalator. In children, the tube is shorter (17–18 mm), more horizontal, and its cartilaginous portion is floppier, meaning it collapses more easily with negative pressure. This anatomical difference is the single most important reason why ASOM is predominantly a childhood disease. During an upper respiratory infection, the mucosal oedema spreads into the Eustachian tube lining, blocks the tube's lumen, and creates negative intratympanic pressure as the middle ear mucosa absorbs the existing air. Bacteria from the nasopharynx are then sucked into the middle ear by this negative pressure gradient — a mechanism called the aspiration theory.
Route of infection: The Eustachian tube route accounts for the vast majority of ASOM cases. Haematogenous spread is rare. Traumatic spread (through a perforated TM) occurs mainly in chronic ear disease.
Most common causative organisms:
- Streptococcus pneumoniae (commonest overall, ~30–35%)
- Haemophilus influenzae (~20–25%, mostly non-typeable strains)
- Moraxella catarrhalis (~15%)
- Streptococcus pyogenes (Group A, ~8–10%)
- Viral pathogens (RSV, rhinovirus, influenza) often precede or co-exist with bacterial infection
The four stages of ASOM (Dhingra's classification):
| Stage | Name | Pathological change | Key clinical feature |
|---|---|---|---|
| 1 | Tubal Occlusion | ET blockage → negative middle ear pressure → TM retraction | Retracted TM; mild otalgia; no pus |
| 2 | Pre-suppuration | Mucosal hyperaemia, oedema; serous transudate; bacterial invasion begins | Red TM; loss of cone of light; otalgia increasing |
| 3 | Suppuration | Pus under pressure → TM bulges; all landmarks lost | Bulging cherry-red TM; severe throbbing pain; fever peaks |
| 4 | Resolution / Complication | TM ruptures (or myringotomy) → pus drains, pain relieved; OR infection spreads | Perforation with discharge and pain relief; or complication |
The critical clinical decision point is at Stage 3: timely myringotomy or spontaneous rupture leads to resolution, while delayed management risks spreading infection.
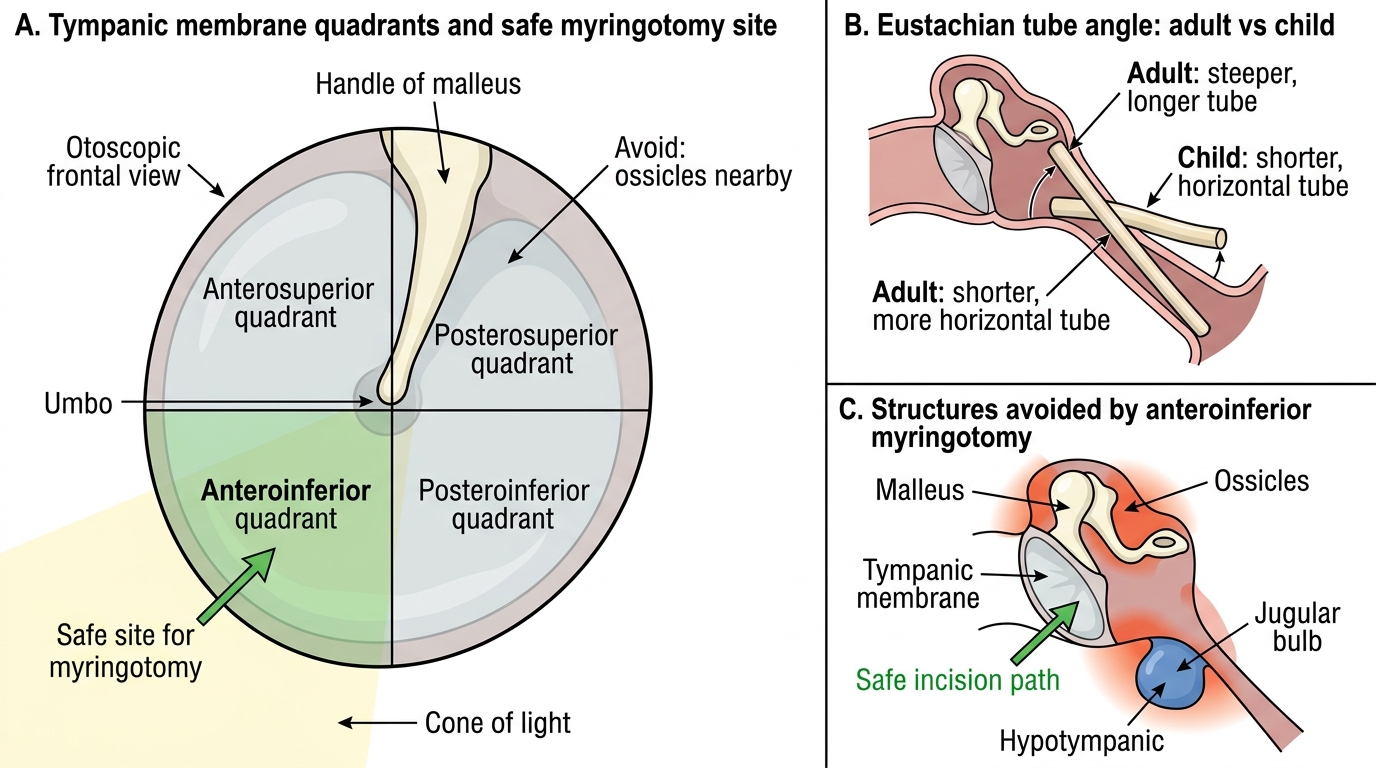
Safe Site for Myringotomy in the Tympanic Membrane
SELF-CHECK
A 3-year-old is brought with 2 days of left ear pain and fever. Otoscopy shows a diffusely red, mildly swollen tympanic membrane with early loss of the cone of light. No bulge. No discharge. Which stage of ASOM is this?
A. Stage 1 — Tubal occlusion
B. Stage 2 — Pre-suppuration
C. Stage 3 — Suppuration
D. Stage 4 — Resolution
Reveal Answer
Answer: B. Stage 2 — Pre-suppuration
Diffuse hyperaemia of the TM with loss of the cone of light but no bulging and no discharge is the hallmark of Stage 2 (Pre-suppuration). At Stage 1 the TM is retracted without hyperaemia; at Stage 3 there is frank bulging with maximal otalgia; Stage 4 involves perforation and discharge with pain relief.
Otoscopic Examination and Investigations
The otoscopic examination is the clinical cornerstone of ASOM diagnosis and staging. A systematic approach begins with the external auditory canal: inspect for wax, foreign bodies, or canal wall oedema (the last would suggest otitis externa as the primary diagnosis rather than ASOM). Then examine the tympanic membrane systematically under a bright light source. Identifying the normal TM landmarks is the prerequisite step — because recognising ASOM requires knowing exactly what has changed. The normal TM has a visible handle of malleus as a white vertical streak, the umbo at its lower end, a triangular cone of light reflection anteroinferiorly (produced by the flat, tensioned membrane reflecting the otoscope beam), and the pars flaccida superiorly above the lateral process. In ASOM, these landmarks are systematically lost as the stages progress: the cone of light disappears first (Stage 2), then the handle of malleus becomes obscured as the TM bulges outward (Stage 3), and perforation changes the appearance entirely (Stage 4). Equally important is identifying normal landmarks on the UNAFFECTED ear — this calibrates the examiner's baseline and aids comparison.
Otoscopic findings by ASOM stage:
- Stage 1: TM retracted; handle of malleus appears more horizontal and prominent; cone of light displaced or absent; mild vascular injection along the malleus
- Stage 2: Diffuse TM hyperaemia with visible vessels; early fullness; cone of light lost; mucosal swelling
- Stage 3: TM bulges outward (convex profile); cherry-red or yellow-red colour; ALL landmarks (cone of light, handle of malleus) obscured by pus tension — the most dramatic finding
- Stage 4: Small perforation visible in the pars tensa (usually central); mucopurulent or purulent discharge in the canal; TM hyperaemia begins to subside after drainage
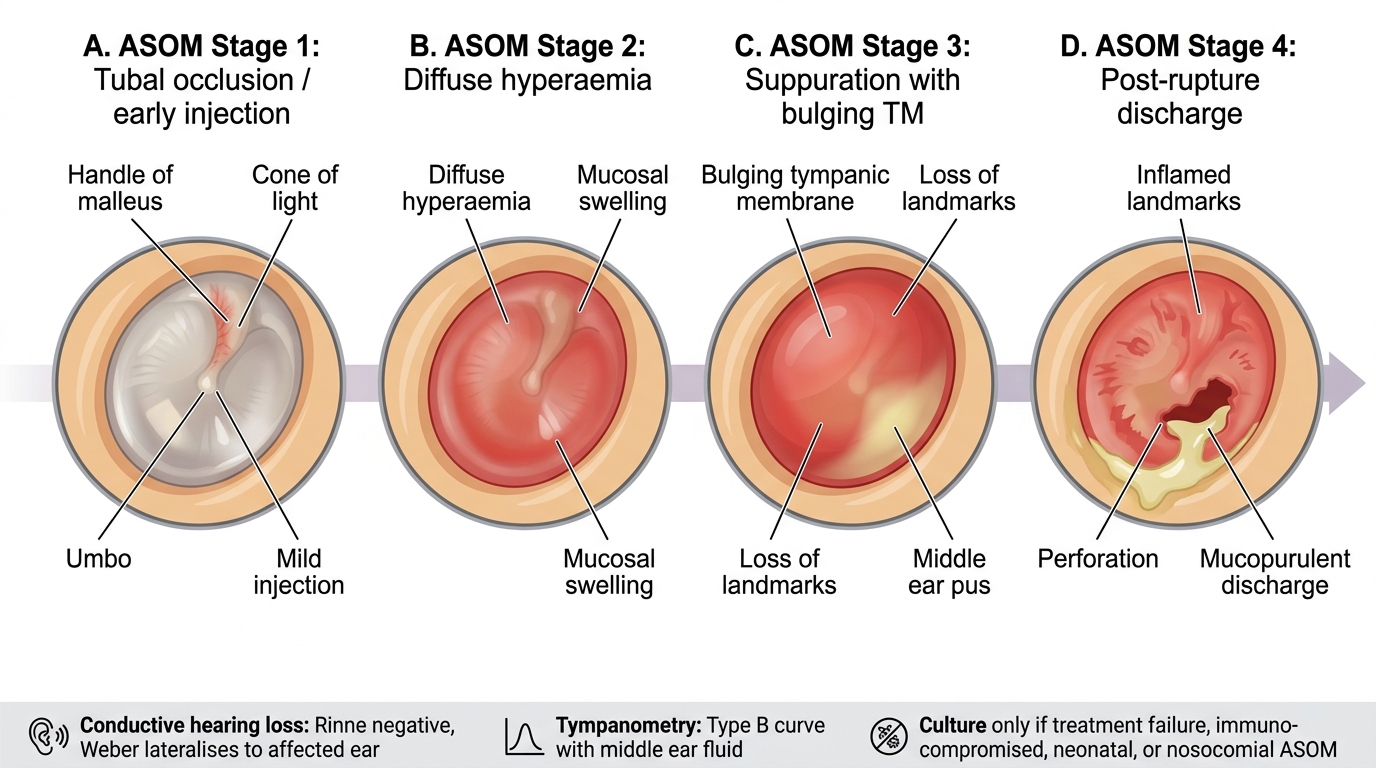
Otoscopic Stages of Acute Suppurative Otitis Media
Hearing assessment:
- Tuning fork tests (512 Hz): ASOM with middle ear fluid causes conductive hearing loss. Rinne test: negative (BC > AC) on the affected ear — bone conduction bypasses the fluid-filled middle ear. Weber test: lateralises to the affected ear — the diseased ear has a better bone-to-air ratio, so the midline vibration is perceived louder there. These findings confirm unilateral conductive loss.
- Pure-tone audiometry (PTA): Not routine in uncomplicated acute ASOM; useful for confirming hearing recovery, detecting residual effusion post-treatment, or investigating suspected mixed/sensorineural loss
- Tympanometry: Type B (flat) curve in the presence of middle ear fluid; normal Type A after resolution. Useful when TM findings are equivocal — especially to distinguish resolved ASOM from persistent OME
Microbiological investigation:
- Not routinely required for uncomplicated ASOM in immunocompetent children
- Culture of middle ear discharge indicated when: (1) treatment failure after 48–72 hours, (2) immunocompromised patient, (3) neonatal ASOM, (4) nosocomial ASOM
- Source: myringotomy aspirate (most reliable) or spontaneous discharge swab