Page 2 of 23
EN4.3 | Acute Suppurative Otitis Media — SDL Guide (Part 2)
Diagnosis and Differential Diagnosis
The diagnosis of ASOM is primarily clinical, based on the combination of acute onset symptoms and characteristic otoscopic findings. No single finding is pathognomonic — the diagnosis requires integrating the history (acute ear pain, fever, preceding URTI), the systemic examination (febrile, irritable child), and the otoscopic appearance (stage-specific TM changes) into a coherent clinical picture. A critical conceptual point for ENT assessment is that otoscopy must be used to stage the disease, not merely to confirm that the ear is infected — because the stage drives the management decision. A student who can describe the TM appearance and correctly assign the stage is demonstrating a higher level of competence than one who simply diagnoses ASOM and prescribes antibiotics without staging.
Diagnostic criteria for ASOM (Dhingra/AAP-aligned):
1. Acute onset (less than 3 weeks duration)
2. Middle ear inflammation: otalgia, fever, or irritability in young children
3. Middle ear effusion: bulging TM, limited TM mobility on pneumatic otoscopy, air-fluid level, or otorrhoea
All three criteria should ideally be met. Limited TM mobility on pneumatic otoscopy is the most sensitive sign for effusion but is frequently omitted in practice.
Differential diagnosis — the four most important:
1. Otitis Media with Effusion (OME / Glue Ear): Chronic (weeks to months) non-suppurative fluid in the middle ear WITHOUT acute inflammation. No fever, no severe otalgia; TM is retracted, dull, amber or grey-blue in colour — NOT red, NOT bulging. Hearing loss is the dominant complaint (noticed by parents or teacher). Tympanometry Type B confirms effusion. Managed by watchful waiting for 3 months then surgical review.
2. Otitis Externa (OE): Infection of the external auditory canal skin. Distinguished from ASOM by tragal tenderness (pain on pressing the tragus) and pinna traction pain — absent in ASOM. Canal wall is oedematous; TM is usually normal when visible. Tympanometry Type A (normal compliance) if TM intact. Treatment: topical ciprofloxacin ear drops + ear wicking.
3. Bullous Myringitis: Painful haemorrhagic or serous bullae on the TM surface — caused by Mycoplasma pneumoniae or viral infections. Very painful; TM has discrete bullae rather than uniform bulging. No purulent middle ear effusion under pressure. Management: analgesics; erythromycin for Mycoplasma coverage.
4. Referred Otalgia: Ear pain from non-ear sources transmitted via sensory nerve overlap (CN V3 auriculotemporal, CN IX, CN X, lesser occipital C2). Sources: dental disease, temporomandibular joint, tonsillitis, pharyngeal or laryngeal pathology. Key sign: normal otoscopy with ear pain → examine the oral cavity, throat, and neck to find the source.
SELF-CHECK
A 6-year-old girl has had mishearing in class for 8 weeks. No fever, no ear pain. Otoscopy shows a dull, amber-coloured, retracted left TM. Tympanometry is Type B. The correct diagnosis and management is:
A. Acute suppurative otitis media — start oral amoxicillin immediately
B. Otitis media with effusion — watchful waiting for 3 months before considering surgery
C. Otitis externa — prescribe ciprofloxacin ear drops
D. Sensorineural hearing loss — refer for audiological assessment and hearing aid
Reveal Answer
Answer: B. Otitis media with effusion — watchful waiting for 3 months before considering surgery
Chronic hearing loss without pain or fever, a dull amber retracted TM, and Type B tympanometry are diagnostic of OME (glue ear). OME is non-suppurative and chronic — antibiotics are not indicated. Standard management is watchful waiting for at least 3 months; surgical intervention (myringotomy + grommet) is considered if the effusion persists with significant bilateral hearing loss affecting school performance. SNHL would show a normal TM with audiometric bone conduction threshold elevation — not the case here.
Principles of Management and Myringotomy
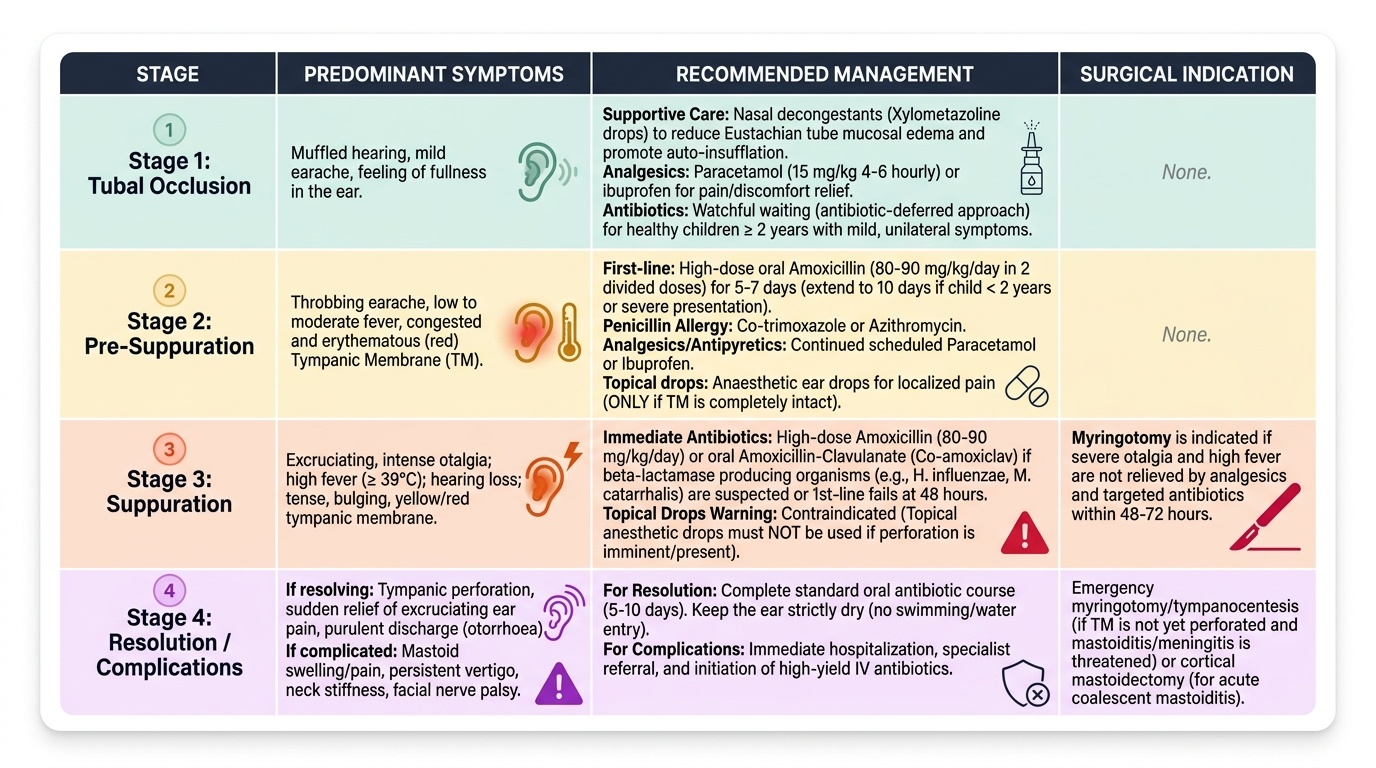
Management of ASOM is stage-guided: the choice between watchful waiting, antibiotic therapy, and surgical intervention (myringotomy) depends on the stage of disease, the severity of symptoms, the age of the patient, and the response to initial treatment. The underlying principles are to control infection, relieve pain and pressure, restore hearing, and prevent complications. A common error among students is to treat ASOM as a single entity requiring a uniform antibiotic course: in reality, mild ASOM in an older child may resolve without antibiotics (watchful waiting is an evidence-based approach), while Stage 3 ASOM in a young febrile child requires immediate antibiotics and may need surgical drainage. Understanding the age-dependent risk profile — children under 2 years with bilateral ASOM have a significantly higher rate of complications and persistent effusion — is what drives the graduated management algorithm described below.
Provided image
General and supportive measures (all stages):
- Analgesics/antipyretics: Paracetamol (15 mg/kg 4–6 hourly) or ibuprofen; the most important immediate comfort measure regardless of whether antibiotics are started
- Nasal decongestants: Xylometazoline nasal drops to reduce Eustachian tube mucosal oedema and promote drainage (modest benefit but widely used)
- Ear drops: Topical anaesthetic drops provide short-term pain relief but do NOT treat infection; contraindicated if TM is perforated
- Rest and adequate fluid intake: Standard supportive care
Antibiotic therapy:
- First-line: Amoxicillin (oral, high-dose 80–90 mg/kg/day in 2 divided doses, or standard dose in mild disease) for 5–7 days (extend to 10 days in children <2 years or with severe disease)
- Penicillin allergy: Co-trimoxazole (trimethoprim-sulfamethoxazole) or azithromycin
- Treatment failure / beta-lactamase-producing organisms: Amoxicillin-clavulanate (co-amoxiclav) covers H. influenzae and M. catarrhalis that produce beta-lactamase
- Watchful waiting (antibiotic-deferred): Acceptable in children ≥2 years with mild unilateral ASOM and no red flags — prescribe a safety-net prescription and review at 48–72 hours. NOT recommended in children <2 years, bilateral ASOM, fever >39°C, or immunocompromised patients
Indications for myringotomy:
1. Stage 3 ASOM with severe otalgia not relieved by analgesics and antibiotics within 48–72 hours
2. Impending or actual complications (mastoiditis, facial palsy, labyrinthitis, meningitis)
3. Febrile convulsions in a young child with ASOM
4. Immunocompromised patient
5. When microbiological diagnosis is urgently needed (neonatal ASOM, treatment failure)
Myringotomy — the anteroinferior quadrant rule:
Myringotomy is a surgical incision of the tympanic membrane to drain middle ear pus or fluid. The incision MUST be made in the anteroinferior quadrant of the pars tensa — this is non-negotiable. The anatomical reasons are: (1) the handle of malleus and the ossicular chain (incus, stapes) lie superiorly — any superior incision risks ossicular injury; (2) the jugular bulb forms the floor of the hypotympanum posteroinferiorly — a posteroinferior incision can cause catastrophic venous haemorrhage if the jugular bulb is abnormally high-riding. A small radial incision (2–3 mm) is made in the anteroinferior quadrant under microscopic guidance, using local anaesthesia (EMLA cream topically) or general anaesthesia in young children. Pus drains immediately; suction evacuates the contents. In simple ASOM myringotomy, NO tube (grommet) is inserted — a grommet is placed only in recurrent ASOM or persistent OME.
Post-ASOM follow-up:
- Review at 2 weeks to confirm resolution and healing of any perforation
- Hearing assessment (PTA/tympanometry) at 6–8 weeks to detect residual effusion (OME)
- Persistent effusion beyond 3 months → consider grommets
- Recurrent ASOM (≥3 episodes in 6 months or ≥4 in 12 months) → refer for consideration of grommet insertion
CLINICAL PEARL
The anteroinferior quadrant rule for myringotomy must be memorised without exceptions: superiorly lie the ossicles (malleus, incudostapedial joint); posteroinferiorly lies the jugular bulb. A posterosuperior incision risks entering the stapes footplate or dislocating the incus-stapes joint; a posteroinferior incision in a patient with a high-riding jugular bulb can cause catastrophic venous haemorrhage. The second pearl: when a parent reports that their child's severe earache suddenly stopped and was immediately followed by discharge, this is spontaneous perforation — reassure them it is therapeutic drainage, NOT worsening disease. Treat with antibiotics and ear hygiene; the perforation usually heals within 2–4 weeks.
Self-Assessment: Key Concepts in ASOM
Before testing yourself on the micro-quiz questions below, consolidate the core concepts of this module by reviewing the following framework. ASOM is a staged disease — the ability to assign a stage from the history and otoscopy finding, and then match the management to that stage, is the central clinical skill being assessed in EN4.3. Stage 1 (tubal occlusion with TM retraction) and Stage 2 (pre-suppuration with TM hyperaemia) are typically managed conservatively with analgesia and antibiotics; Stage 3 (suppuration with bulging TM) may require myringotomy if symptoms persist beyond 48–72 hours or if complications are imminent; Stage 4 (resolution after perforation or myringotomy) requires antibiotic completion, ear hygiene, and follow-up to confirm perforation healing and hearing recovery. The tuning fork findings in active ASOM — Rinne negative on the affected side, Weber lateralising to the affected ear — confirm conductive hearing loss and are a direct consequence of middle ear fluid impeding air-conducted sound. The critical safety rule that underpins the entire surgical section is that myringotomy must always be performed in the anteroinferior quadrant, avoiding the ossicular chain superiorly and the jugular bulb posteroinferiorly. Ensuring that you can articulate WHY the anteroinferior quadrant is safe — not merely that it is — distinguishes understanding from rote memorisation.
Key facts to consolidate:
- Four stages of ASOM and their TM appearance at each stage
- Most common causative organisms: S. pneumoniae, H. influenzae, M. catarrhalis
- First-line antibiotic: amoxicillin
- Safe myringotomy quadrant: anteroinferior
- Tuning forks: Rinne negative (affected ear), Weber to affected ear = conductive loss
- Key differentials: OME (chronic, no fever, amber TM), OE (tragal tenderness, normal TM), referred otalgia (normal otoscopy)
- Post-ASOM follow-up at 6–8 weeks for residual effusion detection
SELF-CHECK
During myringotomy for Stage 3 ASOM, the incision must be made in which quadrant, and what two anatomical structures does this placement avoid?
A. Posteroinferior quadrant — avoids the handle of malleus and the chorda tympani
B. Anterosuperior quadrant — avoids the Eustachian tube opening and the facial nerve
C. Anteroinferior quadrant — avoids the ossicular chain (superiorly) and the jugular bulb (posteroinferiorly)
D. Posterosuperior quadrant — avoids the facial nerve canal and the annulus fibrosus
Reveal Answer
Answer: C. Anteroinferior quadrant — avoids the ossicular chain (superiorly) and the jugular bulb (posteroinferiorly)
The anteroinferior quadrant is the universally accepted safe site for myringotomy. Superiorly lie the handle of malleus and the ossicular chain (incus, stapes); any superior incision risks ossicular damage and potential hearing impairment. Posteroinferiorly lies the jugular bulb, which can be abnormally high-riding in some patients; a posteroinferior incision risks jugular vein injury with catastrophic haemorrhage. The anteroinferior quadrant avoids both hazards. Drainage is achieved regardless of site because pus under pressure flows to any opening.